
Persistent torticollis beyond 4 weeks after minor trauma in children should raise suspicion of fixed atlantoaxial rotatory subluxation requiring surgical stabilization.
Dr. Chirag Sharma, Department of Orthopaedics, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya, India. E-mail: chiragammu@gmail.com
Abstract
Introduction: Atlantoaxial rotatory subluxation (AARS) is an uncommon yet important cause of painful torticollis in children. While most acute cases respond to conservative management, delayed diagnosis may result in fixed and irreducible deformity requiring surgical stabilization. Chronic irreducible cases are rare and pose significant management challenges.
Case Report: A 9-year-old girl presented with persistent painful torticollis for 6 weeks following minor trauma. Clinical examination revealed a classic cock-robin posture with severely restricted cervical motion. Computed tomography confirmed fielding type II C1–C2 rotatory subluxation. Despite adequate conservative management, the deformity remained irreducible. Failure of conservative treatment and fixed deformity necessitated surgical intervention. Posterior C1 lateral mass and C2 pedicle screw fixation was performed. Intraoperative reduction was achieved, followed by rigid stabilization and fusion.
Conclusion: Chronic irreducible AARS in children requires early recognition and timely surgical stabilization. Posterior C1–C2 lateral mass fixation provides reliable correction and excellent functional outcomes.
Keywords: Atlantoaxial rotatory subluxation, C1–C2 instability, pediatric torticollis, posterior lateral mass fixation, fielding Type II, cervical spine surgery
Atlantoaxial rotatory subluxation (AARS) represents a spectrum of instability involving the C1–C2 complex and accounts for a significant proportion of cervical spine rotation in children [1]. Approximately 50% of cervical rotation occurs at the atlantoaxial joint, predisposing it to instability when ligamentous or muscular support is compromised. Children are particularly vulnerable due to increased ligamentous laxity, horizontal orientation of the facet joints and underdeveloped cervical musculature [2,3] AARS commonly follows minor trauma or upper respiratory infection and presents with painful torticollis and the classic cock-robin posture. Acute cases are often reducible with rest, analgesia, traction, or immobilization. However, delayed presentation may result in adaptive facet changes and persistent muscular spasm, leading to irreducible deformity that necessitates surgical stabilization [4,5,6]. We present a case of chronic irreducible C1–C2 rotatory subluxation in a child successfully treated with posterior lateral mass fixation.
A 9-year-old female presented with painful abnormal head posture persisting for 6 weeks following a minor fall while playing. There was no history of fever, upper respiratory infection, congenital cervical anomaly, or inflammatory disorder.
Clinical findings
The head was tilted to the right with rotation of the chin to the left, consistent with cock-robin posture (Fig. 1). Cervical motion was markedly restricted and painful in all directions. Spasm and tenderness were present over the upper cervical region. Neurological examination was normal.

Figure 1: Clinical photograph demonstrating fixed torticollis with lateral flexion of the head to the right and rotation of the chin to the left (cock-robin posture). Facial features have been anonymized.
Radiological examination
Plain radiographs demonstrated asymmetry of the lateral masses. Computed tomography (CT) scan confirmed Fielding Type II C1–C2 rotatory subluxation with anterior displacement of C1 (Fig. 2 and 3). Magnetic resonance imaging (MRI) showed persistent malalignment without spinal cord compression (Fig. 4).

Figure 2: Pre-operative anteroposterior cervical spine radiograph demonstrating asymmetry of the C1 lateral masses relative to C2, suggestive of atlantoaxial rotatory subluxation.
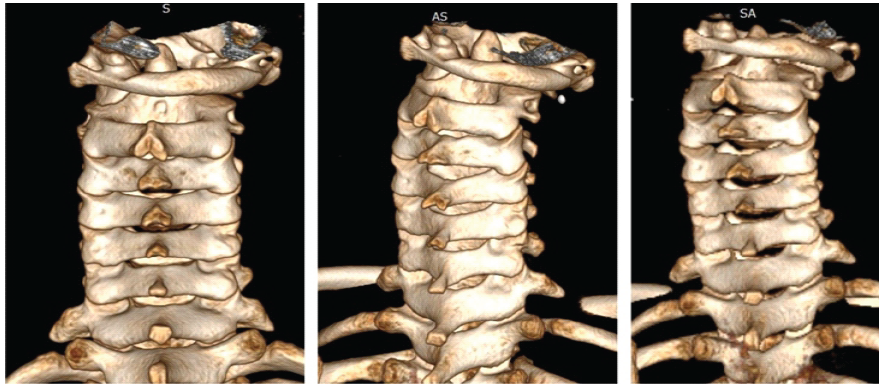
Figure 3: Pre-operative computed tomography scan with three-dimensional reconstruction showing persistent rotation of the atlas (C1) relative to the axis (C2), consistent with Fielding Type II atlantoaxial rotatory subluxation.
