
The all-inside ACL reconstruction technique is a reliable alternate to the full tibial tunnel technique with reduced incidences of post-operative pain and reconstruction failure.
Dr. Nitish Kumar, Department of Orthopedics, All India Institute of Medical Sciences, Gorakhpur, Uttar Pradesh, India. E-mail: nitishaiims@gmail.com
Abstract
Background: Anterior cruciate ligament (ACL) reconstruction aims to restore knee stability and function while minimizing tunnel-related complications. The all-inside technique was developed to preserve bone stock, reduce post-operative pain, and improved function. This study, therefore, aimed to compare clinical and radiological outcomes between the all-inside and full tibial tunnel ACL reconstruction techniques.
Materials and Methods: The study prospectively enrolled 60 patients and divided in two groups, 30 patients in each, an all-inside and full tibial tunnel group. At final follow-up, subjective functional scores were used to assess the functional outcome, and magnetic resonance imaging (MRI) was used to assess socket/tunnel widening and graft characteristics. Subjective functional scores included the Lysholm knee score, the International Knee Documentation Committee score, and the knee society score for pain and function. MRI was used to measure the value of bone socket/tunnel widening, graft fiber integrity, graft laxity, and posterior cruciate ligament (PCL) buckling.
Results: At the final follow-up of 18–24 months, no significant differences were found with respect to femoral socket widening and subjective function scores. However, a significant increase in tibial tunnel diameter was found in the full tibial tunnel group compared to the all-inside group (P < 0.005). Knee stability and MRI parameters, including graft continuity, graft laxity, and PCL buckling, were comparable between groups.
Conclusion: Both surgical techniques result in satisfactory clinical and radiological outcomes following ACL reconstruction. However, the all-inside technique offers a radiological advantage by significantly reducing tibial tunnel enlargement, likely due to closed socket creation and suspensory fixation, making it a biomechanically favorable option without compromising functional results.
Keywords: Anterior cruciate ligament reconstruction, all-inside technique, full tibial tunnel technique, tunnel widening, suspensory fixation, magnetic resonance imaging.
Anterior cruciate ligament (ACL) injury is considered one of the most common knee injuries in the athletically active population, resulting in functional instability of the knee joint and impairment of athletic performance [1]. The purpose of ACL reconstruction is to reproduce the structural and functional properties of the ACL and to prevent further degenerative complications of the joint [2]. Perhaps the most controversial factor concerning the ACL-deficient knee is the expected course of the untreated joint. Loss of ligament does not necessarily result in poor function [3,4]. However, loss of function of this ligament often results in severe problems for the patient, with frequent re-injury, allowing the joint to be further damaged. Reconstruction of ACL has evolved from an open procedure to an arthroscopically-assisted technique, which has reduced patient morbidity, improved cosmesis, and facilitates early rehabilitation.
The all-inside ACL reconstruction technique is a relatively new development in ACL surgery [5]. This technique was originally described over 20 years ago [6]. The all-inside ACL reconstruction technique has emerged as a minimally invasive alternative. It involves the creation of a socket in place of tunnels on both femoral and tibial sides using retrograde drilling, allowing preservation of bone stock on the outer cortex and reduction of soft-tissue trauma. This technique also facilitates graft tensioning on both ends and potentially reduces post-operative pain and rehabilitation time.
The conceptual difference between full tunnel technique and all-inside ACL reconstruction is that of “potting the graft ”into a compact bony socket as opposed to pulling a graft through a full-length tunnel, this allow for more complete fill of the aperture and socket with graft collagen and eliminates the need for interference fixation, which can displace a graft to one portion of aperture and can be deleterious to healing by limiting interface area, as well as affecting the biological milieu [7]. In all-inside technique, preserved tibial cortex allows strong, low-profile hybrid fixation.
Clinical and radiological comparisons between the All-inside and complete tibial tunnel techniques have yielded variable results with ongoing debate. Therefore, there is a need for prospective comparative data to evaluate whether the minimally invasive All-inside technique provides equivalent or superior outcomes to the conventional complete tibial tunnel method.
This study was a prospective comparative study from January 2022 to July 2025. Approval from the institutional ethics committee was taken with IHEC Ref. No. IESC/T-57/January 03, 2022. A total of 60 patients enrolled in the study, meeting the inclusion criteria and divided into two groups: Group A all-inside and Group B complete tibial tunnel. Inclusion criteria were patients having an isolated ACL tear, which was confirmed on magnetic resonance imaging (MRI), age – 15–55 years, male or female gender, time from injury to surgery is <1 year, and patient willingness to participate and give informed and written consent for the study. Exclusion criteria were revision surgery, multi-ligament injuries, inflammatory arthritis, and knee varus more than 10°.
