
Neglected pediatric Kaplan’s MCP dislocations can be successfully treated with volar open reduction, which allows direct release of the fibrotic volar plate and restoration of joint stability even in long-standing cases.
Dr. Siddhant Pundalik Pol, Department of Orthopedics, LTMMC and Sion Hospital, Mumbai, Maharashtra, India. E-mail: siddhantpol@gmail.com
Abstract
Introduction: Kaplan’s dislocation is a rare complex metacarpophalangeal (MCP) joint dislocation in which soft-tissue interposition prevents closed reduction. Chronic neglected cases in children are extremely uncommon and present significant diagnostic and therapeutic challenges.
Case Report: We report the case of an 11-year-old left-hand-dominant boy who presented with deformity and restricted motion of the left index finger 8 years after childhood trauma. Radiographs demonstrated a chronic dorsal dislocation of the second MCP joint consistent with Kaplan’s lesion. An initial attempt at closed reduction with distraction failed to maintain reduction. Open reduction through a volar approach revealed dense fibrosis of the volar plate and capsule acting as the mechanical block to reduction. After release and repair of these structures, stable reduction was achieved and maintained using transarticular K-wire fixation. At 6-month follow-up, the patient regained full range of motion with good pincer grip and no residual instability.
Conclusion: Neglected pediatric Kaplan’s MCP dislocations are rare but can be successfully treated with volar open reduction, which allows direct visualization and release of obstructing volar structures, leading to excellent functional outcomes.
Keywords: Kaplan dislocation, metacarpophalangeal joint, pediatric hand injury, chronic metacarpophalangeal dislocation, volar open reduction.
Metacarpophalangeal (MCP) joint dislocations account for approximately 5% of upper extremity injuries among the pediatric population, especially in children <5 years of age [1]. Kaplan’s lesions are rare complex MCP dislocations in which soft-tissue interposition prevents closed reduction. Simple Kaplan’s dislocations are treated by closed reduction, whereas complex dislocations require open reduction [2]. The pathoanatomy of Kaplan’s lesion involves entrapment of the metacarpal head by surrounding soft tissues. The superficial transverse metacarpal ligament lies proximally, while the flexor tendons with pre-tendinous bands lie on the ulnar side and the lumbrical muscle lies on the radial side. Distally, the metacarpal head becomes buttonholed between the natatory ligament and the volar plate, creating a constricting soft-tissue noose that prevents closed reduction [3]. A simple dislocation can become complex if there are multiple failed closed reduction attempts. While a dorsal approach with open reduction is commonly recommended in acute cases, the volar approach may provide full exposure of the volar plate, facilitating management of osteochondral fractures with decreased risk to palmarly displaced neurovascular structures. However, to achieve sufficient reduction, the dorsal method necessitates separating the volar plate, which might delay recovery [4]. We report a unique case of an 8-year neglected chronic Kaplan’s dislocation of the second MCP joint, successfully treated using a volar open reduction approach after failed closed reduction.
Patient information
An 11-year-old left-hand-dominant boy presented in June 2025 with a 6-month history of pain and deformity of the left index finger. He had sustained trauma to the same digit at 3 years of age, which had been managed conservatively without orthopedic evaluation. There was no history of recent trauma, infection, or other medical comorbidities. Clinical examination revealed a visible dorsal deformity of the left index finger with mild tenderness over the MCP joint. The joint was rigid and non-reducible, with a painful and restricted range of motion (Fig. 1a, b, c, d).
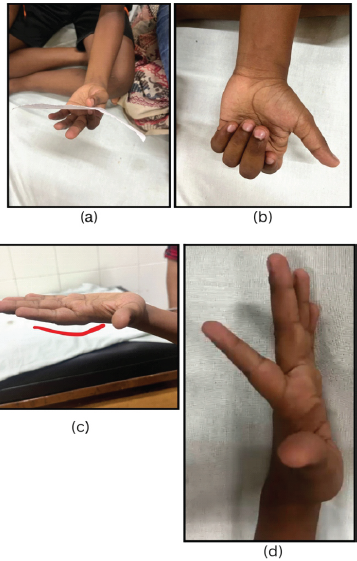
Figure 1: (a, b, c, d) Weak pincer grip of the left hand. The patient is unable to make a fist using the left hand. Dorsal bump deformity of the second digit. Hyperextension of the second digit.
Distal neurovascular status was intact. Plain radiographs demonstrated dorsal dislocation of the left index MCP joint consistent with a chronic Kaplan’s dislocation (Fig. 2a and b). A schematic representation of the anatomical configuration responsible for Kaplan’s lesion is illustrated in Fig. 2c.
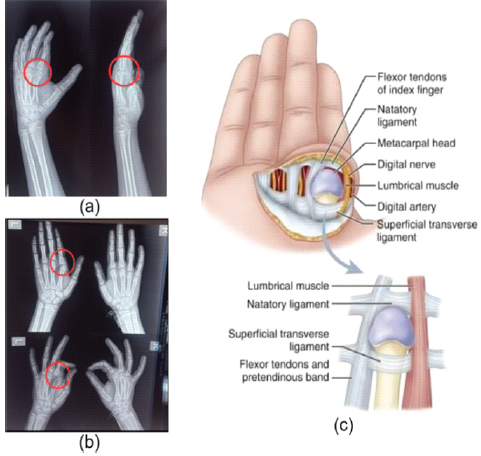
Figure 2: (a and b) Anteroposterior and lateral view radiographs of the left hand showing a dislocated second metacarpophalangeal (MCP) joint. Radiograph showing comparison between the unaffected right side and the affected left side in both anteroposterior and oblique views to confirm dislocation of the left second MCP joint. (c) Schematic illustration demonstrating the anatomical configuration in Kaplan’s lesion showing the flexor tendons, lumbrical muscle, natatory ligament, superficial transverse ligament, and digital neurovascular bundle forming a constricting noose around the metacarpal head.
Closed reduction with external fixation using a finger distractor was planned to facilitate gradual soft-tissue lengthening. Under fluoroscopic guidance, closed reduction was performed. Two K-wires were inserted into the metacarpal and two into the proximal phalanx of the left index finger, and a finger distractor was applied across the MCP joint. Adequate joint distraction and acceptable reduction were achieved intra-operatively.
However, fixation failed due to loosening of the metacarpal-side pins. The distractor and K-wires were removed, and a cock-up splint was applied for 15 days to allow pin-tract healing and pain control. Follow-up radiographs, however, demonstrated persistent MCP dislocation, with no clinical or radiological evidence of maintained reduction. One month later, open reduction and internal fixation were performed. Under general anesthesia with tourniquet control, a volar approach was used through a 3-cm L-shaped incision over the volar aspect of the MCP joint (Fig. 3a and b). The flexor digitorum superficialis and flexor digitorum profundus tendons and the digital neurovascular bundles were identified and protected. The hypertrophic capsule and markedly thickened volar plate were identified as the principal mechanical block to reduction and were released. The hypertrophic capsule and markedly thickened volar plate were identified as the principal mechanical block to reduction and were released (Fig. 3c). The obstructing volar plate tissue was excised from the joint space, followed by capsular and volar plate repair using absorbable 3-0 Vicryl sutures. Stable reduction was achieved and maintained with transarticular K-wire fixation (Fig. 3d). The wound was closed in layers and a cock-up splint was applied. The wound was closed in layers, and a cock-up splint was applied.
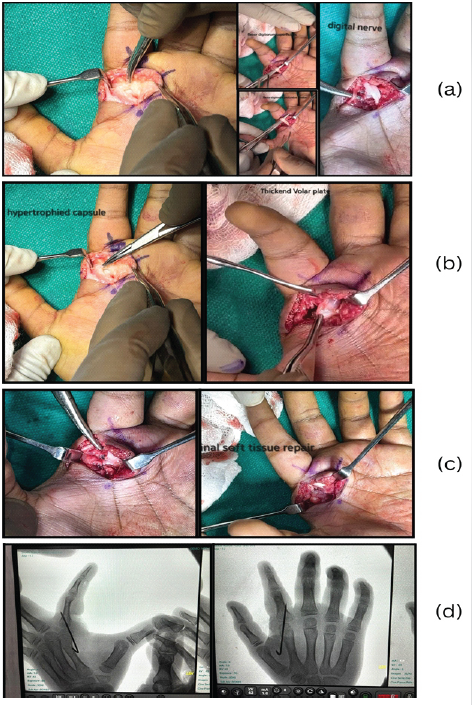
Figure 3: (a, b, c, d) 3 cm L-shaped incision using volar approach with identification of flexor digitorum profundus and flexor digitorum superficialis Tendon with digital nerve. Hypertrophied capsule and thickened volar plate. Final soft tissue repair of volar plate and capsule with 3-0 Vicryl sutures. Final fixation and intraoperative C-arm image confirming reduced joint.
The post-operative course was uneventful. Immobilization was maintained for 20 days, after which the K-wires and sutures were removed. Active range-of-motion exercises of the wrist and fingers were initiated following splint removal and continued for 2 months. At 6-month follow-up, radiographs confirmed stable reduction and the patient regained a full range of motion with good pincer grip (Fig. 4a-d). No residual pain, neurovascular compromise, skin puckering, or recurrent dislocation was observed. No residual pain, neurovascular compromise, skin puckering, or recurrent dislocation was observed.
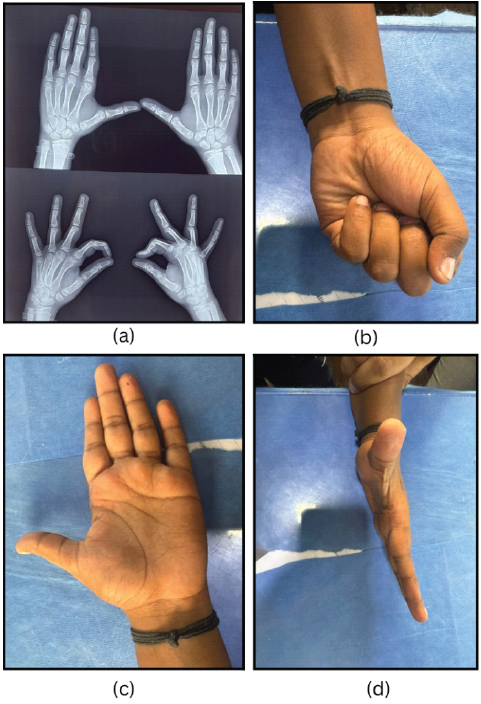
Figure 4: (a, b, c, d) 6 months post-operative plain radiograph showing reduced congruent metacarpophalangeal joint. Patient making a fist with the left hand. Well-healed scar with no skin puckering. Correction of the dorsal bump deformity of the left second digit.
Kaplan’s dislocations are complex MCP joint dislocations typically caused by hyperextension trauma and most commonly involve the index finger in young children [5]. Closed reduction frequently fails because of interposition of the volar plate and surrounding soft tissues, which constitute the principal mechanical block to reduction. Previous literature reviews have described the characteristic anatomical configuration and management principles of complex MCP dislocations, emphasizing the importance of recognizing the soft-tissue “noose” mechanism around the metacarpal head [6,7,8].Several case reports have described successful treatment of complex MCP dislocations using open reduction through dorsal approaches, particularly in acute cases [8,9]. Standard hand surgery texts also describe the volar plate and surrounding soft-tissue structures as the principal block to reduction in complex MCP dislocations [10]. Important differences between pediatric and adult complex MCP dislocations include the absence of fully developed sesamoid bones and the presence of osteochondral injury at the metacarpal head near the collateral ligament insertions [5,6]. Dorsal open reduction is widely described for acute Kaplan’s dislocations and is associated with favorable outcomes when performed early. However, in neglected or chronic cases, long-standing fibrosis of the capsule and volar plate may limit dorsal exposure and prevent adequate release of the obstructing structures. In the present patient, the dislocation had persisted for 8 years, resulting in dense fibrosis of the volar plate and periarticular tissues. A volar approach enabled direct visualization and complete release of the fibrotic volar plate and capsule, facilitating stable reduction and repair. Long-standing MCP dislocations in children are associated with risks of stiffness, degenerative changes, and potential growth disturbance. Early mobilization following stable fixation is therefore essential to achieve optimal functional recovery. This case demonstrates that the volar approach provides superior visualization and release of fibrotic volar plate and capsular structures compared with the dorsal approach and may be particularly effective in long-standing neglected pediatric Kaplan’s dislocations. Reports describing the successful treatment of pediatric Kaplan’s dislocations, neglected for several years, are extremely limited in the literature, with most published cases representing acute or subacute presentations. To our knowledge, this represents one of the longest-standing neglected pediatric Kaplan MCP dislocations of the index finger successfully treated using a volar open-reduction approach with good functional outcome.