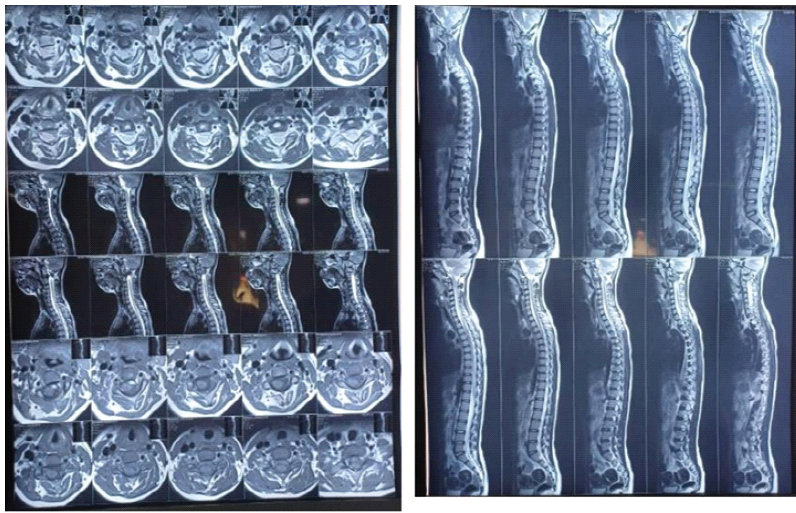
Figure 4: Pre-operative magnetic resonance imaging of the cervical spine showing atlantoaxial malalignment without evidence of spinal cord compression.
Given the chronicity of 6 weeks and imaging findings, the deformity was considered irreducible.
Management
Initial conservative management included analgesics, cervical immobilization and activity restriction. No meaningful correction was achieved. Given the fixed deformity and failure to achieve reduction with conservative measures, the subluxation was considered clinically irreducible and surgical stabilization was planned.
Surgical technique
Under general anesthesia, posterior exposure of C1–C2 was performed with careful preservation of the vertebral artery and C2 nerve root. The Harms technique was preferred over transarticular screw fixation due to improved safety profile in pediatric anatomy and reduced vertebral artery risk. C1 lateral mass screws and C2 pedicle screws were inserted bilaterally under fluoroscopic guidance. Gentle intraoperative manipulation achieved restoration of alignment before rod fixation. Reduction was confirmed fluoroscopically before final tightening of the construct. Autologous bone graft was applied to promote fusion. Rigid fixation allowed stable correction of the deformity.
Outcome and follow-up
Immediate post-operative correction of head posture was achieved. Pain resolved significantly within days. Neurological function remained intact. Follow-up radiographs and CT imaging demonstrated maintained alignment and stable hardware position (Fig. 5).
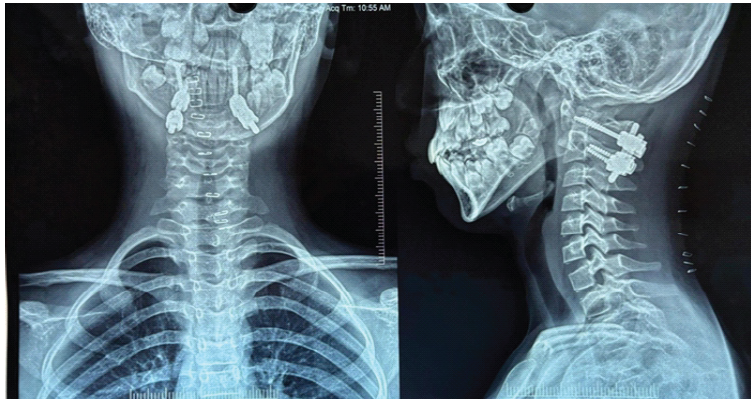
Figure 5: Post-operative anteroposterior cervical spine radiograph demonstrating bilateral C1 lateral mass and C2 pedicle screw fixation with restoration of atlantoaxial alignment and stable hardware position.
At final follow-up, the patient resumed normal daily activities without recurrence.
AARS in children typically responds to early conservative treatment [1,2]. However, delayed presentation beyond several weeks increases the likelihood of persistent muscle contracture and facet remodeling, rendering reduction difficult or impossible [4,5,6]. Fielding Type II injuries involve unilateral facet subluxation with anterior displacement of C1, often requiring more aggressive management when chronic. CT imaging remains the gold standard for diagnosis and classification, while MRI is essential to assess ligamentous integrity and neural elements [1,2,7]. In irreducible cases, surgical stabilization is indicated to prevent progressive deformity, avoid neurological compromise and provide definitive correction. Posterior C1–C2 screw-rod fixation, as described by Goel and later modified by Harms, has largely replaced older wiring and transarticular techniques due to superior biomechanical stability, higher fusion rates, and improved safety profile [8,9,10]. Only limited literature describes chronic irreducible AARS requiring posterior C1–C2 fixation in the pediatric population. Shousha et al. [10] reported satisfactory long-term outcomes with posterior screw fixation in chronic cases. Our case further supports that rigid screw-rod stabilization provides reliable reduction and maintenance of alignment even after delayed presentation. In pediatric patients, careful screw trajectory planning is essential due to smaller anatomical dimensions and vertebral artery proximity. This case highlights that chronic painful torticollis following minor trauma should raise suspicion for atlantoaxial instability. Delay in diagnosis may convert a reducible condition into one requiring operative management.
Persistent painful torticollis in children warrants early advanced imaging to exclude atlantoaxial instability. Chronic irreducible rotatory subluxation requires surgical stabilization for definitive management. Posterior C1–C2 lateral mass fixation provides reliable correction, neurological safety, and excellent functional outcomes.
Early CT evaluation is essential in children with fixed torticollis. Chronic irreducible atlantoaxial instability is best managed with rigid posterior fixation to prevent long-term deformity and neurological compromise.
References
- 1. Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation. (Fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am 1977;59:37-44. [Google Scholar] [PubMed]
- 2. Pang D, Li V. Atlantoaxial rotatory fixation: Part 2–New diagnostic paradigm and a new classification based on motion analysis using computed tomographic imaging. Neurosurgery 2005;57:941-53. [Google Scholar] [PubMed]
- 3. Brockmeyer D. Down syndrome and craniovertebral instability. Neurosurg Focus 1999;6:e1. [Google Scholar] [PubMed]
- 4. Phillips WA, Hensinger RN. The management of rotatory atlanto-axial subluxation in children. J Bone Joint Surg Am 1989;71:664-8. [Google Scholar] [PubMed]
- 5. Wetzel FT, La Rocca H. Grisel’s syndrome. Clin Orthop Relat Res 1989;240:141-52. [Google Scholar] [PubMed]
- 6. Martínez-Lage JF, Martínez Robledo A, Poza M. Atlantoaxial rotatory fixation in children: Early management. Childs Nerv Syst 2003;19:30-5. [Google Scholar] [PubMed]
- 7. Nunez DB, Zuluaga A. CT and MR imaging of odontoid abnormalities in children. Radiographics 1996;16:641-60. [Google Scholar] [PubMed]
- 8. Goel A, Laheri V. Plate and screw fixation for atlanto-axial subluxation. Acta Neurochir (Wien) 1994;129:47-53. [Google Scholar] [PubMed]
- 9. Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine (Phila Pa 1976) 2001;26:2467-71. [Google Scholar] [PubMed]
- 10. Shousha M, El-Saghir H, Boehm H. Surgical treatment of chronic atlantoaxial rotatory fixation in children: Long-term results. Spine J 2019;19:1190-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2022 An Isolated Displaced Coracoid Fracture Treated with Open Reduction Internal Fixation with 4 mm Cannulated Cancellous Screw
January 10, 2022 An Isolated Displaced Coracoid Fracture Treated with Open Reduction Internal Fixation with 4 mm Cannulated Cancellous Screw February 1, 2026 Functional Outcomes after Radial Shortening Osteotomy in Stage IIIA Kienböck’s Disease: A Five-Patient Case Series
February 1, 2026 Functional Outcomes after Radial Shortening Osteotomy in Stage IIIA Kienböck’s Disease: A Five-Patient Case Series October 14, 2014 The Acute and Chronic Presentation of Gluteus Medius Calcific Tendinitis- A Case Report of Two
October 14, 2014 The Acute and Chronic Presentation of Gluteus Medius Calcific Tendinitis- A Case Report of Two September 10, 2022 A Lumpy-Bumpy Painful Ankle – Trevor Disease of the Ankle in a 9-year-old
September 10, 2022 A Lumpy-Bumpy Painful Ankle – Trevor Disease of the Ankle in a 9-year-old