Pre-operative evaluation
All patients had subjective instability and functional impairment, confirmed by a positive Lachman test, anterior drawer test, and/or pivot-shift test findings. Radiological evaluation was done with the help of X-ray knee AP and lateral view, and MRI.
Operative method
All patients fulfilling the inclusion criteria were planned for arthroscopic ACL reconstruction. All-inside and full tibial tunnel group allocation was done on a 1:1 basis in each group. Basic steps are similar in both groups, such as patient positioning, pneumatic tourniquet applied at the base of the thigh. Standard anteromedial and anterolateral portals were made, and diagnostic arthroscopy was done to confirm the torn ACL and other associated knee injury. The semitendinosus tendon was harvested when planning for all-inside ACL reconstruction, and the semitendinosus and gracilis were both harvested for the full tibial tunnel group. Quadrupled semitendinosus and 5-strand semitendinosus with gracilis were used for all-inside and full tibial tunnel groups, respectively (Fig. 1).
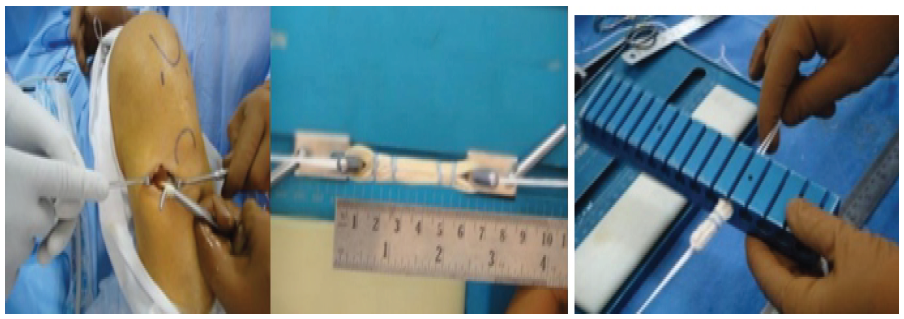
Figure 1:Graft harvesting and preparation.
The graft configuration differed between the groups because the all-inside technique requires a shorter but thicker graft that can be adequately prepared using a quadrupled semitendinosus tendon, allowing preservation of the gracilis. In contrast, the full tibial tunnel technique requires a longer graft, and therefore, both semitendinosus and gracilis tendons were harvested to obtain sufficient graft length and diameter.
Femoral preparation was done using an appropriate size of reamer. The rimmer of the diameter of the prepared graft size was used. The length of the socket on the femur side was decided depending on the length of the graft prepared. In the all-inside technique, FlippCutter was passed from outside to inside. FlippCutter was introduced in the joint through the center of the tibial jig. Once the tibial jig was removed and the cutter was flipped, it was withdrawn while drilling (Fig.2). The depth of the socket depending upon the length of the graft, as marking over the flip-cutter.

Figure 2: Retro-drilling system for tibial socket preparation.
For the complete tibial tunnel group, the tibia is drilled through and through by appropriate size reamer. The graft was pulled into the joint through the anteromedial portal. The adjustable button was flipped at the outer cortex of the femur, and the graft was pulled through the anteromedial portal into the tibial socket by pulling the fiber tape attached at the end of the graft and fixed over the tibial cortex using an adjustable button system button. For a complete tibial tunnel group graft pulled through the tibia tunnel and pulled in femoral socket in a similar fashion as all-inside and on the tibial side fixed with a biodegradable interference screw.
Rehabilitation protocol
Both groups were subjected to a similar standard rehabilitation protocol. The patients were allowed crutch-assisted partial weight bearing within 6 weeks after surgery. The operated knee was kept protected in a long-hinged knee brace for a period of 8 weeks. The knee range of motion exercise was started from the 1st post-operative day with gradual attainment of full range by the end of 8 weeks. Usually, the patients were allowed to bear full weight on the operated knee after 6 weeks. Low-speed treadmill jogging was started at 3–6 months, and pre-injury sports activity was allowed at 9–12 months following surgery.