Neglected pediatric Kaplan’s dislocations of the MCP joint are rare and may present many years after the initial injury. In chronic cases, fibrosis of the volar plate and periarticular tissues often prevents closed reduction. A volar open approach provides direct visualization of the obstructing structures, facilitates adequate release and repair, and allows stable reduction of the joint. Early post-operative mobilization following stable fixation can result in excellent functional recovery even in long-standing neglected cases.
Neglected pediatric Kaplan’s dislocations of the MCP joint can present with dense volar fibrosis that prevents closed reduction. A volar open approach allows direct release of obstructing structures and can achieve stable reduction with excellent functional outcome even in long-standing cases.
References
- 1. Lee A, Colen DL, Fox JP, Chang B, Lin IC. Pediatric hand and upper extremity injuries presenting to emergency departments in the United States: Epidemiology and health care-associated costs. Hand (N Y) 2019;16:519-27. [Google Scholar] [PubMed]
- 2. Kaplan EB. Dorsal dislocation of the metacarpophalangeal joint of the index finger. J Bone Joint Surg Am 1957;39-A:1081-6. [Google Scholar] [PubMed]
- 3. Keshkar S, Biswas S. Kaplan’s dislocation in a child with delayed presentation: A case report. Int J Orthop Surg 2024;32:59-61. [Google Scholar] [PubMed]
- 4. Patterson RW, Maschke SD, Evans PJ, Lawton JN. Dorsal approach for open reduction of complex metacarpophalangeal joint dislocations. Orthopedics 2008;31:1099. [Google Scholar] [PubMed]
- 5. Durand Y, Rodriguez NN, Georgopoulos S, Mesoraca C, Jaën M. Complex metacarpophalangeal joint dislocation (Kaplan’s lesion) of the index finger in a 5-year-old patient: A case report. J Orthop Case Rep 2024;14:141-5. [Google Scholar] [PubMed]
- 6. Sumarriva G, Cook B, Godoy G, Waldron S. Pediatric complex metacarpophalangeal joint dislocation of the index finger. Ochsner J 2018;18:398-401. [Google Scholar] [PubMed]
- 7. Malisorn S. Dislocation of the metacarpophalangeal joint: A narrative review treatment and examination. Int J Res Orthop 2023;10:173-7. [Google Scholar] [PubMed]
- 8. Mahajan NP, Patil TC, Sangma S. Management of complex Kaplan’s dislocation by open dorsal approach – a case report. J Orthop Case Rep 2021;11:84-7. [Google Scholar] [PubMed]
- 9. Srivastava S, Afaque SF. Complex metacarpophalangeal joint dislocation of the index finger in pediatric age: A case report and review of literature. J Orthop Case Rep 2022;12:102-5. [Google Scholar] [PubMed]
- 10. Green DP, Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH. Green’s Operative Hand Surgery. 7th ed. Philadelphia, PA: Elsevier; 2017. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Management of a Rare Case of Complex and Irreducible Dislocation of the Metacarpophalangeal Joint in the Little Finger – A Case Report
June 1, 2025 Management of a Rare Case of Complex and Irreducible Dislocation of the Metacarpophalangeal Joint in the Little Finger – A Case Report March 10, 2024 Spontaneous Idiopathic Bilateral Sagittal Band Rupture: A Case Report
March 10, 2024 Spontaneous Idiopathic Bilateral Sagittal Band Rupture: A Case Report November 10, 2023 Metacarpal Joint Arthroplasty in the Acute Setting: A Case Report
November 10, 2023 Metacarpal Joint Arthroplasty in the Acute Setting: A Case Report December 10, 2022 Digital Arterial Occlusion at the Metacarpophalangeal Joint with Hypothenar Hammer Syndrome-like Symptoms: A Case Report
December 10, 2022 Digital Arterial Occlusion at the Metacarpophalangeal Joint with Hypothenar Hammer Syndrome-like Symptoms: A Case Report