
In pediatric osteopetrosis related femoral neck fractures, physeal sparing fixation may achieve union but risks late capital femoral epiphysis slippage, suggesting that crossing the physis may be necessary for long term stability.
Dr. J K Giriraj Harshavardhan, Department of Orthopedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai - 600116, Tamil Nadu, India. E-mail: girirajh@yahoo.com
Abstract
Introduction: Pathological femoral neck fractures are rare but significant injuries in children with osteopetrosis and pose unique management challenges. Optimal treatment strategies remain controversial, particularly in skeletally immature patients with open physes.
Case Report: We report a rare case of a 6-year-old boy with osteopetrosis who sustained a pathological fracture of the left femoral neck following trivial trauma. The child was managed with closed reduction and physeal-sparing internal fixation using cannulated cancellous screws, followed by hip spica immobilization. Although fracture union was achieved, the patient subsequently developed slippage of the capital femoral epiphysis, resulting in a painless limp and limb length discrepancy.
Conclusion: This case highlights the importance of fixation strategy in pathological pediatric femoral neck fractures and suggests that crossing the physis may be necessary to prevent late epiphyseal slippage.
Keywords: Osteopetrosis, pediatric femoral neck fracture, pathological fracture, cannulated cancellous screws.
Osteopetrosis is a rare hereditary metabolic bone disorder characterized by increased bone density due to defective osteoclastic bone resorption. Based on the age of onset, it is classified into infantile (malignant), intermediate, and adult-onset (benign) forms. Adult-onset osteopetrosis is further subdivided into two types. Many patients remain asymptomatic and are diagnosed only after sustaining fractures, most commonly involving the proximal femur [1,2]. Management of pathological femoral neck fractures in children with osteopetrosis is particularly challenging due to abnormal bone architecture, increased bone brittleness, technical difficulties during surgery, and risks of complications such as avascular necrosis, non-union, and growth plate injury. Owing to the rarity of this condition, standardized treatment guidelines are lacking [3,4,5,6].
A 6-year-old boy presented to the emergency department with pain and inability to bear weight on the left lower limb following a trivial slip and fall. Clinical examination revealed restricted and painful movements of the left hip. Radiographs of the pelvis demonstrated a fracture of the left femoral neck with marked sclerosis of the pelvic bones and proximal femur, raising suspicion of a pathological fracture (Fig. 1).
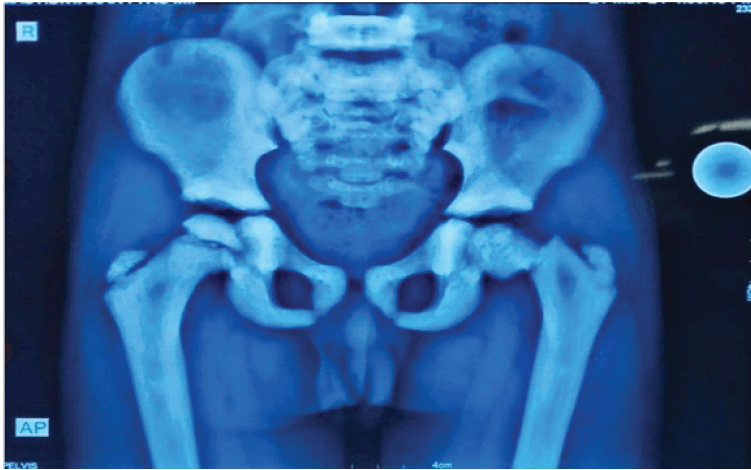
Figure 1: Anteroposterior radiograph of pelvis with both hips at presentation showing left femoral neck fracture with diffuse bony sclerosis.
The child was the firstborn of two siblings, delivered at term following an uncomplicated pregnancy and normal vaginal delivery. There was no history of neonatal intensive care admission or prior fractures. Magnetic resonance imaging of the pelvis showed features suggestive of osteopetrosis.
The patient underwent closed reduction on a fracture table using traction and internal rotation, followed by internal fixation with two 4-mm cannulated cancellous screws, deliberately stopping short of the physis (Fig. 2).
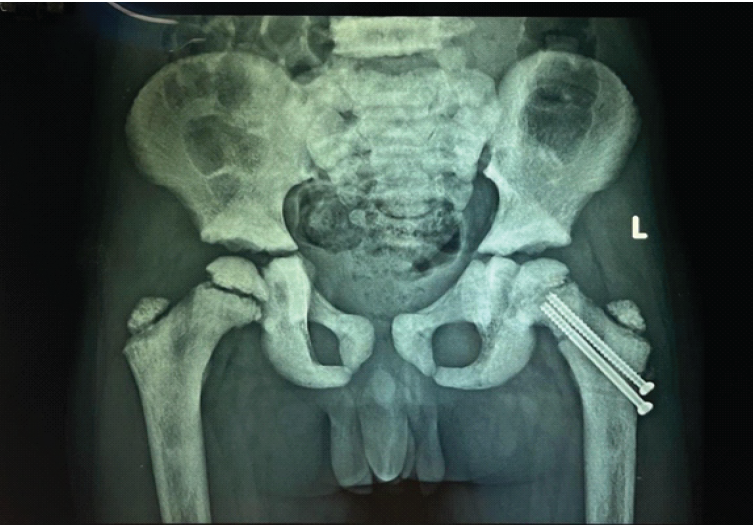
Figure 2: Immediate post-operative radiograph showing fixation with two cannulated cancellous screws (May 07, 2024).
Intraoperatively, significant technical difficulty was encountered due to dense sclerotic bone, including breakage of a drill bit, which required removal by burring the surrounding bone.
Postoperatively, a hip spica cast was applied for 7 weeks. After removal of the hip spica cast, gradual physiotherapy and progressive weight-bearing were initiated under clinical supervision. Follow-up radiographs after cast removal showed satisfactory fracture healing (Fig. 3).
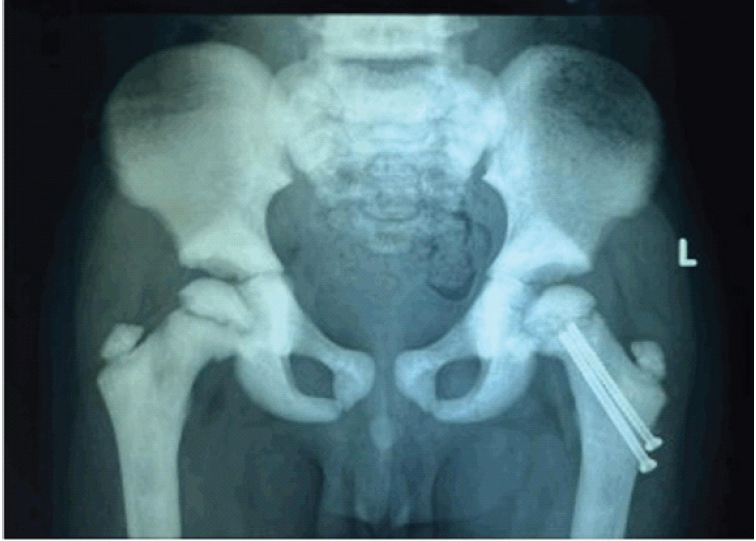
Figure 3: Radiograph at 7-Weeks follow-up after Hip Spica Cast removal showing progressing fracture union without evidence of avascular necrosis.
At 3 months, the fracture had united without evidence of avascular necrosis or non-union (Fig. 4), and the child had a painless full range of hip movements. Full weight-bearing ambulation was initiated.
