
Patient-specific three-dimensional (3D)-printed models enhance spatial understanding and fixation accuracy in complex scapular fractures and have broad applicability across orthopedics for optimizing reduction strategy, implant positioning, and surgical efficiency.
Dr. Jordan Dobrich, Madigan Army Medical Center Orthopaedics, Joint Base Lewis-McChord, WA, USA. E-mail: jordan.m.dobrich.mil@health.mil
Abstract
Introduction: Scapular fractures are relatively uncommon but pose significant challenges in high-energy polytrauma, particularly when complex comminuted patterns are present. Three-dimensional (3D) computed tomography (CT) reconstruction and 3D printing are emerging tools in orthopedics that enhance pre-operative planning and intraoperative decision-making. Although widely used in pelvic, acetabular, and distal radius fractures, their application in scapular fracture management remains limited.
Case Report: A 22-year-old active-duty male sustained polytrauma following a high-speed motorcycle collision, including a comminuted scapular body fracture with scapulothoracic dissociation and a transected branch of the suprascapular nerve to the supraspinatus. High-resolution CT imaging was used to generate a 3D reconstruction of the scapula, from which a full-scale, patient-specific 3D-printed model was created and sterilized for intraoperative reference. Open reduction and internal fixation was performed via a modified Judet approach using a 3.5-mm locking compression plate, a 2.0-mm T-plate, and a 3.5-mm cannulated screw for reduction of this complex fracture. The transected suprascapular nerve branch was repaired intraoperatively. Use of the sterilized 3D model improved spatial understanding of fracture morphology and facilitated accurate implant placement. Post-operative CT imaging confirmed anatomic reduction and optimal hardware positioning.
Conclusion: This case demonstrates the novel utility of sterilized 3D-printed models in the fixation of complex scapular fractures, an application infrequently described in the orthopedic literature. Patient-specific 3D models enhance intraoperative spatial orientation and facilitate precise hardware placement when fracture comminution and anatomic complexity limit interpretation of conventional imaging. This report supports extending the use of 3D modeling to scapular fractures in both military and civilian trauma settings.
Keywords: Scapular fracture, 3D printing, orthopedic trauma, surgical planning.
Scapular fractures are relatively uncommon injuries, but present substantial challenges in the setting of high-energy polytrauma, particularly when complex articular or comminuted patterns occur in young, active patients [1,2]. Traditional management has relied on radiographic evaluation and surgeon experience; however, advances in three-dimensional (3D) computed tomography (CT) reconstruction have significantly improved pre-operative characterization of fracture morphology and operative decision-making [1,2]. The integration of 3D printing technology into orthopedic trauma care has further enhanced both pre-operative planning and intraoperative execution. Patient-specific 3D-printed models derived from CT data provide tactile and visual feedback that improves understanding of complex anatomy, facilitates rehearsal of reduction maneuvers, and enables precise pre-contouring of fixation implants [3,4,5,6,7,8]. Prior studies have demonstrated reductions in operative time, intraoperative blood loss, and procedural variability, with improvements in the accuracy of anatomical restoration [3,4,5,9,10,11]. In scapular fracture surgery, 3D-printed models allow for direct application of pre-contoured implants and simulation of surgical steps, which is particularly valuable in cases with distorted anatomy or limited surgical exposure [3,5,7,11]. These workflows can be implemented in-house, improving accessibility and cost-effectiveness [3,5,6,7,12]. This case report describes the use of 3D CT reconstruction and a sterilizable, patient-specific 3D scapular model in the operative management of a complex scapular fracture, highlighting its role in enhancing surgical planning and intraoperative efficiency.
A 22-year-old active-duty male sustained polytrauma following a high-speed motorcycle collision, resulting in fractures of the left radius and ulna, left scapula, left tibia and fibula, and left proximal femur, as well as cervical spine fractures and a left subclavian artery injury. Initial treatment occurred at a community hospital before transfer to a Level II military trauma center. Further evaluation revealed a comminuted left scapular body fracture with scapulothoracic dissociation. Neurologic examination raised concern for pan-brachial plexus injury, with complete motor and sensory deficits in the affected extremity. Imaging demonstrated transection of the suprascapular nerve branch to the supraspinatus, while the branch to the infraspinatus remained anatomically intact but non-functional. Radiographs of the left shoulder were collected, and high-resolution CT imaging of the scapula was used to render a 3D reconstruction of the scapular fracture. Imaging demonstrated a comminuted left scapula fracture with fractured margins isolating the glenohumeral joint from the scapular body (Fig. 1 and 2). Given the goals of pain control and shoulder girdle stabilization, operative management was indicated.
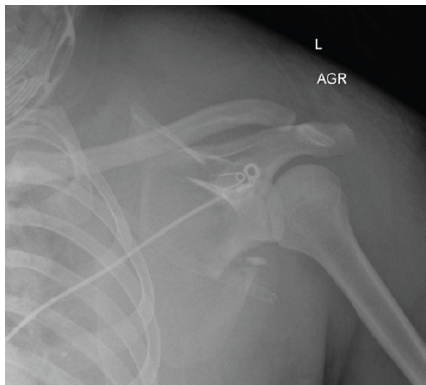
Figure 1: Pre-operative anteroposterior radiograph of the left shoulder demonstrating a comminuted left scapula fracture with displacement and medialization of the glenoid segment.
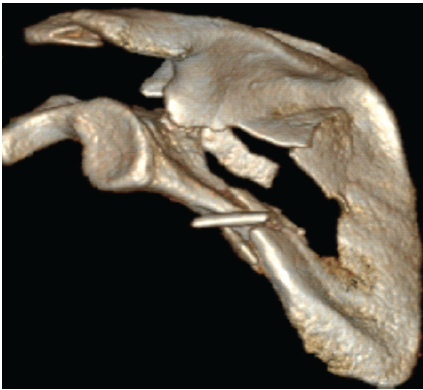
Figure 2: Pre-operative 3D computed tomography reconstruction of the left scapula further demonstrating the comminuted fracture pattern.
Utilizing the 3D reconstruction file, 3D modeling and printing software, and a non-commercial 3D printer, a full-scale, patient-specific 3D-printed scapular model was fabricated for pre-operative planning. The model was subsequently sterilized for intraoperative reference during the case. Open reduction and internal fixation of the left scapula was performed via a modified Judet approach. The 3D model facilitated visualization and planning of reduction at three critical regions: the lateral scapular body, spinoglenoid notch, and suprascapular fossa. Intraoperatively, the model served as a tactile reference for fracture reduction and implant positioning (Fig. 3).

Figure 3: Intraoperative photograph showing the application of the left scapula 3D model for surgical planning and reference.
A point-to-point reduction clamp was used to reduce the lateral scapular body as planned. Visualization through the supraspinatus and infraspinatus fossae enabled further reduction across the spinoglenoid notch; however, limited exposure complicated direct visualization of fracture margins. As determined preoperatively using the model, a contoured 3.5-mm compression plate was placed along the lateral scapular body. A 3.5-mm partially threaded cannulated screw was inserted from the spinoglenoid notch toward the glenoid using a Kirschner wire for guidance, achieving compression across the fracture. The 3D model enabled the precise determination of the screw start point and trajectory, simplifying this technically demanding step. A 2.0-mm T-plate was applied across the suprascapular fossa to neutralize the fracture. Fluoroscopy confirmed satisfactory hardware placement without joint penetration. The transected suprascapular nerve branch to the supraspinatus was identified and repaired.
Postoperatively, the patient was immobilized in a sling for 6 weeks. Post-operative radiographs and CT imaging confirmed anatomic reduction and appropriate hardware placement (Fig. 4 and 5). Pain was managed with an epidural and ketamine infusion, and neurorehabilitation planning was initiated. The patient tolerated the procedure well and was discharged with a comprehensive recovery plan.
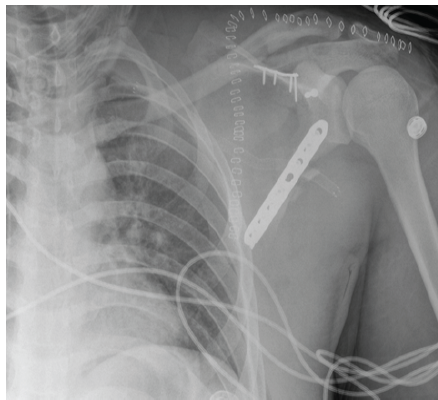
Figure 4: Post-operative anteroposterior radiograph of the left shoulder demonstrating internal fixation of the comminuted left scapular fracture.

Figure 5: Post-operative 3D computed tomography reconstruction of the left scapula confirming anatomic reduction and appropriate hardware placement.
Three-dimensional CT reconstruction and 3D printing represent significant advances in the management of complex scapular fractures. Patient-specific models provide a tangible representation of fracture anatomy, enhancing pre-operative planning, intraoperative orientation, and implant selection in anatomically complex regions [3,4,5,7,13]. Pre-contouring implants and simulating surgical steps using 1:1 models have been shown to reduce operative time and intraoperative variability while improving anatomical restoration [3,11,14]. Advanced technologies such as augmented reality and virtual simulation further enhance precision, particularly in minimally invasive approaches [11,12,13,14]. Beyond trauma, 3D models have proven useful in oncologic reconstruction and malunion correction, supporting individualized surgical planning and patient education [7,14]. Model accuracy depends on high-quality imaging. Although ultra-low-dose CT protocols reduce radiation exposure, they may compromise geometric fidelity in complex scapular fractures [15]. High-resolution CT remains essential for accurate model generation [2,15]. Fracture mapping studies have identified reproducible scapular fracture patterns that inform surgical approach and implant design [2]. In cases with limited posterior visualization through a modified Judet approach, sterilized 3D models enhance spatial orientation and facilitate precise screw trajectory planning, as demonstrated in this case. Barriers to widespread adoption include technical expertise, equipment access, and workflow integration [3,4,13]. However, in-house printing has demonstrated feasibility and cost-effectiveness [3,13]. Future applications include patient-specific implants, bioprinting, and integration with advanced navigation technologies, expanding both trauma and elective orthopedic indications [11,13].
Three-dimensional CT reconstruction and 3D printing offer meaningful advantages in the management of complex scapular fractures by enhancing anatomical visualization, surgical planning, and intraoperative execution. This case supports extending the use of patient-specific 3D models to scapular fractures in both military and civilian trauma settings, particularly when fracture comminution and anatomic complexity limit conventional imaging interpretation. Continued technological advancement is expected to further integrate 3D printing into routine orthopedic practice.
This case demonstrates that a sterilizable, patient-specific three-dimensional (3D)-printed model can provide meaningful intraoperative guidance during fixation of a complex, comminuted scapular fracture when conventional imaging and limited surgical exposure impede accurate interpretation of fracture morphology. The use of a physical model facilitated the identification of bony corridors and precise implant positioning during a technically demanding procedure. Although 3D modeling has been described in other areas of orthopedic trauma, its application to scapular fracture fixation remains limited; this report highlights its potential value as an adjunct in select cases of severe anatomical complexity in both civilian and military trauma care.
References
- 1. Cole PA, Gauger EM, Schroder LK. Management of scapular fractures. J Am Acad Orthop Surg 2012;20:130-41. [Google Scholar] [PubMed]
- 2. Yimam HM, Dey R, Rachuene PA, Kauta NJ, Roche SJ, Sivarasu S. Identification of recurring scapular fracture patterns using 3-dimensional computerized fracture mapping. J Shoulder Elbow Surg 2022;31:571-9. [Google Scholar] [PubMed]
- 3. Martínez-Gómiz JM, Muniesa MP, Martín JR, Garijo RL, Chana-Rodríguez F. Homemade 3D mirror imaging models utility for surgical treatment of complex fractures of scapula. Injury 2021;52 Suppl 4:S109-16. [Google Scholar] [PubMed]
- 4. Ling K, Wang W, Liu J. Current developments in 3D printing technology for orthopedic trauma: A review. Medicine (Baltimore) 2025;104:e41946. [Google Scholar] [PubMed]
- 5. Fillat-Gomà F, Marcano-Fernández FA, Coderch-Navarro S, Martínez-Carreres L, Berenguer A. 3D printing innovation: New insights into upper extremity surgery planning. Injury 2021;52 Suppl 4:S117-24. [Google Scholar] [PubMed]
- 6. Alemayehu DG, Zhang Z, Tahir E, Gateau D, Zhang DF, Ma X. Preoperative planning using 3D printing technology in orthopedic surgery. BioMed Res Int 2021;2021:7940242. [Google Scholar] [PubMed]
- 7. Thomas CN, Mavrommatis S, Schroder LK, Cole PA. An overview of 3D printing and the orthopaedic application of patient-specific models in malunion surgery. Injury 2022;53:977-83. [Google Scholar] [PubMed]
- 8. Skelley NW, Smith MJ, Ma R, Cook JL. Three-dimensional printing technology in orthopaedics. J Am Acad Orthop Surg 2019;27:918-25. [Google Scholar] [PubMed]
- 9. Bagaria V, Chaudhary K. A paradigm shift in surgical planning and simulation using 3Dgraphy: Experience of first 50 surgeries done using 3D-printed biomodels. Injury 2017;48:2501-8. [Google Scholar] [PubMed]
- 10. Mensel C, Gundtoft PH, Brink O. Preoperative templating in orthopaedic fracture surgery: The past, present and future. Injury 2022;53 Suppl 3:S42-6. [Google Scholar] [PubMed]
- 11. Guo Q, Li X, Tang Y, Huang Y, Luo L. Augmented reality and three-dimensional plate library-assisted posterior minimally invasive surgery for scapula fracture. Int Orthop 2022;46:875-82. [Google Scholar] [PubMed]
- 12. Rodriguez Colon R, Nayak VV, Parente PE, Leucht P, Tovar N, Lin CC, et al. The presence of 3D printing in orthopedics: A clinical and material review. J Orthop Res 2023;41:601-13. [Google Scholar] [PubMed]
- 13. Richard RD, Heare A, Mauffrey C, McGinley B, Lencioni A, Chandra A, et al. Use of 3D printing technology in fracture management: A review and case series. J Orthop Trauma 2023;37:S40-8. [Google Scholar] [PubMed]
- 14. Luo G, Zhang Y, Wang X, Chen S, Li D, Yu M. Individualized 3D printing-assisted repair and reconstruction of neoplastic bone defects at irregular bone sites: Exploration and practice in the treatment of scapular aneurysmal bone cysts. BMC Musculoskelet Disord 2021;22:984. [Google Scholar] [PubMed]
- 15. Lei M, Zhang M, Luo N, Ye J, Lin F, Chen Y, et al. The clinical performance of ultra-low-dose shoulder CT scans: The assessment on image and physical 3d printing models. PloS One 2022;17:e0275297. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies
June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies May 1, 2026 Effect of Intrawound Vancomycin Powder as an Adjunct to SystemicAntibiotic Prophylaxis on Surgical Site Infection Following Open TibialFracture Fixation: A Randomized Prospective Study
May 1, 2026 Effect of Intrawound Vancomycin Powder as an Adjunct to SystemicAntibiotic Prophylaxis on Surgical Site Infection Following Open TibialFracture Fixation: A Randomized Prospective Study May 1, 2026 Suprapatellar Tibial Nailing in Skeletally Immature Patients: A Case Series
May 1, 2026 Suprapatellar Tibial Nailing in Skeletally Immature Patients: A Case Series February 1, 2026 Post-Traumatic Subcutaneous Emphysema of the Upper Extremity Associated with an Open Scapular Fracture: A Case Report and Review of Literature
February 1, 2026 Post-Traumatic Subcutaneous Emphysema of the Upper Extremity Associated with an Open Scapular Fracture: A Case Report and Review of Literature