
Distal femoral replacement can be a viable salvage option in young adults with severely comminuted, non-reconstructible distal femur fractures when internal fixation is not feasible.
Dr. Maan H. Hajjar, Faculty of Medicine, Taibah University, Medina, Saudi Arabia. E-mail: mrockizer@gmail.com
Abstract
Introduction: Distal femur fractures (DFFs) are uncommon injuries that predominantly affect elderly patients and are usually managed with internal fixation. In young adults, distal femoral replacement (DFR) is rarely considered and is typically reserved for elderly or oncologic indications. We report two young, previously healthy patients with traumatic, non-reconstructible DFFs treated with DFR and describe their outcomes.
Case Report: Two 25-year-old patients, one female and one male, sustained high-energy DFFs with severe comminution and intra-articular destruction. In both cases, internal fixation was not feasible because of extensive bone loss and irreversible joint damage. Following multidisciplinary evaluation, DFR was performed as a salvage procedure. Both patients were allowed early weight-bearing and achieved functional ambulation. One patient developed aseptic loosening that required revision surgery; however, both patients ultimately demonstrated satisfactory pain control, knee stability, and functional recovery.
Conclusion: DFR may represent a viable salvage option in carefully selected young adults with non-reconstructible traumatic DFFs. These cases highlight an uncommon indication for DFR and add novel clinical insight to orthopedic trauma practice, although long-term durability in this population remains uncertain.
Keywords: Distal femur fracture, distal femoral replacement, megaprosthesis.
Distal femur fractures (DFFs) are uncommon but serious types of fractures with complicated management. Based on the literature, the prevalence of distal femoral fracture is 0.4% of all fractures [1]. For a young patient, although it is rare, high-intensity trauma can end up with these patterns of fractures. And for an elderly patient, a household accident is a common scenario [1]. Risk factors include old age, female gender, and any condition that increases bone fragility, such as osteoporosis, cystic bone lesions, and inflammatory bone disease, such as rheumatoid arthritis [1]. The presence of femoral or tibial prosthesis also increases the risk of fractures, which in such cases will be named a periprosthetic fracture, which is discussed a separate topic [2]. The mean age for patients developing DFFs is 74, with a range of 46–94 years [3]. Although the mean age differs among studies, the population of focus is the elderly in all studies regarding this topic [1,3,4]. Treatment is almost always surgical as these fractures are usually displaced, surgical options include open reduction with internal fixation (ORIF), which is usually the treatment of choice, especially for the younger population and patients with healthy bone quality. Distal femoral replacement (DFR) as a treatment option for DFFs is rarely considered and is preserved for elderly patients, patients with comorbidities affecting bone health, or for cases of severely comminuted fractures in whom ORIF is not achievable [4,5], it is also poorly discussed in the literature, with only two case reports discussing cases of DFFs managed by DFR [6,7]. To our latest research, publications regarding this type of treatment are inclusive to elderly patients with osteoporotic bone, or patients with malignant lesions at the site of the distal femur [8,9,10]. No research was found to report treating such fractures with DFR in the young or healthy patients In our study, we present two young and medically free patients who had a comminuted DFF and were managed by DFR. To the best of our knowledge, no similar cases have been reported in the literature.
Case 1
This patient is a 25-year-old female college student who was involved in a road traffic accident as a pedestrian struck by a motorcycle. She presented to the emergency department with a severe open fracture, with AO class: (AO 33-C3) (Fig. 1). The wound was a 15 cm laceration with exposed distal femur, patella, and lateral proximal tibial plateau.

Figure 1: Pre-operative anteroposterior and lateral radiographs showing a severely comminuted open distal femur fracture (AO/OTA 33-C3).
The distal 5 cm of the femur was severely comminuted. The preceding 10 cm showed a longitudinal split, with complete loss of the lateral aspect at the scene of the accident, while the medial aspect remained intact. Both femoral condyles were severely comminuted and no reconstrable.
Emergency surgery was performed with irrigation, debridement, and insertion of a spanning external fixator connecting the tibial shaft to the femoral shaft (Fig. 2).

Figure 2: Initial management with a knee-spanning external fixator following irrigation and debridement.
Three screws were inserted into the distal femur connecting the medial and lateral condyles, and another three screws into the proximal tibia, connecting the medial and lateral tibial plateaus.
The knee was immobilized in extension. The patient received IV antibiotics and underwent serial dressings. Over 6 weeks, the wound healed, inflammatory markers normalized, and there were no signs of infection.
The case was then discussed among orthopedic consultants, including orthopedic trauma surgeons. The initial management options considered were amputation, arthrodesis, fixation, or distal femur replacement.
Arthrodesis was not favored due to loss of knee flexion, significantly limiting the patient’s function. Fixation was not feasible given the extensive bone loss, severe articular involvement, and poor prognosis of cartilage and meniscal structures. The anterior cruciate ligament attachment was avulsed and irreparable. Approximately 75% of the patella was lost, including the cartilage. The remaining patella was deemed non-functional. Prolonged immobilization, even with Ilizarov bone transport, risked significant joint stiffness and severe quadriceps and patellar tendon adhesions. Psychological burden, prolonged hospitalization, and infection risks were also considered. After a thorough discussion, the decision for distal femur replacement was made and discussed with the patient. The patient was taken to surgery 1 month after the initial injury, following complete wound healing. At that time, there were no clinical or radiological signs of osteomyelitis or infection. There were no neurological deficits. Pre-operative laboratory tests were within normal limits. Computed tomography imaging demonstrated an unhealed comminuted DFF with intra-articular extension, while the associated tibial plateau fracture had already united. Imaging also showed approximately 75% patellar bone loss. The patellar tendon could not be adequately assessed radiologically.
Surgical technique
The patient was taken to the OR on 23 February 2023. The previous anteromedial scar was utilized. Severe adhesions around the quadriceps tendon were noted. A medial parapatellar approach was used. Surgery was performed in two stages. In the first stage, the distal femur was excised, debridement was done, and a subperiosteal release of the quadriceps tendon was performed to improve flexion. Samples from the femoral intramedullary canal were taken, showing fat droplets. Cultures and gram stain were sent. After thorough irrigation and changing drapes, gowns, and instruments, the second stage proceeded. The comminuted portion of the distal femur was approximately 4.5 cm. The remaining proximal medial half of the femoral shaft measured about 14 cm. A cementless intramedullary stem was used, spanning the defect and entering 12 cm into intact bone. The total stem length was 240 mm. The LINK Endo-Model modular system, size small, was used. There was difficulty excising the distal femur due to concerns about injuring posterior vessels, which are often scarred and at risk of traction injury. The lateral femoral condyle was completely excised, and the medial condyle was also completely excised by subperiosteal dissection. Both menisci were excised. A tibial plateau cut was made, removing 10 mm from the proximal tibia perpendicular to the shaft. Reconstruction was done using a tumor prosthesis (mega-prosthesis). A cementless femoral shaft stem (14 mm straight cylindrical, LINK system) and femur component (size small) were inserted. The tibial component (size small) was also cementless (stem size 12 mm). Length and rotation were restored, using the linea aspera as a landmark (Fig. 3).

Figure 3: Post-operative radiographs showing distal femoral replacement with restoration of limb length and alignment.
There was a patellar tendon rupture, which was tagged by non-absorbable sutures during the initial debridement. The tension from restored length (patient had 3–4 cm of pre-operative shortening) likely contributed to tendon rupture. A direct repair and augmentation of the patellar tendon was performed. A flap from the iliotibial band was used. The iliotibial band flap was mobilized and attached to the lateral patellar tendon, patella, and quadriceps tendon following an extensive lateral release to correct maltracking.
After closure of the medial parapatellar approach, patellar tracking was good. The lateral retinaculum was left open. Wound closure was done in layers after irrigation. Tranexamic acid was administered locally. A drain was inserted.
Post-operative follow-up
By post-operative day 3, the patient was able to bear full weight with a knee immobilizer. A gradual knee range of motion (ROM) protocol was initiated to protect the extensor mechanism repair. Passive ROM was progressed to 20° during the 1st week, then up to 40° over 6 weeks. At 6 weeks, active quadriceps ROM was initiated, increasing from 40° to 50°, with further gradual improvement. After 3 years of follow-up, she is walking without assistance and has not developed any complications.
Case 2
A medically free 25-year-old male smoker was brought to the emergency department by paramedics following a motor vehicle accident. The patient was conscious, alert, and oriented. The primary survey was unremarkable. On secondary survey, he had a left knee wound and deformity, as well as swelling and deformity of the right ankle. Imaging revealed mild bilateral pneumothorax, pulmonary contusions, and a comminuted fracture of the left iliac crest. Portable X-rays showed an open comminuted left distal femur and shaft fracture with intra-articular extension (AO 33-C3), a right talar neck fracture (Hawkins I), and a right distal tibial fracture with intra-articular extension (AO 43-C). The right foot and ankle injuries were managed conservatively with closed reduction and slab immobilization. The left femoral fracture was treated acutely with irrigation, debridement, and a knee-spanning external fixator (Fig. 4).
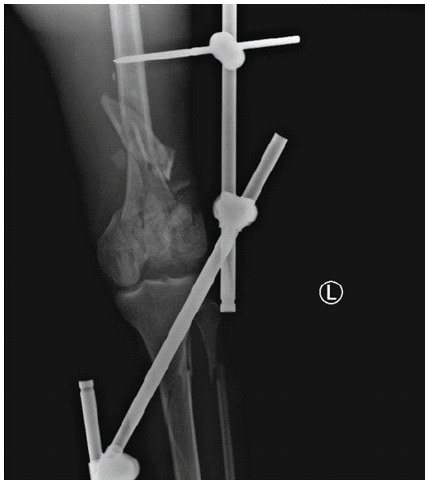
Figure 4: Radiographs showing comminuted distal femur fracture treated initially with a knee-spanning external fixator.
First and second surgeries involved combined medial and lateral exposure with tibial tubercle osteotomy, partial fixation of the medial condyle using a distal femoral plate, and insertion of a cement spacer. The lateral condyle was non-reconstructible. The second operation focused on revising fixation, correcting deformities, and reinserting a cement spacer into the bone defect of the distal femur in preparation for DFR (Fig. 5).

Figure 5: Interim reconstruction with partial fixation of the medial femoral condyle and placement of a cement spacer in the distal femoral defect.
The case was discussed with orthopedic trauma surgeons and arthroplasty surgeons, along with the physiotherapy team, and a DFR followed by a structured physiotherapy plan was planned (Fig. 6).
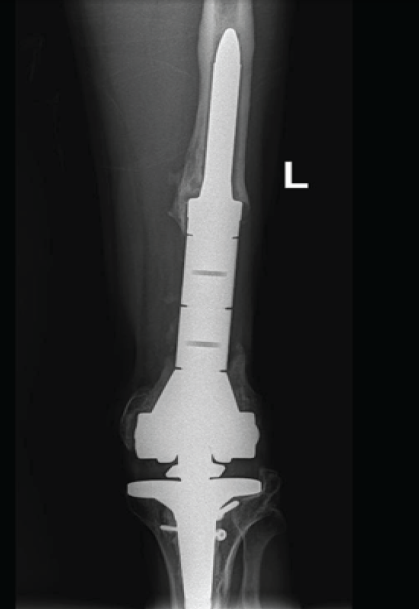
Figure 6: Final post-operative radiographs showing distal femoral replacement.
Surgical technique
Under general anesthesia with successful endotracheal intubation, the patient was positioned supine. A tourniquet was applied to the left proximal thigh. Lateral thigh support and two-foot pieces were used to allow knee flexion. The limb was prepped and draped in a sterile fashion. One gram of prophylactica cefazolin was administered.
The previous surgical approach for the left tibia was utilized. Dissection was performed through the lateral approach, with removal of the skin and subcutaneous tissue. The previously inserted plates and screws were removed. The tibial fracture site demonstrated good healing without infection. The approach was extended medially along the previous scar over the knee and femur.
Further dissection exposed the knee joint and distal femur. The quadriceps tendon was released, and a medial parapatellar arthrotomy with rectus snip was performed. The previously placed femoral plate and cement spacer were removed.
For femoral preparation, the distal femur was cut at the preoperatively planned level, and reaming of the femoral canal was performed. A 13.5 mm × 100 mm trial stem showed a good fit. An extra-small femoral component was selected.
For tibial preparation, the tibia was reamed until the appropriate size was achieved, and a trial stem measuring 150 mm × 12 mm demonstrated good stability and adequate length. A rotating platform Metal-Backed Tibial tray, size 2, was selected, along with a polyethylene insert trial of size 14.
For implantation, the final prostheses included a legacy posterior stabilized cemented femoral stem measuring 13.5 mm × 100 mm with an extra-small component, and a cemented tibial component measuring 150 mm × 12 mm with a tibial tray size 2. A polyethylene insert of size 14 was used (Fig. 6). After allowing the cement to cure, final assessment demonstrated a stable knee with full ROM. The quadriceps tendon was repaired, the arthrotomy was closed, and a drain was inserted. The subcutaneous tissues were closed in layers, and the skin was closed with skin clips. Sterile dressings were applied. The patient tolerated the procedure well and was transferred to the recovery room in good condition, with intact distal neurovascular status. He was planned for a few days of inpatient observation for pain control and to initiate full weight-bearing as tolerated. Discharge was planned once medically fit.
Post-operative follow-up
The patient underwent extensive exercises to improve ROM and muscle strength starting 1 week’s post-operative. We delayed active extension to 6 weeks due to the quadriceps repair. He could reach flexion of 30° in the first 3 months, and 45°, and extension was full by 6 months, extension, he was using walking cane for the first 6 months after surgery, then he became able to walk without any walking aid. At 12 months post-operative, the patient reported start-up pain. On examination, there was femoral tenderness and thigh pain during extension against gravity; the femoral X-ray showed progressive radiolucent line around the femur stem, and a diagnosis of aseptic loosening was confirmed. The patient underwent a revision of the femoral component using cemented stems, and he is doing well postoperatively. On 6 months follow up, flexion was 80° and extension was full, and he is walking without a cane.
DFFs are uncommon and difficult to manage. In such fractures, restoration of the anatomy is almost never possible by conservative management, so surgical treatment is the gold standard when appropriate [1]. Treatment decisions depend on patient age, bone quality, and fracture complexity. Young patients are typically treated with internal fixation [11,12]. Arthroplasty is rarely considered in healthy young adults, DFR, which is considered one type of total knee arthroplasty, is reserved for the elderly or those with non-reconstructible fractures. The literature provides minimal data on outcomes of DFR in young adults [8,10]. In our series, both patients in this series; young and previously healthy adults, represent rare but justified use of DFR following failure or infeasibility of fixation. In both cases, the fractures were highly comminuted, intra-articular, and segmentally destructive with extensive cartilage loss, leaving DFR as the only viable surgical option. In Case 1, extensive bone and soft-tissue damage, extensive cartilage loss, patellar tendon avulsion, and prior infection risk further complicated management. Reconstruction attempts would likely have resulted in poor function or complications like joint stiffness, infection, and extensor mechanism failure. As seen in the literature, prolonged immobilization can also lead to severe adhesions requiring additional interventions like quadricepsplasty. Early mobilization post-DFR allowed for improved rehabilitation. This patient represents one of the youngest cases in which the team performed a distal femur replacement that was done for a traumatic indication rather than post-traumatic arthritis. Multidisciplinary discussion with trauma and reconstruction surgeons is essential. Implant availability and surgical expertise are also crucial. The patient was referred to our center from another country due to these considerations. Infection risk and psychological impact were significant factors in management. The patient’s and family’s understanding was vital. Outcomes so far are promising. While long-term outcomes remain unknown, the team believes this approach yields superior results compared to alternative management options.
In Case 2, the patient failed two prior fixation attempts, and radiographic and clinical signs suggested non-union and ongoing dysfunction. DFR provided stable alignment, pain relief, and functional improvement. When it comes to choosing the type of prosthesis, mega-prostheses are not discussed in the literature separately from oncologic cases and elderly patients. Since those populations have poor life expectancy due to their comorbidities, not enough studies about the effectiveness of mega-prostheses are available [13], for our patients, both achieved satisfactory outcomes without infection, periprosthetic fractures, or malalignmen, however, one patient developed an aseptic loosening after 1 year. Long-term durability in young active patients remains uncertain, but the short-term functional outcomes were satisfactory.
This case series presents two rare instances of DFR in young, previously healthy adults with complex, comminuted, intra-articular femoral fractures. In both cases, internal fixation was not feasible, necessitating the use of mega-prosthetic implants. Both patients demonstrated improved stability, pain control, and functional mobility in the first 6 weeks postoperatively. These cases suggest that with appropriate surgical planning and patient selection, DFR can be a viable salvage option in young trauma patients. Further studies are needed to assess long-term outcomes and define clear criteria for such interventions in this population.
In rare cases of traumatic distal femur destruction in young adults, distal femoral replacement may provide early stability, pain relief, and functional recovery when fixation is not achievable.
References
- 1. Ehlinger M, Ducrot G, Adam P, Bonnomet F. Distal femur fractures. Surgical techniques and a review of the literature. Orthop Traumatol Surg Res 2013;99:353-60. [Google Scholar] [PubMed]
- 2. Marsland D, Mears SC. A review of periprosthetic femoral fractures associated with total hip arthroplasty. Geriatr Orthop Surg Rehabil 2012;3:107-20. [Google Scholar] [PubMed]
- 3. Meluzio MC, Oliva MS, Minutillo F, Ziranu A, Saccomanno MF, Maccauro G. The use of knee mega-prosthesis for the management of distal femoral fractures: A systematic review. Injury 2020;51 Suppl 3:S17-22. [Google Scholar] [PubMed]
- 4. Tibbo ME, Parry JA, Hevesi M, Abdel MP, Yuan BJ. Distal femoral replacement versus ORIF for severely comminuted distal femur fractures. Eur J Orthop Surg Traumatol 2022;32:959-64. [Google Scholar] [PubMed]
- 5. Pearse EO, Klass B, Bendall SP, Railton GT. Stanmore total knee replacement versus internal fixation for supracondylar fractures of the distal femur in elderly patients. Injury 2005;36:163-8. [Google Scholar] [PubMed]
- 6. Choi NY, Sohn JM, Cho SG, Kim SC, In Y. Primary total knee arthroplasty for simple distal femoral fractures in elderly patients with knee osteoarthritis. Knee Surg Relat Res 2013;25:141-6. [Google Scholar] [PubMed]
- 7. Yoshino N, Takai S, Watanabe Y, Fujiwara H, Ohshima Y, Hirasawa Y. Primary total knee arthroplasty for supracondylar/condylar femoral fracture in osteoarthritic knees. J Arthroplasty 2001;16:471-5. [Google Scholar] [PubMed]
- 8. Senthilkumaran S, MacDonald DR, Rankin I, Stevenson I. Total knee arthroplasty for distal femoral fractures in osteoporotic bone: A systematic literature review. Eur J Trauma Emerg Surg 2019;45:841-8. [Google Scholar] [PubMed]
- 9. Dathik S, Chopra RK, Talwar J, Pheroz M, Prasad R. Primary hydatidosis of distal femur masquerading malignancy -A rare case. J Clin Orthop Trauma 2019;10:213-20. [Google Scholar] [PubMed]
- 10. Joshi N, Pujol O, Prat S. Complex distal femoral fractures in the fragile elderly patient treated by distal femoral replacement: A report of three cases. [Artículo traducido] Fractura de fémur distal compleja en el paciente frágil y anciano tratada mediante reemplazo femoral distal: Reporte de 3 casos. Rev Esp Cir Ortop Traumatol 2022;66:149-53. [Google Scholar] [PubMed]
- 11. Gangavalli AK, Nwachuku CO. Management of distal femur fractures in adults: An overview of options. Orthop Clin North Am 2016;47:85-96. [Google Scholar] [PubMed]
- 12. Haidukewych GJ, Springer BD, Jacofsky DJ, Berry DJ. Total knee arthroplasty for salvage of failed internal fixation or nonunion of the distal femur. J Arthroplasty 2005;20:344-9. [Google Scholar] [PubMed]
- 13. Gautam D, Malhotra R. Megaprosthesis versus allograft prosthesis composite for massive skeletal defects. J Clin Orthop Trauma 2018;9:63-80. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 Emerging Trends in Distal Femur Fracture Treatment Modalities – A Narrative Review
March 1, 2025 Emerging Trends in Distal Femur Fracture Treatment Modalities – A Narrative Review September 10, 2021 Distal Femur Tumor Megaprosthesis for Non-union of Supracondylar Femur Fracture after Failed Osteosynthesis. An Ingenious Solution.
September 10, 2021 Distal Femur Tumor Megaprosthesis for Non-union of Supracondylar Femur Fracture after Failed Osteosynthesis. An Ingenious Solution. July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report May 1, 2026 Functional Outcomes and Complications of Megaprosthetic Reconstruction in Limb-Salvage Surgery for Musculoskeletal Tumors: A Scoping Review
May 1, 2026 Functional Outcomes and Complications of Megaprosthetic Reconstruction in Limb-Salvage Surgery for Musculoskeletal Tumors: A Scoping Review