Clinical assessment
At 18–24 months in final follow-up, the knee joint stability was checked clinically with the anterior drawer test, Lachman test, and pivot-shift test. Patients reported objective functional scores, which included the Lysholm knee score, the subjective International Knee Documentation Committee (IKDC) score, and the Knee Society Score (KSS) for pain and function was obtained on standard questionnaire forms.
Radiological evaluation
At last, a follow-up of 18–24 months 3T MRI unit (Philips, Holland) was done for all patients to assess graft integrity and socket/tunnel enlargement. Bone socket/tunnel enlargement was evaluated digitally by non-contrast enhanced T2 non-fat saturation metal artefact reducing software technique MRI in the oblique coronal, sagittal, and axial planes, which measured the widths of the bone tunnels in a line perpendicular to the long axis of the socket/tunnels. The articular opening point of the bone tunnel and the midpoint of the entrance and exit of the tunnel were measured. The final readings for each position were obtained by calculating the mean values of coronal and sagittal positions measurement. Graft behavior and remaining posterior cruciate ligament (PCL) buckling were evaluated.
Statistical analysis
Two independent investigators calculated the values of socket/tunnel diameters measured during surgery and by MRI at the final follow-up. Femoral and tibial socket diameters (FSD and TSDs) were measured at two points on either side of the femur and tibia. One of the measured values was taken at the site of entry of the socket and other at the midpoint of the socket. Data were analyzed by using the Statistical Package for the Social Sciences-20 software, and the data were presented in Mean (standard deviation) and frequency (percentage). Within change in the continuum variable was assessed by repeated measures Analysis of Variance (ANOVA) (2-way ANOVA) followed by post hoc comparison using the Bonferroni post hoc test. P < 0.05 was taken as statistically significant.
Patient characteristics
This study included data of 60 patients with complete ACL tear. Of these, 30 patients (22 males and 8 females; mean age 27.97 ± 5.43 years) underwent all-inside ACL reconstruction, while another 30 patients (26 males and 4 females; mean age 26.07 ± 5.43 years) underwent ACL reconstruction using the full tibial tunnel Pre-operative patient characteristics are shown in (Table 1). There were no significant differences in gender, age, and follow-up duration between all-inside and full tibial tunnel groups.
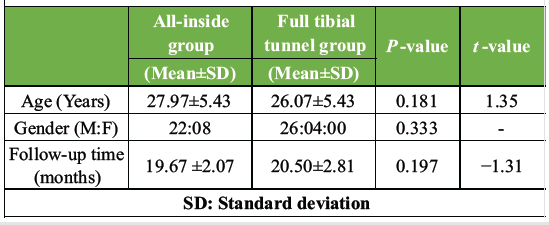
Table 1: Demographic data of both group
Functional outcome
Functional outcomes were assessed at the final follow-up visit, conducted between 18 and 24 months after surgery. Patient-reported knee function was evaluated using subjective knee scores, such as IKDC, KSS (Pain) and KSS (Function), and Lysholm knee score (Table 2 and Fig. 3).
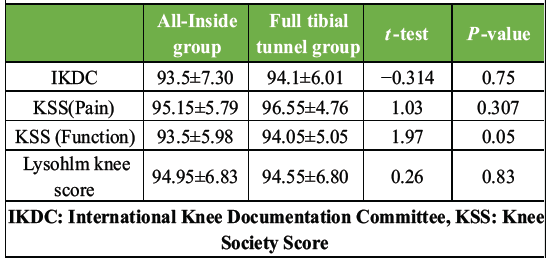
Table 2: Subjective functional score at final follow-up
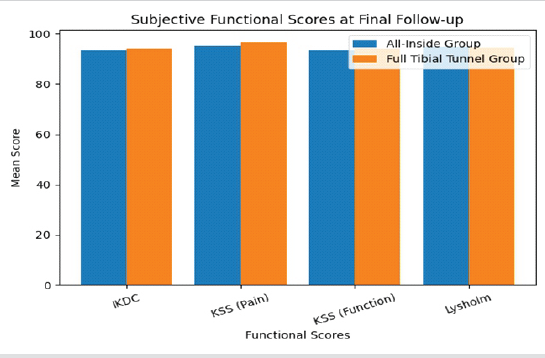
Figure 3: Functional scores between 2 groups.
Radiological outcome
Radiological outcomes were assessed at the final follow-up visit, between 18 and 24 months after surgery, with the help of MRI.
Widening of socket/tunnel
FSD and TSD/tibial tunnel diameter (TTD)was measured at two points on follow-up MRI in both sagittal and axial image, one at entrance of socket and one at midpoint of socket/tunnel. Table 3 compares intra-operative and follow-up diameters of the femoral socket and tibial socket/tunnel between the all-Inside and the full tibial tunnel group, along with the difference socket/tunnel widening and corresponding P-values.
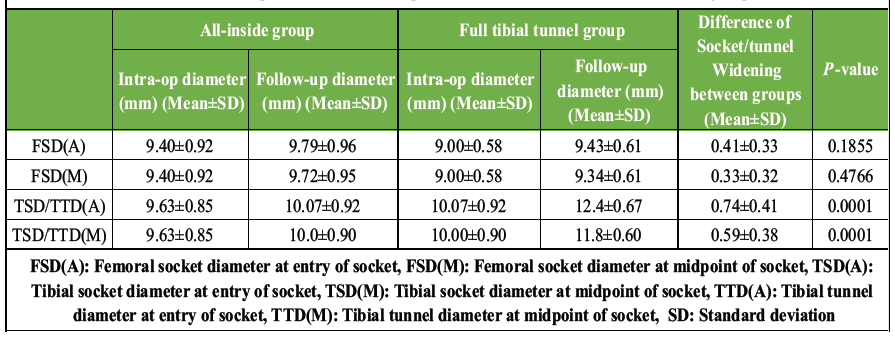
Table 3: Intra-operative and follow-up diameter of bone Socket/Tunnel in both groups
Femoral socket widening
Femoral socket widening is the difference between the intraoperative socket/tunnel diameter, which is the same as the drill diameter used, and the follow-up diameter of the socket on MRI. In all-inside group, the mean intraoperative FSD at entry of socket [FSD(A)] was 9.40 ± 0.92 and at midpoint of socket [FSD(M)] was 9.40 ± 0.92. Follow-up mean FSD(A) was 9.79 ± 0.96 and FSD(M) it was 9.72 ± 0.95. In full tibial tunnel group, the mean intraoperative FSD(A) was 9.00 ± 0.58 and FSD(M) was 9.00 ± 0.58. Follow-up mean FSD(A) was 9.43 ± 0.61 and FSD(M) it was 9.34 ± 0.61. However, the difference in femoral socket widening between the two techniques was minimal and not statistically significant, with P = 0.1855 (Articular) and 0.4766 (midpoint) (Fig. 4).
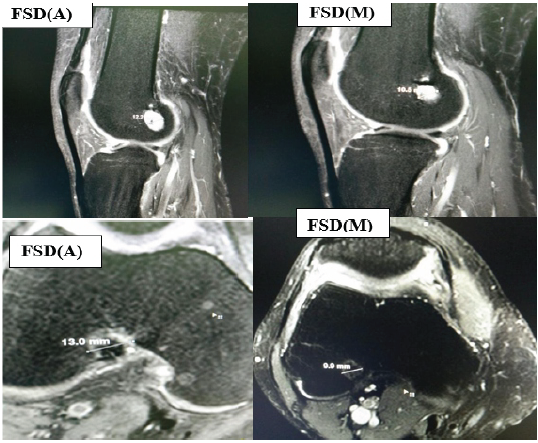
Figure 4: Femoral socket diameter in sagittal and axial plane.
Tibial socket/tunnel widening
In all-inside group, the mean intraoperative TSD at entry of socket [TSD(A)] was 9.63 ± 0.85 and at midpoint of socket [TSD(M)] was 9.63 ± 0.85. Follow-up mean TSD(A) was 10.07 ± 0.92, and SD(M) it was 10.0 ± 0.90. In full tibial tunnel group, the mean intraoperative TSD(A) was 10.07 ± 0.92 and TSD(M) was 10.07 ± 0.92. Follow-up mean TSD(A) was 12.4 ± 0.67, and TSD(M) it was 11.8 ± 0.60 (Fig. 5).
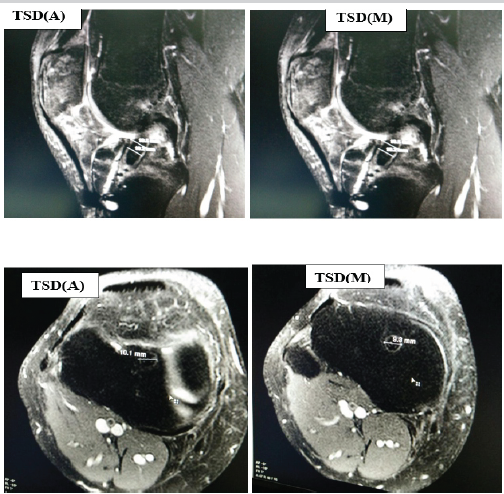
Figure 5:Tibial Socket/Tunnel diameter in both sagittal and axial plane.
In contrast to FSD, TSD/TTD measurements demonstrated a marked increase at follow-up in the Full Tibial Tunnel group compared to the All-Inside group in both axial and mid-sagittal planes. The difference in tibial tunnel widening between groups was statistically highly significant in both views (P = 0.0001).
Graft healing
Healing of the hamstring tendon autograft and its incorporation to bone socket/tunnel were assessed on MRI, and features of graft behavior were evaluated.
Table 4 compares graft fiber characteristics between the All-Inside group and the Full Tibial Tunnel group, with 30 patients in each group. Graft fiber integrity (Fig. 6a) was preserved in all patients in both groups, indicating complete graft continuity irrespective of the surgical technique used. Graft fiber laxity (Fig. 6b) was observed in 6 patients in the All-Inside group and 7 patients in the full tibial tunnel group. PCL buckling (Fig. 6c) was noted in 11 patients in the all-Inside group and 10 patients in the full tibial tunnel group (Fig. 6).
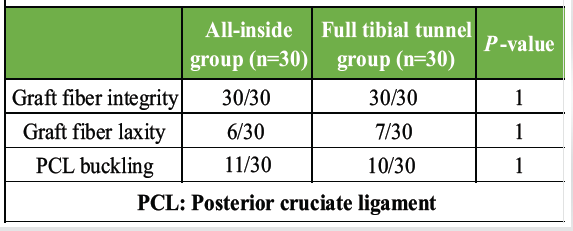
Table 4: Evaluation of graft fibres in both groups
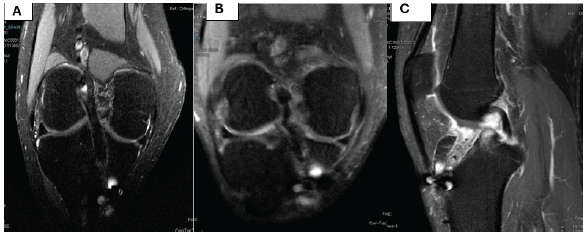
Figure 6: (a-c) Magnetic resonance imaging features of graft fibres.
Statistical analysis showed no significant difference between the two groups for any of the evaluated parameters (P = 1.00 for all), suggesting that both surgical techniques provide comparable graft fiber integrity and post-operative graft behavior.
This prospective study compared the functional and radiological outcomes of ACL reconstruction performed using the all-inside technique and the full tibial tunnel technique. To the best of our knowledge and based on the available literature, this is the first study to comprehensively evaluate and compare both clinical and radiological parameters between these two surgical techniques.
The baseline characteristics of patients, including age, gender, body mass index, and duration of follow-up, were comparable between the two groups. Functional outcomes assessed using the Lysholm knee score, subjective IKDC score, and KSS for pain and function showed no statistically significant differences, indicating equivalent subjective clinical outcomes with both techniques.
The most important finding of this study was significantly lower tibial tunnel enlargement following all-inside ACL reconstruction compared with the full tibial tunnel technique. In contrast, no statistically significant difference was observed between the two groups with respect to femoral tunnel enlargement.
The precise mechanism of femoral and tibial tunnel widening following ACL reconstruction remains incompletely understood and is believed to result from a combination of biological and mechanical factors. Biological contributors include cytokine-mediated inflammatory responses, toxic effects of degradable fixation materials, and thermal bone injury during drilling [8,9,10]. Mechanical factors include excessive graft motion within the tunnel (bungee-cord and windshield-wiper effects), increased fixation distance from the joint line, and aggressive post-operative rehabilitation protocols [11,12,13].
In the all-inside technique, both femoral and tibial sockets are created using retrograde drilling and fixed with cortical suspensory button devices, whereas the full tibial tunnel technique typically employs suspensory femoral fixation combined with tibial bioabsorbable interference screw fixation. The significantly greater tibial tunnel enlargement observed in the full tibial tunnel group suggests a relative disadvantage of interference screw fixation on the tibial side.
Retrograde drilling has been shown to result in less tunnel aperture damage compared with antegrade drilling, thereby preserving cortical bone and limiting synovial fluid ingress into the tunnel [14,15,16]. Closed bone sockets reduce exposure to synovial fluid rich in inflammatory mediators, such as tumor necrosis factor-alpha, interleukin-1 beta, interleukin-6, bone morphogenetic proteins, and nitric oxide, all of which promote osteoclastic bone resorption [9,10,17]. This biological mechanism likely accounts for the reduced tibial tunnel widening observed in the all-inside group.
Previous studies have also demonstrated that closed bone sockets created through retrograde drilling effectively preserve the tibial cortical bone. Furthermore, inside-out drilling allows more accurate tunnel placement while minimizing the risk of intra-articular tunnel rim fragmentation [18,19,20,21]. The use of closed sockets combined with press-fit graft insertion further limits synovial fluid penetration into the bone tunnel [22].
Adjustable loop cortical button devices permit closer graft–socket approximation, thereby reducing graft motion and minimizing both the bungee-cord and windshield-wiper effects. Their ability to be re-tensioned enhances initial fixation strength and improves joint stability [11,23,24]. Biomechanical studies have also demonstrated superior load-to-failure characteristics with tibial suspensory fixation compared with interference screw fixation [25].
Although interference screws provide graft compression, they may mechanically expand the tunnel during insertion and facilitate synovial fluid tracking, particularly when placed close to the joint line, thereby contributing to tunnel enlargement [26]. In addition, bioabsorbable screws containing β-tricalcium phosphate have been associated with greater tunnel widening than pure poly-L-lactic acid screws, likely due to differences in degradation kinetics and local tissue responses [27].
In the present study, both the all-inside and full tibial tunnel ACL reconstruction techniques resulted in satisfactory subjective functional outcomes. However, radiological assessment demonstrated significantly less tibial tunnel enlargement in the all-inside group, most likely attributable to the use of closed bone sockets and suspensory fixation. Reduced tunnel widening may indicate improved graft stability and potentially better objective knee stability in the all-inside group.
MRI evaluation of graft characteristics revealed preserved graft fiber integrity with complete continuity in all patients, irrespective of the surgical technique used. Graft fiber laxity and PCL buckling were also comparable between the groups, suggesting similar post-operative graft behavior. Polat et al. reported that PCL buckling can be observed even in normal knees [28]. However, several studies have described PCL buckling as a secondary sign of ACL deficiency [29,30,31,32]. Yoo and Lim demonstrated a reduction in the degree of PCL buckling following ACL reconstruction [33]. In contrast, persistent graft laxity has been associated with unresolved PCL buckling [29].
Overall, these findings are consistent with previously published literature, indicating that the all-inside ACL reconstruction technique provides clinical outcomes comparable to the full tibial tunnel technique while minimizing tibial bone loss and enhancing mechanical stability. The all-inside technique, therefore, appears to offer distinct biomechanical and radiological advantages without compromising functional results.
Both the all-inside and full tibial tunnel ACL reconstruction techniques provide comparable functional outcomes, knee stability, and graft integrity. However, the all-inside technique demonstrates significantly less tibial tunnel enlargement. Radiological advantage suggests preservation of tibial bone stock, making the all-inside technique a reliable and biomechanically favorable option without compromising clinical results.
The all-inside ACL reconstruction technique is superior to the full tibial tunnel technique with reference to post-operative pain and graft healing features, although long-term functional and radiological outcome is comparable.
References
- 1. Ntoulia A, Papadopoulou F, Zampeli F, Ristanis S, Argyropoulou M, Georgoulis A. Evaluation with contrast-enhanced magnetic resonance imaging of the anterior cruciate ligament graft during its healing process: A two-year prospective study. Skeletal Radiol 2013;42:541-52. [Google Scholar] [PubMed]
- 2. Harvey A, Thomas NP, Amis AA. Fixation of the graft in reconstruction of the anterior cruciate ligament. J Bone Joint Surg (Br) 2005;87B:593-603. [Google Scholar] [PubMed]
- 3. Johnson RJ. The anterior cruciate ligament problem. Clin Orthop 1983;172:14-8. [Google Scholar] [PubMed]
- 4. Kennedy J, Jackson MP, O’ Kelly P, Moran R. Timing of reconstruction of the anterior cruciate ligament in athletes and the incidence of secondary pathology within the knee. J Bone Joint Surg Br 2010;92-B:362-6. [Google Scholar] [PubMed]
- 5. Connaughton AJ, Geeslin AG, Uggen CW. All-inside ACL reconstruction: How does it compare to standard ACL reconstruction techniques? J Orthop 2017;14:241-6. [Google Scholar] [PubMed]
- 6. Blackman AJ, Stuart MJ. All-inside anterior cruciate ligament reconstruction. J Knee Surg 2014;27:347-52. [Google Scholar] [PubMed]
- 7. Lynch JL, Anderson K. Anterior cruciate ligament reconstruction: All-inside reconstruction. Oper Tech Sports Med 2013;21:40-6. [Google Scholar] [PubMed]
- 8. Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnel widening in anterior cruciate ligament reconstruction: A prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc 1999;7:138-45. [Google Scholar] [PubMed]
- 9. Zysk SP, Fraunberger P, Veihelmann A, Dörger M, Kalteis T, Maier M, et al. Tunnel enlargement and changes in synovial fluid cytokine profile following anterior cruciate ligament reconstruction with patellar tendon and hamstring tendon autografts. Knee Surg Sports Traumatol Arthrosc 2004;12:98-103. [Google Scholar] [PubMed]
- 10. Höher J, Möller HD, Fu FH. Bone tunnel enlargement after anterior cruciate ligament reconstruction: Fact or fiction? Knee Surg Sports Traumatol Arthrosc 1998;6:231-40. [Google Scholar] [PubMed]
- 11. Fauno P, Kaalund S. Tunnel widening after hamstring anterior cruciate ligament reconstruction is influenced by the type of graft fixation used: A prospective randomized study. Arthroscopy 2005;21:1337-41. [Google Scholar] [PubMed]
- 12. Tsuda E, Fukuda Y, Loh JC, Debski RE, Fu FH, Woo SL. The effect of soft-tissue graft fixation in anterior cruciate ligament reconstruction on graft-tunnel motion under anterior tibial loading. Arthroscopy 2002;18:960-7. [Google Scholar] [PubMed]
- 13. Rodeo SA, Kawamura S, Kim HJ, Dynybil C, Ying L. Tendon healing in a bone tunnel differs at the tunnel entrance versus the tunnel exit: An effect of graft tunnel motion? Am J Sports Med 2006;34:1790-800. [Google Scholar] [PubMed]
- 14. Kim SG, Kurosawa H, Sakuraba K, Ikeda H, Takazawa S, Takazawa Y. Development and application of an inside-to-out drill bit for anterior cruciate ligament reconstruction. Arthroscopy 2005;21:1012. [Google Scholar] [PubMed]
- 15. McAdams TR, Biswal S, Stevens KJ, Beaulieu CF, Mandelbaum BR. Tibial aperture bone disruption after retrograde versus antegrade tibial tunnel drilling: A cadaveric study. Knee Surg Sports Traumatol Arthrosc 2008;16:818-22. [Google Scholar] [PubMed]
- 16. Lubowitz JH, Schwartzberg R, Smith P. Cortical suspensory button versus aperture interference screw fixation for knee anterior cruciate ligament soft-tissue allograft: A prospective, randomized controlled trial. Arthroscopy 2015;31:1733-9. [Google Scholar] [PubMed]
- 17. Berg EE, Pollard ME, Kang Q. Interarticular bone tunnel healing. Arthroscopy 2001;17:189-95. [Google Scholar] [PubMed]
- 18. Osti M, Krawinkel A, Hoffelner T, Benedetto KP. Quantification of tibial bone loss in antegrade versus retrograde tunnel placement for anterior cruciate ligament reconstruction. Int Orthop 2015;39:1611-4. [Google Scholar] [PubMed]
- 19. Lubowitz JH, Konicek J. Anterior cruciate ligament femoral tunnel length: Cadaveric analysis comparing anteromedial portal versus outside-in technique. Arthroscopy 2010;26:1357-62. [Google Scholar] [PubMed]
- 20. Lubowitz JH, Akhavan S, Waterman BR, Aalami-Harandi A, Konicek J. Technique for creating the anterior cruciate ligament femoral socket: Optimizing femoral footprint anatomic restoration using outside-in drilling. Arthroscopy 2013;29:522-8. [Google Scholar] [PubMed]
- 21. Geeslin AG, Jansson KS, Wijdicks CA, Chapman MA, Fok AS, LaPrade RF. Tibial tunnel aperture irregularity after drilling with 5 reamer designs: A qualitative micro-computed tomography analysis. Am J Sports Med 2011;39:825-31. [Google Scholar] [PubMed]
- 22. Smith PA, Schwartzberg RS, Lubowitz JH. No tunnel 2-socket technique: All-inside anterior cruciate ligament double-bundle retroconstruction. Arthroscopy 2008;24:1184-9. [Google Scholar] [PubMed]
- 23. Smith PA, Piepenbrink M, Smith SK, Bachmaier S, Bedi A, Wijdicks CA. Adjustable- versus fixed-loop devices for femoral fixation in ACL reconstruction: An in vitro full-construct biomechanical study of surgical technique-based Tibial f ixation and graft preparation. Orthop J Sports Med 2018;6:2325967118768743. [Google Scholar] [PubMed]
- 24. Nye DD, Mitchell WR, Liu W, Ostrander RV. Biomechanical comparison of f ixed-loop and adjustable-loop cortical suspensory devices for metaphyseal femoral-sided soft tissue graft fixation in anatomic anterior cruciate ligament reconstruction using a porcine model. Art Ther 2017;33:1225-32.e1. [Google Scholar] [PubMed]
- 25. Smith PA, DeBerardino TM. Tibial fixation properties of a continuous-loop ACL hamstring graft construct with suspensory fixation in porcine bone. J Knee Surg 2015;28:506-12. [Google Scholar] [PubMed]
- 26. Buelow JU, Siebold R, Ellermann A. A prospective evaluation of tunnel enlargement in anterior cruciate ligament reconstruction with hamstrings: Extracortical versus anatomical fixation. Knee Surg Sports Traumatol Arthrosc 2002;10:80-5. [Google Scholar] [PubMed]
- 27. Wang JH, Lee ES, Lee BH. Paradoxical tunnel enlargement after ACL reconstruction with hamstring autografts when using β-TCP containing interference screws for tibial aperture fixation-prospectively comparative study. BMC Musculoskelet Disord 2017;18:398. [Google Scholar] [PubMed]
- 28. Polat A, Acar N, Aybar A, Fidan F, Özden E, Gürkan O. The correlation between posterior cruciate ligament buckling sign and meniscofemoral ligaments: A radiological study. Jt Dis Relat Surg 2021;32:371-6. [Google Scholar] [PubMed]
- 29. Rak KM, Gillogly SD, Schaefer RA, Yakes WF, Liljedahl RR. Anterior cruciate ligament reconstruction: Evaluation with MR imaging. Radiology 1991;178:553-6. [Google Scholar] [PubMed]
- 30. Boeree NR, Ackroyd CE. Magnetic resonance imaging of anterior cruciate ligament rupture. A new diagnostic sign. J Bone Joint Surg Br 1992;74:614-6. [Google Scholar] [PubMed]
- 31. Gentili A, Seeger LL, Yao L, Do HM. Anterior cruciate ligament tear: Indirect signs at MR imaging. Radiology 1994;193:835-40. [Google Scholar] [PubMed]
- 32. Oronowicz J, Mouton C, Pioger C, Valcarenghi J, Tischer T, Seil R. The posterior cruciate ligament-posterior femoral cortex angle (PCL-PCA) and the lateral collateral ligament (LCL) sign are useful parameters to indicate the progression of knee decompensation over time after an ACL injury. Knee Surg Sports Traumatol Arthrosc 2023;31:5128-36. [Google Scholar] [PubMed]
- 33. Yoo JD, Lim HM. Morphologic changes of the posterior cruciate ligament on magnetic resonance imaging before and after reconstruction of chronic anterior cruciate ligament ruptures. Knee Surg Relat Res 2012;24:241-4. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study
July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study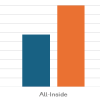 July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes
July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes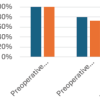 July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction
July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction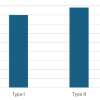 July 1, 2026 Correlation between Magnetic Resonance Imaging Modic Endplate Changes and Histopathological Inflammatory Activity in Lumbar Degenerative Disc Disease
July 1, 2026 Correlation between Magnetic Resonance Imaging Modic Endplate Changes and Histopathological Inflammatory Activity in Lumbar Degenerative Disc Disease