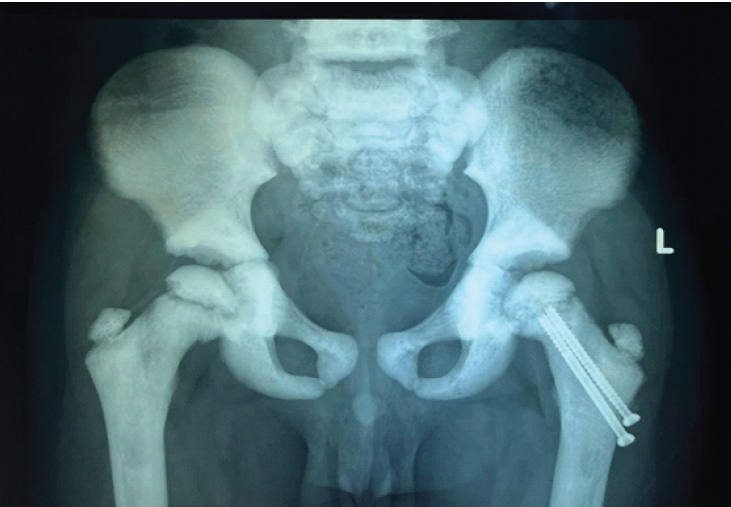
Figure 4: Radiograph at 3-month follow-up showing progressing fracture union without evidence of avascular necrosis.
Seven months postoperatively, the child presented with a painless limp and apparent limb shortening. Radiographs revealed slippage of the capital femoral epiphysis despite fracture union (Fig. 5).

Figure 5: Radiograph at 7-month follow-up demonstrating slippage of the capital femoral epiphysis.
The likely cause was stress concentration at the screw tips adjacent to the physis. Revision fixation was deferred due to the small size of the epiphysis and anticipated poor screw purchase. At 1-year follow-up, radiographs demonstrated progression of epiphyseal slippage with significant limb length discrepancy (Fig. 6), although the child remained painless and ambulatory.

Figure 6: One-year post-operative radiograph showing progression of epiphyseal slip with limb length discrepancy.
The patient was advised to continue observation with a plan for future deformity correction.
Osteopetrosis results in dense but brittle bone due to defective osteoclastic resorption, making fracture fixation technically demanding. Femoral neck fractures are particularly problematic because of high biomechanical stress and the risk of growth-related complications in children [1,2]. Various fixation strategies have been described for pediatric femoral neck fractures, including cannulated screws crossing the physis, pediatric dynamic hip screws, and locking plate constructs. However, the optimal fixation method in patients with osteopetrosis remains uncertain due to altered bone biology, increased bone brittleness, and technical challenges during drilling and implant placement. Although conservative treatment has been described, it is associated with complications such as non-union and coxa vara [5,6]. Surgical fixation is generally favored; however, drilling and implant insertion are difficult due to bone hardness, with reported complications including drill bit bending or breakage [3,7,8]. Similar intraoperative challenges were encountered in our case. Our case demonstrates that physeal-sparing fixation, while initially successful for fracture union, may predispose to subsequent capital femoral epiphyseal slippage. We believe that screw tips may act as stress risers near the growth plate. The hypothesis that screw tips near the physis may act as stress risers remains speculative and would require biomechanical validation in future studies. Similar fixation challenges and complications have been described in previous reports of osteopetrotic fractures, emphasizing the need for careful surgical planning and consideration of alternative fixation strategies in this unique patient population. Crossing the physis during fixation may provide better long-term stability in pathological femoral neck fractures, despite traditional concerns regarding physeal injury [3,4,9]. Advanced imaging modalities such as computed tomography may provide better evaluation of fracture morphology and implant positioning in osteopetrotic bone. Alternative fixation options, including physeal-crossing screws, pediatric dynamic hip screw constructs, or supplementary fixation, may be considered to improve stability in pathological femoral neck fractures associated with osteopetrosis. Post-operative magnetic resonance imaging evaluation of the physis could potentially help assess growth plate viability and detect early complications. Management of osteopetrosis often requires a multidisciplinary approach involving orthopedic surgeons, endocrinologists, and metabolic specialists to address both skeletal and systemic manifestations. Orthopedic surgeons should anticipate intraoperative challenges and carefully select fixation strategies in osteopetrotic fractures. Meticulous technique and close post-operative surveillance are essential [10].
Limitations
This report has several limitations. First, it represents a single case observation, which limits the ability to generalize the findings to the broader pediatric population with osteopetrosis. Because the study involves only one patient, conclusions regarding the optimal fixation strategy remain speculative and should be interpreted with caution. Although the patient was followed for 1-year, longer follow-up would be required to assess late complications such as avascular necrosis, progressive deformity, or degenerative changes of the hip joint. Genetic confirmation of the specific subtype of osteopetrosis was not performed in this case, which may influence fracture behavior and healing potential. Objective quantification of bone quality using bone mineral density testing or advanced imaging techniques was not performed. Standardized pediatric functional outcome scores or gait analysis were not utilized, and clinical recovery was assessed primarily through physical examination and radiographic follow-up. Case reports may also be subject to publication bias, as unusual or complicated cases are more likely to be reported.
Surgical fixation is an effective treatment option for pathological femoral neck fractures in children with osteopetrosis, despite significant technical challenges. Although fracture union can be achieved with physeal-sparing techniques, this case illustrates the risk of late capital femoral epiphyseal slippage. This case suggests that physeal-crossing fixation may provide improved stability in pathological femoral neck fractures associated with osteopetrosis; however, further clinical studies are required to validate this observation.
Pathological femoral neck fractures in children with osteopetrosis should be managed surgically. Internal fixation that crosses the physis may be necessary to prevent subsequent capital femoral epiphyseal slippage and achieve optimal outcomes.
References
- 1. Aydin AT, Yeter AB. Osteopetrosis. Turk Klin J Orthop Traumatol 2010;3:82-6. [Google Scholar] [PubMed]
- 2. Stark Z, Savarirayan R. Osteopetrosis. Orphanet J Rare Dis 2009;4:5. [Google Scholar] [PubMed]
- 3. Aslan A, Baykal YB, Uysal E, Atay T, Kirdemir V, Baydar ML, et al. Surgical treatment of osteopetrosis-related femoral fractures: Two case reports and literature review. Case Rep Orthop 2014;2014:891963. [Google Scholar] [PubMed]
- 4. Birmingham P, McHale KA. Treatment of subtrochanteric and ipsilateral femoral neck fractures in an adult with osteopetrosis. Clin Orthop Relat Res 2008;466:2002-8. [Google Scholar] [PubMed]
- 5. Armstrong DG, Newfield JT, Gillespie R. Orthopedic management of osteopetrosis: Results of a survey and review of the literature. J Pediatr Orthop 1999;19:122-32. [Google Scholar] [PubMed]
- 6. Bombacı H, Esenkaya İ, Görgec M, Kuşkaya S. Femoral neck fractures in osteopetrosis. Eklem Hastalik Cerrahisi 1998;9:56-8. [Google Scholar] [PubMed]
- 7. Rafiq I, Kapoor A, Burton DJ, Haines JF. A new modality of treatment for non-united fracture of the humerus in a patient with osteopetrosis: A case report. J Med Case Rep 2009;3:15. [Google Scholar] [PubMed]
- 8. Kumbaraci M, Karapinar L, Incesu M, Kaya A. Treatment of bilateral simultaneous subtrochanteric femur fractures with proximal femoral nail antirotation (PFNA) in a patient with osteopetrosis: Case report and review of the literature. J Orthop Sci 2013;18:486-9. [Google Scholar] [PubMed]
- 9. Sar C, Pinar H, Demirhan M, Yazicioglu O. Bilateral femoral neck fracture in a case of osteopetrosis. Acta Orthop Traumatol Turc 1994;28:56-8. [Google Scholar] [PubMed]
- 10. Martinez FL, Zenteno CB, Rodriguez RS. Subtrochanteric fracture in autosomal dominant osteopetrosis type II: A case report. Acta Ortop Mex 2006;20:30-2. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis
December 1, 2025 Management of Pathological Subtrochanteric Fractures in Two Patients with Osteopetrosis July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall
July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report
July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes
June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes