
Even in terminal cancer, appropriate orthopedic intervention such as THA can substantially improve pain control and daily function.
Dr. Hiroki Kobayashi, Department of Orthopedic Surgery, National Defense Medical College, 3-2 Namiki, Tokorozawa, Saitama 359-8543, Japan. E-mail: supercova0205@gmail.com
Abstract
Introduction: Proper fracture management is crucial for maintaining quality of life in cancer patients with metastatic bone lesions. Subchondral insufficiency fracture (SIF) of the femoral head can lead to severe pain and functional decline. When accompanied by metastatic acetabular lesions, implant stability becomes difficult to achieve, making surgical decision-making highly complex, particularly in terminal cancer patients with limited life expectancy.
Case Report: We report an 80-year-old woman with terminal lung adenocarcinoma who developed a SIF of the femoral head and an acetabular metastatic lesion, resulting in debilitating pain and loss of mobility. After conservative treatment failed to control pain, she and her family requested surgical intervention. Total hip arthroplasty was performed using the restoration GAP II reinforcement ring combined with a cemented cup. Pain relief was immediate, and independent ambulation was achieved by post-operative week 2. Although the acetabular metastasis progressed, implant stability was preserved due to the large surface area of the reinforcement ring. The patient remained pain-free and ambulatory until her death 14 months postoperatively.
Conclusion: A careful assessment of the systemic conditions and a well-planned surgery can achieve substantial pain relief and functional restoration even in terminal cancer patients, contributing meaningfully to their quality of life.
Keywords: Locomotive syndrome, terminal cancer patients, total hip arthroplasty, metastatic acetabular lesion, subchondral insufficiency fracture.
Bone metastases occur in approximately half of all cancer patients and are a major cause of pain and pathological fractures [1]. Fracture management in terminal cancer patients with metastatic bone disease primarily aims to relieve pain and maintain quality of life (QOL). In recent years, increasing emphasis on QOL has led to more active consideration of orthopedic intervention even in patients with limited life expectancy. However, when extensive bone destruction or systemic deterioration is present, surgical decision-making requires careful assessment of the balance between surgical burden and expected functional recovery and pain relief. In particular, metastatic lesions of the acetabulum present substantial challenges due to the difficulty of achieving implant stability. We report a case of terminal lung adenocarcinoma in which a subchondral insufficiency fracture (SIF) of the femoral head with metastatic acetabular involvement caused severe pain and loss of mobility and independence. Total hip arthroplasty (THA) using the restoration GAP II reinforcement ring was performed with the aim of improving QOL. We describe the clinical course and discuss the case in the context of the relevant literature.
An 80-year-old woman with terminal lung adenocarcinoma developed left hip pain in February of year X-1. At her initial visit to our clinic in May, radiographs showed collapse of the left femoral head (Fig. 1). Magnetic resonance imaging (MRI) scans revealed a SIF (Fig. 2).
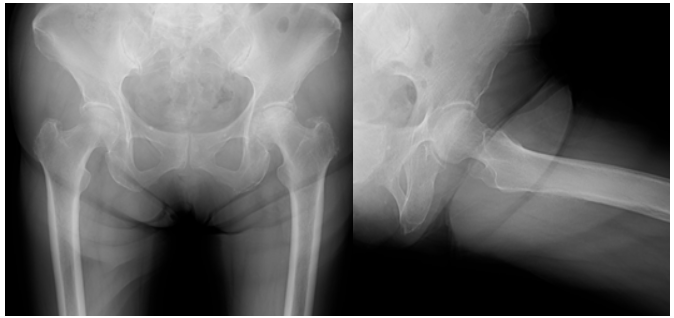
Figure 1: Radiograph at the first visit showing a subchondral fracture line in the left femoral head.
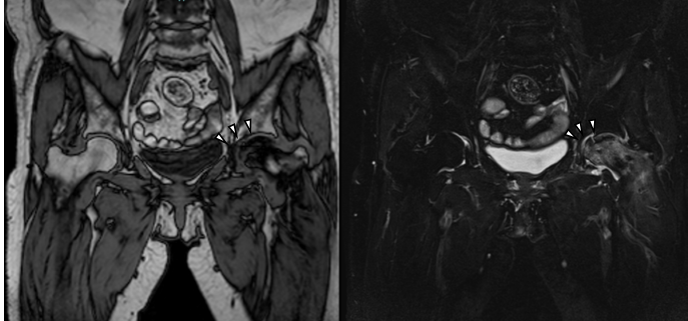
Figure 2: Magnetic resonance imaging at the initial visit. The T1-weighted image (left) shows a low-signal area in the femoral head, and the short tau inversion recovery image (right) shows a corresponding high-signal area, indicating a subchondral insufficiency fracture (arrowheads).
She had multiple metastatic brain lesions and was undergoing chemotherapy. As she was able to walk with a cane and had been diagnosed with a life expectancy of only several months, conservative treatment with analgesics was chosen.
Her symptoms gradually worsened, and in October of year X, radiographs revealed progression of femoral head collapse (Fig. 3).

Figure 3: Radiograph obtained at the time of worsening pain, demonstrating progressive collapse of the left femoral head.
Although she was able sit in a wheelchair, her pain became intolerable. The patient and her family strongly requested surgical intervention for pain relief. Pre-operative computed tomography (CT) and MRI demonstrated metastatic bone destruction involving the left acetabulum and extending toward the ischium (Fig. 4).
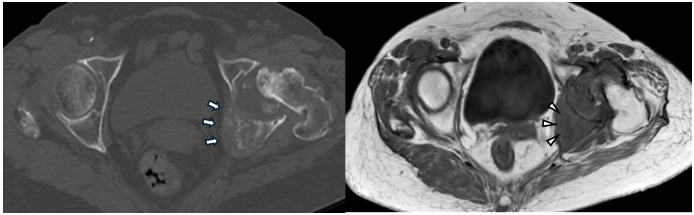
Figure 4: Pre-operative computed tomography (CT) (left, axial view) and magnetic resonance imaging (MRI) (right, axial view). The axial CT view shows osteolytic metastatic destruction extending from the acetabulum toward the ischium (arrows). The axial T1-weighted MRI view demonstrates a metastatic lesion involving the superior acetabular dome, corresponding to the weight-bearing region (arrowheads).
Because the degree of acetabular destruction made placement of a cementless cup difficult, THA using the restoration GAP II reinforcement ring and a cemented acetabular cup was planned.
THA was performed using a posterior approach. Intraoperatively, soft-tissue consistent with metastatic tumor was identified in the acetabulum and removed as extensively as possible. The GAP II ring was applied to reinforce the acetabulum, and a cemented cup was implanted (Fig. 5).
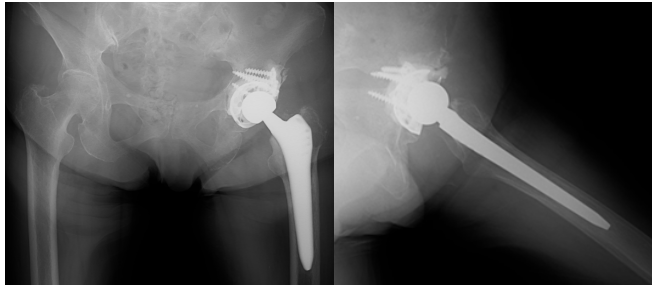
Figure 5: Post-operative radiographs showing acetabular reconstruction using the restoration GAP II reinforcement ring and a cemented cup with stable fixation.
Surgery was completed without complications. Pain relief was immediate, and gait training began the day after surgery. By post-operative week 2, the patient achieved independent ambulation. Denosumab was recommended, but the patient and her family disagreed with the administration. At 6 months postoperatively, she developed numbness and weakness in the left leg. CT showed extensive metastatic involvement of the left sacrum and ilium (Fig. 6).
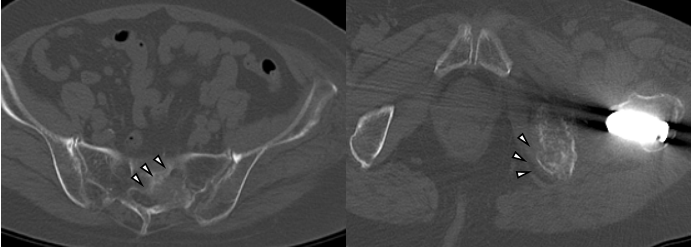
Figure 6: Computed tomography at 6 months postoperatively showing extensive metastatic involvement of the left sacrum and ilium (arrowheads).
Although acetabular osteolysis progressed and medial migration of the implant was observed (Fig. 7), construct stability was preserved, presumably due to the wide surface area of the GAP II ring.
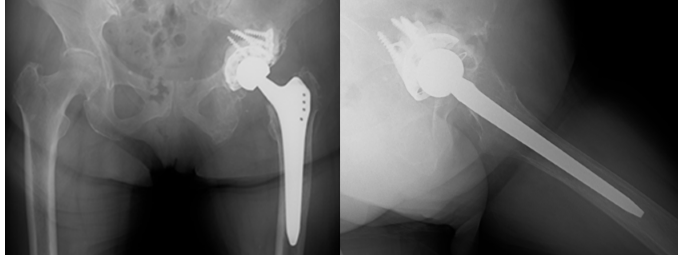
Figure 7: Radiograph at 6 months postoperatively showing medial migration of the acetabular cup and progressive osteolysis, while construct stability is preserved by the wide contact surface of the reinforcement ring.
Because she remained free of hip symptoms, denosumab and radiation therapy were initiated. At 10 months postoperatively, radiographs showed increased sclerosis around the acetabular lesion (Fig. 8).
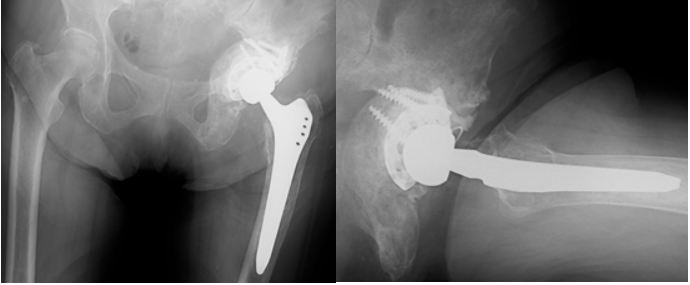
Figure 8: Radiograph at 10 months postoperatively demonstrating increased sclerosis around the metastatic acetabular lesion following adjuvant therapy.
The patient died 14 months after surgery; however, she remained independently ambulatory and did not experience recurrence of hip pain until her final days.
This case illustrates that surgical intervention, including THA, can be beneficial even for terminal cancer patients with limited life expectancy. Locomotive syndrome in cancer patients, which is defined as musculoskeletal dysfunction directly affected by cancer, related to cancer treatment, and coexisting with cancer, has been increasingly recognized as a major contributor to QOL decline in cancer patients [2]. Recent studies have demonstrated a strong association between locomotor dysfunction and reduced QOL among cancer patients [3]. Among these conditions, metastatic lesions involving the acetabulum are particularly debilitating due to severe pain and profound impairment of daily activities, which often require orthopedic intervention to alleviate the symptoms and improve QOL. Regarding surgical indications for metastatic bone disease, the report by Manabe et al. remains a key reference [4]. Major indications include intractable pain, loss of structural stability, pathological fracture or impending fracture, and prevention of neurological compromise associated with tumor progression. Unlike primary malignant bone tumors, surgical treatment for metastatic disease does not aim for oncologic cure; rather, the focus is on rapid restoration of structural stability and pain relief to allow patients to maintain independence for the remainder of their life expectancy. Hayashi et al. noted that advances in systemic cancer treatment, including molecular targeted therapy and immune checkpoint inhibitors, have extended survival in certain patients, thereby complicating and individualizing surgical decision-making [5]. With prolonged survival, the need to consider implant durability, standardized reconstruction strategies using bone defect classifications, and long-term functional expectations has increased. Nevertheless, registry data from the Scandinavian Sarcoma Group analyzing 1,195 surgically treated metastatic lesions demonstrated that surgery contributes to pain relief and functional improvement [6]. However, prognosis and complication rates depended largely on primary tumor type and lesion location. Metastatic acetabular lesions are particularly challenging to reconstruct due to the high mechanical stress borne by the hip joint. In recent years, the expansion of reconstructive options, including cages, reinforcement rings, and modular implants, has allowed surgeons to tailor procedures according to the extent of bone loss and tumor characteristics [7]. Even in hypervascular tumors such as renal cell carcinoma, THA using cement augmentation combined with a cage or large reinforcement ring has shown acceptable outcomes [8]. Recent reports on THA performed for metastatic hip disease suggest favorable functional recovery and acceptable complication rates [9]. However, Iljazi et al. reported an approximately 6% 1-year cumulative dislocation rate in THA for metastatic disease, indicating the importance of soft-tissue preservation and the use of dual mobility components to minimize the risk of dislocation [10]. The QOL of patients with skeletal metastases is often severely compromised by pain, limited mobility, reduced daily functioning, and psychological distress, as demonstrated in multiple studies [11,12]. In the present case, the patient experienced immediate pain relief after surgery and achieved independent ambulation within 2 weeks. More importantly, she maintained mobility and remained free of hip pain throughout the remaining 14 months of her life. These outcomes highlight the meaningful role orthopedic intervention can play in palliative cancer care, supporting not only symptom control but also the patient’s autonomy and dignity.
THA using a reinforcement ring provided immediate pain relief and restored functional mobility in a terminal cancer patient with metastatic acetabular destruction. Even in patients with limited life expectancy, appropriate orthopedic intervention can play a critical role in preserving dignity and QOL.
Reinforcement ring–assisted total hip arthroplasty can be an effective strategy for pain relief and mobility preservation in terminal cancer patients with acetabular metastasis.
References
- 1. Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res 2006;12 20 Pt 2:6243s-9. [Google Scholar] [PubMed]
- 2. Kawano H, Hirahata M, Imanishi J. Locomotive syndrome in cancer patients: A new role of orthopaedic surgeons as a part of comprehensive cancer care. Int J Clin Oncol 2022;27:1233-7. [Google Scholar] [PubMed]
- 3. Hirahata M, Imanishi J, Fujinuma W, Abe S, Inui T, Ogata N, et al. Cancer may accelerate locomotive syndrome and deteriorate quality of life: A single-centre cross-sectional study of locomotive syndrome in cancer patients. Int J Clin Oncol 2023;28:603-9. [Google Scholar] [PubMed]
- 4. Manabe J, Kawaguchi N, Matsumoto S, Tanizawa T. Surgical treatment of bone metastasis: Indications and outcomes. Int J Clin Oncol 2005;10:103-11. [Google Scholar] [PubMed]
- 5. Hayashi K, Tsuchiya H. The role of surgery in the treatment of metastatic bone tumor. Int J Clin Oncol 2022;27:1238-46. [Google Scholar] [PubMed]
- 6. Ratasvuori M, Wedin R, Keller J, Nottrott M, Zaikova O, Bergh P, et al. Insight opinion to surgically treated metastatic bone disease: Scandinavian sarcoma group skeletal metastasis registry report of 1195 operated skeletal metastasis. Surg Oncol 2013;22:132-8. [Google Scholar] [PubMed]
- 7. Gazendam A, Axelrod D, Wilson D, Ghert M. Emerging concepts in the surgical management of peri-acetabular metastatic bone disease. Curr Oncol 2021;28:2731-40. [Google Scholar] [PubMed]
- 8. Scoccianti G, Scanferla R, Scorianz M, Frenos F, Sacchetti F, Muratori F, et al. Surgical treatment for pelvic bone metastatic disease from renal cell carcinoma. J Surg Oncol 2023;128:653-9. [Google Scholar] [PubMed]
- 9. Tepper SC, Lee L, Kasson LB, Herbst LR, Vijayakumar G, Colman MW, et al. Hip arthroplasty outcomes in patients with metastatic bone disease. Orthop Rev (Pavia) 2024;16:94568. [Google Scholar] [PubMed]
- 10. Iljazi A, Sørensen MS, Ladegaard TH, Overgaard S, Petersen MM. Dislocation rate after hip arthroplasty due to metastatic bone disease: A retrospective cohort study evaluating the postoperative dislocation risk across different articulating solutions. Acta Orthop 2023;94:107-14. [Google Scholar] [PubMed]
- 11. Ribi K, Thürlimann B, Schär C, Dietrich D, Cathomas R, Zürrer-Härdi U, et al. Quality of life and pain in patients with metastatic bone disease from solid tumors treated with bone-targeted agents- a real-world cross-sectional study from Switzerland (SAKK 95/16). BMC Cancer 2021;21:182. [Google Scholar] [PubMed]
- 12. Rajeswaran T, Wong HC, Zhang E, Kennedy SK, Gojsevic M, Soliman H, et al. Quality of life issues in patients with bone metastases: A systematic review. Support Care Cancer 2023;32:18. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem
July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach