
Late-presenting Legg-Calvé-Perthes disease in adolescents should not preclude surgical containment from meticulous pre-operative planning and surgical management.
Dr. Mark Gamadia, Kansas City University, Kansas City, Missouri, USA. E-mail: markgamadia@gmail.com
Abstract
Introduction: Legg-Calvé-Perthes disease (LCPD) is categorized as idiopathic avascular necrosis of the femoral head, most common in children between the ages of 5 and 7. Prognosis is strongly influenced by age and lateral pillar classification, with children older than 8 years and those with Herring Group C disease typically experiencing poor outcomes. Delayed diagnosis represents a significant barrier to care, often limiting treatment options and worsening prognosis. This case highlights such a scenario while demonstrating that favorable functional and radiographic results remain achievable through meticulous surgical containment in late-presenting, severe disease.
Case Report: An 11-year-old boy with no history of trauma or systemic illness presented with an 8-month history of progressive right hip pain and a severe antalgic gait. On physical examination, he was observed to have severely restricted hip abduction and rotation. Radiographs demonstrated fragmentation, loss of sphericity, and reduced lateral pillar height of the right femoral head, consistent with Herring Group C disease. Magnetic resonance imaging confirmed avascular necrosis. Pre-operative planning targeted correction of a neck-shaft angle of 140–120° with 20° derotation. A varus derotation osteotomy of the proximal femur was performed through a lateral approach, with fixation using a plate and screws. Postoperatively, the patient was immobilized and received routine wound care. At follow-up, the patient demonstrated improved hip range of motion, resolution of the limp, and radiographic evidence of enhanced femoral head containment within the acetabulum.
Conclusion: This case shows that varus derotation osteotomy can impart functional and radiographic improvement in an 11-year-old presenting with Herring Group C LCPD. Despite traditionally poor prognostic indicators, advanced age and disease severity should not be considered absolute contraindications to surgical containment. Further research is indicated, considering the idiopathic and multifactorial etiologies associated with LCPD. Patient selection criteria should be refined and incorporate a wide array of presentations.
Keywords: Legg-Calve-Perthes disease, osteotomy, femur head necrosis, pediatric orthopedics.
Legg-Calvé-Perthes disease (LCPD) is defined by idiopathic avascular necrosis of the femoral head epiphysis in skeletally immature children. The principal goal of management is to maintain femoral head containment within the acetabulum, thereby facilitating spherical remodeling during growth and preserving long-term hip function [1]. Conservative modalities such as activity modification, physiotherapy, and bracing are most effective in younger children who present favorable prognostic features [1]. In contrast, older children and those with more advanced disease more often require surgical containment procedures, including varus derotation femoral osteotomy (VDRO), Salter innominate osteotomy, or shelf acetabuloplasty, to enhance femoral head coverage and mitigate progression of deformity [2]. Prognosis in Perthes disease is strongly influenced by both age at presentation and lateral pillar classification. Children presenting after the age of 8 years with Herring Group C involvement typically face an unfavorable outlook, characterized by minimal capacity for femoral head remodeling and a high likelihood of long-term deformity, even in the setting of surgical intervention [3,4]. We report the case of an 11-year-old boy with an 8-month history of progressive hip pain without treatment, severe limp, and antalgic gait who was diagnosed with Herring Group C Perthes disease. Despite his advanced age and significant delayed presentation, he achieved a favorable clinical and radiological outcome following a carefully planned VDRO. While surgical containment is well established in younger children, outcomes in patients older than 8 years with Herring Group C disease are generally poor, often discouraging operative intervention. This case highlights the value of timely surgical containment, illustrating that even in late-presenting, severe disease, meaningful improvement remains achievable with meticulous surgical planning.
An 11-year-old male presented with an 8-month history of right hip pain accompanied by progressive limp. He had been previously asymptomatic until the gradual onset of walking difficulty. There was no antecedent history of trauma or systemic illness. On examination, gait assessment revealed an antalgic pattern without evidence of limb-length discrepancy. Hip examination demonstrated restriction of both internal and external rotation, limited abduction, and pain elicited on movement of the hip joint. Radiographs of the pelvis with both hips demonstrated fragmentation, loss of sphericity of the femoral head, and reduced lateral pillar height, consistent with Herring Group C disease (Fig. 1). Magnetic resonance imaging of the pelvis confirmed avascular changes of the right femoral head (Fig. 2).
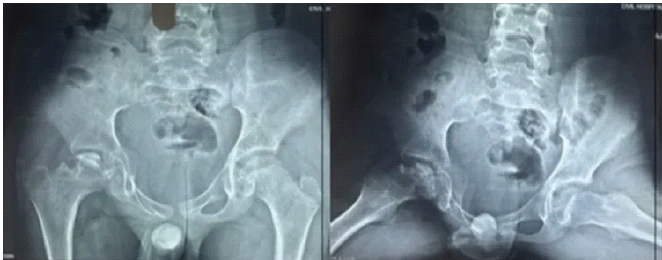
Figure 1: Pre-operative anteroposterior radiograph of the pelvis demonstrating fragmentation, loss of sphericity, and collapse of the right femoral head with reduced lateral pillar height, consistent with Herring Group C Legg-Calvé-Perthes disease.
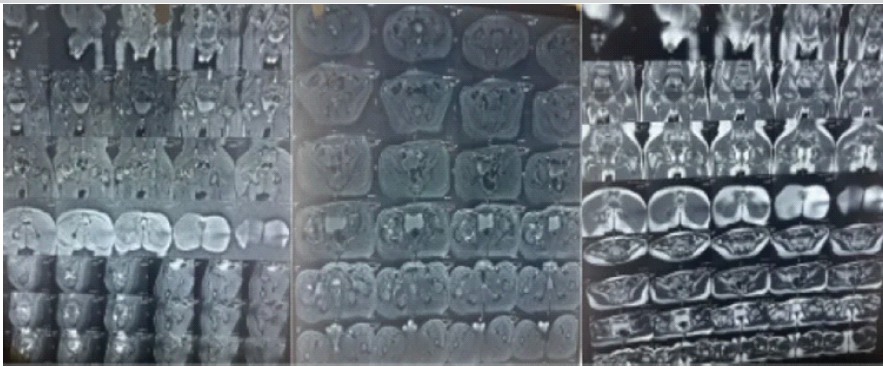
Figure 2: Magnetic resonance imaging of the pelvis with both hips. Multisequence images confirm avascular necrosis of the right femoral head with characteristic signal changes, supporting the diagnosis of Legg-Calvé-Perthes disease.
Pre-operative planning revealed a native neck-shaft angle of 140° on the right and 130° on the left, with a target post-operative neck-shaft angle of 120° on the right. Femoral anteversion measured 35° on the right and 12° on the left, necessitating 20° of derotation. The femoral shaft width was 35 mm, and the wedge size was calculated as 1.28 cm using the tangent of the desired correction angle multiplied by femoral width. A varus derotation osteotomy of the proximal femur was performed via a lateral approach through a longitudinal incision. Dissection was carried through the tensor fascia lata, with anterior reflection of the vastus lateralis muscle. The osteotomy was performed to achieve containment of the femoral head within the acetabulum, and fixation was achieved with a plate and screws (Fig. 3). Postoperatively, the patient received immobilization and routine wound care.
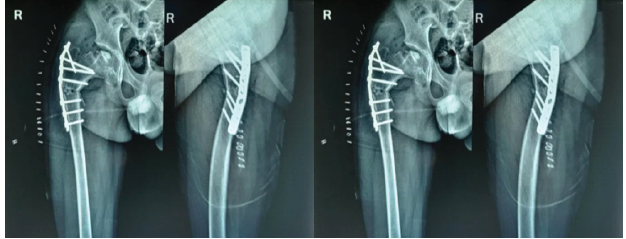
Figure 3: Immediate post-operative anteroposterior radiograph of the pelvis following varus derotation osteotomy of the right proximal femur, demonstrating improved containment of the femoral head within the acetabulum and fixation with a lateral plate and screws.
At follow-up, the patient demonstrated improved hip range of motion, resolution of the limp, and radiographic evidence of enhanced femoral head containment within the acetabulum.
LCPD is a condition in which both patient age and the degree of femoral head involvement critically determine prognosis. Children younger than 6 years typically achieve favorable outcomes with conservative management owing to their greater remodeling capacity. In contrast, those presenting after 8 years of age, particularly with Herring Group C disease, face a markedly increased risk of femoral head collapse, residual deformity, and long-term sequelae, including femoroacetabular impingement and early-onset osteoarthritis [5,6,7]. Surgical containment procedures, including VDRO, Salter innominate osteotomy, and shelf acetabuloplasty, are well-established strategies aimed at enhancing femoral head coverage and decelerating disease progression [2]. Nevertheless, the literature consistently demonstrates attenuated benefits in older children, particularly those with advanced lateral pillar collapse. In this subgroup, numerous studies have reported limited potential for remodeling and a high likelihood of unfavorable long-term Stulberg classifications, irrespective of the intervention employed [8]. The present case is notable for several factors. First, the patient was 11 years old with Herring Group C disease, a category traditionally associated with poor prognosis [4]. Second, there was an 8-month history of progressive symptoms before diagnosis, a delay generally considered to diminish the potential for favorable remodeling [1]. Nevertheless, the patient achieved meaningful clinical and radiographic improvement following timely VDRO. This outcome underscores that neither age nor delayed presentation should be regarded as absolute contraindications to surgical containment, and that carefully selected older patients may still experience substantial benefit when intervention is undertaken promptly after recognition of the disease. A central feature of this case was the meticulous pre-operative planning, which incorporated evaluation of the neck-shaft angle, femoral anteversion, degree of derotation required, and precise wedge size calculation. This individualized approach to correction likely optimized femoral head containment and contributed to the favorable clinical outcome. Consistent with this observation, the multicenter study by Herring et al. demonstrated that although patients in Herring group C typically experience poor prognoses irrespective of intervention, accurate surgical alignment remains a critical determinant of success. Similarly, evidence from Joshi et al. and the recent review by Nama et al. underscores that VDRO, when executed with careful attention to patient-specific anatomy, can improve outcomes even in late-presenting cases [9,0]. Collectively, these findings highlight the necessity of tailoring operative correction to the individual child’s morphology and projected disease course. Recent investigations have documented that VDRO can yield acceptable functional outcomes in late-presenting Perthes disease, although results remain heterogeneous and less predictable in advanced stages. In an observational quasi-prospective study of children aged 7–12 years, functional outcomes assessed by the pediatric outcome data collection instrument were generally favorable, with no statistically significant difference between early- and late-stage cohorts. However, higher scores were consistently observed in earlier stages of the disease. The present case aligns with these observations, illustrating that even in a child older than 10 years with Herring Group C disease, substantial clinical and radiographic improvement can be achieved through meticulous containment surgery [3]. Finally, this case carries substantial instructional significance. It underscores the necessity for clinicians to sustain a heightened index of suspicion for Perthes disease when evaluating older children who present with hip pain and gait disturbance, while also recognizing that surgical containment may still yield meaningful benefit in advanced, late-presenting cases. The dissemination of such reports is valuable, as they contest the therapeutic nihilism often associated with Perthes disease beyond early childhood and demonstrate that, with prompt recognition and judicious operative planning, favorable outcomes remain within reach.
VDRO continues to represent an effective containment strategy for Perthes disease in children with loss of femoral head sphericity. Although outcomes are generally unfavorable in patients older than 8 years, the present case illustrates that meaningful clinical and radiological improvement can still be achieved when the disease is promptly identified and surgically managed. Timely containment, even in late-presenting patients, may preserve hip function and potentially modify the natural course of the disease.
Physicians should suspect Legg-Calvé-Perthes for adolescents presenting with persistent hip pain and antalgic gait, as delayed treatment with this pathology can greatly impact outcomes. When managing late-presenting LCPD in older children, meticulously catering the pre-operative planning to the presenting case can yield favorable outcomes. Age and disease severity alone should not preclude surgical management, and clinical management should be specifically informed by unique case presentations.
References
- 1. Mills S, Burroughs KE. Legg-Calve-Perthes Disease. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. [Google Scholar] [PubMed]
- 2. Maleki A, Qoreishy SM, Bahrami MN. Surgical treatments for legg-calvé-perthes disease: Comprehensive review. Interact J Med Res 2021;10:e27075. [Google Scholar] [PubMed]
- 3. Lal JV, Tontanahal S, Francis J, Philip KM, Lj R, Kurian BT. Functional outcome of varus derotation osteotomy in legg-calve-perthes disease: Can it be justified in late-presenting disease? Cureus 2023;15:e49788. [Google Scholar] [PubMed]
- 4. Kollitz KM, Gee AO. Classifications in brief: The herring lateral pillar classification for legg-calvé-perthes disease. Clin Orthop Relat Res 2013;471:2068-72. [Google Scholar] [PubMed]
- 5. Herring JA, Kim HT, Browne R. Legg-calve-perthes disease. Part II: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-34. [Google Scholar] [PubMed]
- 6. Osman MK, Martin DJ, Sherlock DA. Outcome of late-onset Perthes’ disease using four different treatment modalities. J Child Orthop 2009;3:235-42. [Google Scholar] [PubMed]
- 7. Stulberg SD, Cooperman DR, Wallensten R. The natural history of legg-calvé-perthes disease. J Bone Joint Surg Am 1981;63:1095-108. [Google Scholar] [PubMed]
- 8. Caldaci A, Testa G, Dell’Agli E, Sapienza M, Vescio A, Lucenti L, et al. Mid-long-term outcomes of surgical treatment of legg-calvé-perthes disease: A systematic review. Children (Basel) 2022;9:1121. [Google Scholar] [PubMed]
- 9. Joshi N, Mohapatra SS, Goyal MP, Goyal SK, Kumar R, Saini M. Short term outcome of varus derotation osteotomy in late presenting perthes disease. Indian J Orthop 2018;52:133-9. [Google Scholar] [PubMed]
- 10. Nama KG, Bansal A, Mantri N, Meena RP, Joshi S. Functional outcome of varus derotation osteotomy in late presenting perthes disease: A case series. Int J Res Orthop 2025;11:1252-8. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases
July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis June 1, 2026 Functional Outcomes of All-Inside Arthroscopic Repair for Chronic Ankle Instability in Adolescents: A Case Series
June 1, 2026 Functional Outcomes of All-Inside Arthroscopic Repair for Chronic Ankle Instability in Adolescents: A Case Series June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework
June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework