
A period of observation is warranted for idiopathic Congenital Dislocation of the knee (CDK). In this series, six out of seven knees reduced spontaneously, and the remaining knee required only a brief period of casting at approximately 3 months of age.
Nabil Alassaf, Department of Orthopedic Surgery, Hail Health Cluster, Hail, Saudi Arabia. E-mail: dr.nabil.alassaf@gmail.com
Abstract
Introduction: Idiopathic congenital dislocation of the knee (CDK) represents a distinct clinical category. Grade III CDK, defined as knee flexion <30° has a poor prognosis. The standard of care is “as soon as possible” manipulation and casting. Waiting for spontaneous reduction is not regarded as an accepted treatment strategy. The purpose of this study is to report on the occurrence of spontaneous reduction in idiopathic grade III CDK.
Methods: This prospective cohort study included consecutive cases of idiopathic CDK treated from April 2020 to August 2025. Inclusion criteria were: Absence of neuromuscular or genetic diseases, diagnosis of grade III CDK, and follow-up until full recovery.
Results: Seven knees in five female patients with grade III CDK were included; two had bilateral CDK. All pregnancies were full-term with cephalic presentation; one infant was delivered by cesarean section. Four neonates were firstborn. Hip ultrasound showed dysplasia in three patients, bilateral in two, and unilateral in one. Spontaneous full reduction occurred in six out of seven knees before 1 month of age. In the remaining knee, the flexion gradually improved to 30°, after which reduction was prompted by casting once for 2 weeks at 11 weeks of age. All knees attained a normal, stable range of motion. Bilateral dysplastic hips normalized spontaneously in one patient, while the other two required fewer than 6 weeks of splinting.
Conclusion: These findings suggest a potential role for observation in the management of idiopathic grade III CDK. In this cohort, all infants were non-breech, had no foot deformities, or teratologic etiology.
Significance of study: A period of observation is warranted for idiopathic CDK. In this series, six out of seven knees reduced spontaneously, and the remaining knee required only a brief period of casting at approximately 3 months of age.
Keywords: Congenital knee dislocation, idiopathic congenital dislocation of the knee, hip dysplasia, infant, children, pediatric orthopedics, treatment.
Incidence of congenital dislocation of the knee (CDK) is 1% of the incidence of developmental dysplasia of the hip (DDH) [1]. CDK encompasses several clinical presentations: It may be idiopathic or have an underlying cause, such as Larsen syndrome, arthrogryposis, myelodysplasia, or chromosomal disease. The deformity is characterized by anterior displacement, and severity is classified as follows: Grade I, simple hyperextension with more than 90° of flexion; grade II, subluxation with a maximum flexion between 30 and 90°; and grade III, true dislocation with flexion <30° [2]. CDK commonly coexists with DDH and foot deformities. Breech presentation has been classically considered as a risk factor [3]. Pre-natal diagnosis is possible [4].
Conventional wisdom is early initiation of treatment, with most authors recommending against any delay [5,6]. Serial splinting is universally employed and followed by surgery if manipulation fails. The most widely used surgical interventions are minimally invasive releases and conventional V-Y quadricepsplasty [7]. Moreover, based on their cohort of idiopathic cases, Abdelaziz and Samir advised against attempting serial casting for grade III CDK [2]. The hip is addressed when the knee has sufficient flexion for proper hip immobilization. When the degree of knee flexion is sufficient, club foot, if present, can be casted simultaneously with the knee [5,7].
Apart from the study by Haga et al., which suggested withholding treatment of isolated idiopathic CDK for 1 month to allow for spontaneous reduction, no publications considered a period of observation [8]. The aim of this report is to present seven events of spontaneous complete resolution of grade III CDK and one case requiring only minimal manipulation.
This study includes consecutive patients encountered by a single attending physician from April 2020 to August 2025. Data were collected prospectively. All neonates referred with genu recurvatum were assessed for inclusion. Eligibility criteria were: (1) Absence of neuromuscular and genetic diseases, (2) verified neonatal physical exam and radiographs indicating the diagnosis of grade III CDK, and (3) follow-up until completion of treatment. Table 1 summarizes the cases presented. The families were consented in accordance with the ethical standards set forth in the declaration of Helsinki.
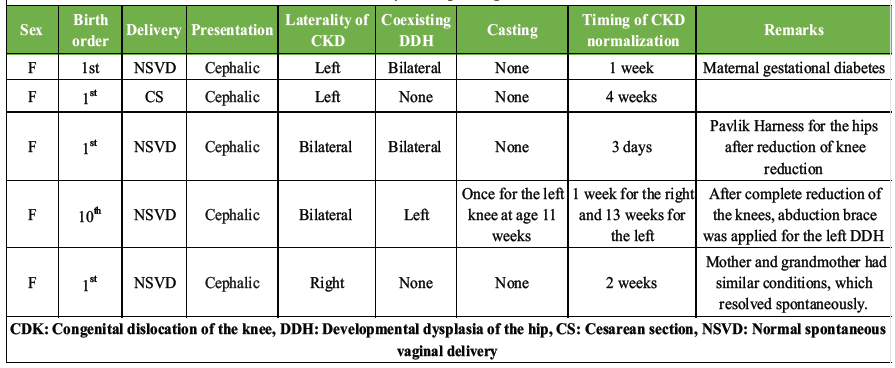
Table 1: Summary of idiopathic grade III CDK cases
Case 1
The patient was a girl, born at term (40 weeks of gestation) by normal spontaneous cephalic delivery. The mother had gestational diabetes, and the pregnancy was otherwise uneventful. Family history was negative. She was the mother’s first child. Neonatal clinical exam revealed left knee hyperextension without other overt musculoskeletal abnormalities. Left knee flexion did not go beyond neutral, and the femoral condyles were palpable posteriorly. Lower limb radiographs showed grade III left CDK (Fig. 1a). There were right Graf type 3 and left type 4 hip dysplasia in ultrasound at birth. Pavlik harness application was thwarted by the extended knee. The prognosis was initially thought to be poor. After hospital discharge, the parents noted gradual left knee improvement without any splinting or manipulation. By 1 week after birth, the knee hyperextension had completely resolved. At 1 month, follow-up examination showed that the left knee range of motion and stability were similar to the right side. Radiographs confirmed the reduction (Fig. 1b). The hips also normalized on the follow-up ultrasound without treatment. Although recurrence was not anticipated, periodic evaluations were performed.
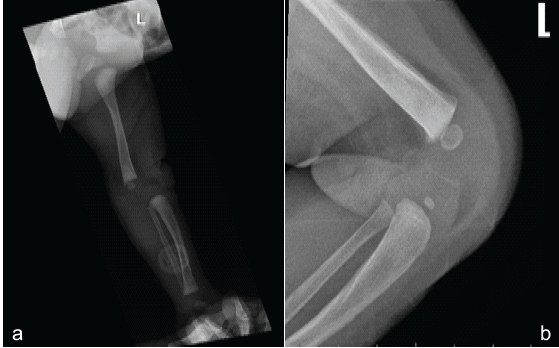
Figure 1: Case 1. (a) Left lateral knee radiograph while attempting flexion showing complete anterior translation of the tibia on the femur. (b) Left knee lateral radiograph at 1 month follow-up confirming reduction.
Case 2
This patient was a female neonate born to a primigravida by cesarean section at 39 weeks due to failure to progress. The presentation was cephalic, and the pregnancy was uneventful. Family history was non-contributory. Neonatal exam revealed left knee hyperextension, which did not flex past neutral (Fig. 2a and b). The remainder of her physical exam was normal. Radiographs confirmed the diagnosis. Ultrasound excluded DDH. The orthopedic service did not recommend manipulation or casting for the dislocated knee. The left knee reduced spontaneously before 1 month of age and was completely normal clinically and in radiographs (Fig. 2c).
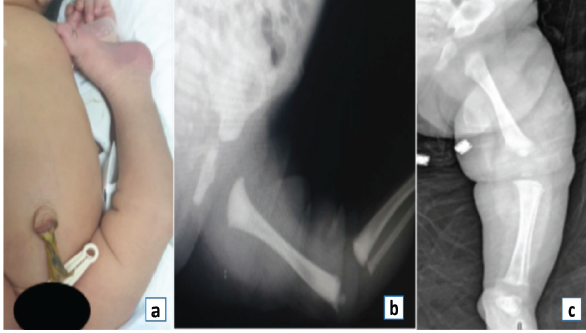
Figure 2: Case 2. (a) Clinical photograph. (b) Initial radiograph showing left knee dislocation. (c) Follow-up radiograph after spontaneous reduction.
Case 3
The patient was a firstborn female delivered uneventfully at 40 weeks of gestation. Birth was by normal spontaneous vaginal delivery in a cephalic presentation. Family history was unremarkable. Physical examination revealed bilateral hyperextended knees with no flexion possible, as confirmed in the radiographs (Fig. 3).
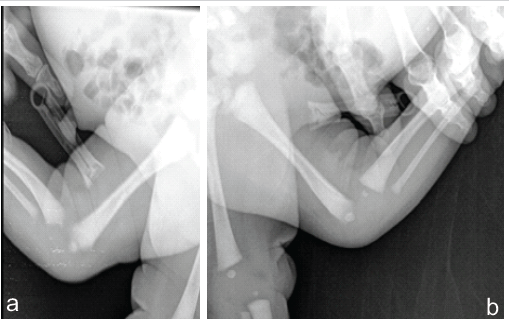
Figure 3: Case 3. (a) Initial right knee radiograph. (b) Initial left knee radiograph.
Hip ultrasound revealed right type 3 and left type 2b hip dysplasia. We opted for expectant management for the knees, which reduced within 72 h after birth. A Pavlik harness was used for 6 weeks to treat the hip dysplasia, which normalized on follow-up imaging. The knees were stable, with a full range of motion and normal alignment; therefore, follow-up radiographs for the knees were deemed unnecessary.
Case 4
The patient was a female infant born at 39 weeks of gestation by spontaneous vaginal delivery in cephalic presentation. The mother was a healthy, gravida 12, para 10. The perinatal course and family history were unremarkable. Examination revealed hyperextended knees with no flexion possible. Hip ultrasound revealed right type 2b and left type 3 DDH. No intervention was performed initially. By 1 week of age, the right knee reduced spontaneously (Fig. 4).
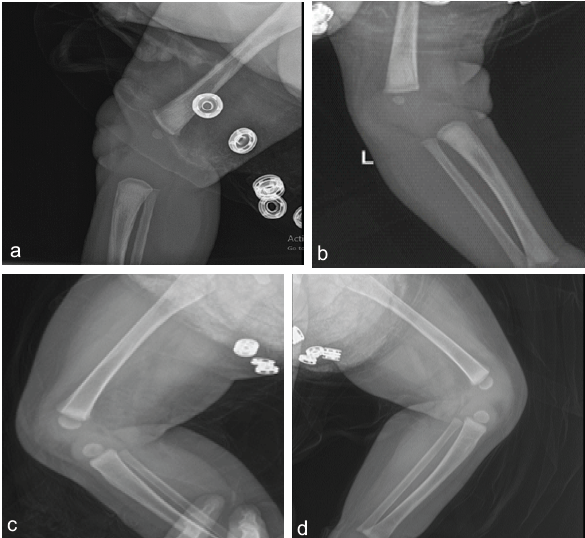
Figure 4: Case 4. (a) Right knee radiograph immediately after reduction at 1 week of age. Note anterior crease. (b) Left knee persistent dislocation. (c and d) Radiographs after a single cast application for the left knee at around 3 months of age.
The left knee continued to improve, but plateaued at around 11 weeks of age, with flexion limited to 30°. A long-leg reduction plaster of Paris cast was applied for 2 weeks; after which, the left knee normalized. The right hip dysplasia improved. After the reduction of both knees, there was residual dysplasia on the left hip, which resolved after 1 month of full-time abduction bracing.
Case 5
The patient was a term female infant born at 40 weeks of gestation by vaginal delivery in a cephalic presentation. The mother was a healthy primigravida, and the pregnancy was uneventful. The mother had unilateral knee hyperextension at birth that resolved spontaneously, and her grandmother had the condition bilaterally, which was self-limiting. On examination, there was rigid right knee hyperextension (Fig. 5a). No other findings were elicited, and DDH was not detected on ultrasound. Radiographs are shown in Fig. 5b-d. By the age of 2 weeks, the knee had reduced spontaneously.

Figure 5: Case 5. (a) Clinical photograph. (b) Maximum flexion possible. (c) Right knee radiograph. (d) The same radiograph at maximum flexion.
Non-operative management of CDK is not without risk, as closed reduction may lead to tibial plastic deformation, metaphysical fractures, physeal separation, or joint line deformity [1,7]. Roth et al. treated three patients who were born with bilateral idiopathic CDK using early serial casting. Only one knee required surgical treatment. However, all knees had a marked limitation of movement, with maximum flexion limited to 100° at follow-up [9], which is similar to an earlier report in a mixed group of patients [3]. In addition, some authors advocate manipulation in simple hyperextension and subluxation, but not for the dislocated knees [1,2]. Cheng and Ko performed a closed reduction maneuver within the first 24 h of life, followed by immobilization. All of the 13 knee subluxations were successfully reduced, and five of the six knee dislocations responded favorably. The single failed reduction was in a knee that had an associated club foot [6].
Vicente-Ferreira et al. were faced with unilateral grade I CDK in a newborn and planned serial casting, but the knee spontaneously reduced on the 3rd day of life [10]. Similarly, Borges et al. reported a case of bilateral idiopathic grade III CDK where spontaneous reduction occurred 24 h after birth [11], consistent with a case reported by Ceylan [12]. Serendipitous reduction is probably a frequent occurrence that is not adequately reported. Haga et al. proposed differentiating CDK based on the presence of associated conditions and believed that some of these cases are postural. They intentionally waited for spontaneous reductions in seven knees of six patients that had isolated idiopathic CDK without club feet. Simple hyperextension was excluded. Six knees were subluxated and only one knee was dislocated. There was one ipsilateral DDH. All had a cephalic presentation. In two knees, there was minimal splinting, but no traction or casting, and the remaining five knees were only observed. Spontaneous reduction occurred within 2 weeks in six knees, and the seventh knee reduced spontaneously at 3 months. Complete flexion was achieved in all knees after reduction, with no recurrence after a minimum follow-up of 6 months. Based on these findings, the authors recommend a 1-month observation period in isolated idiopathic CDK [8]. These recommendations have been largely overlooked.
In the present report, one patient experienced spontaneous resolution of the bilateral hip dysplasia in 1 month without treatment. This supports the timing of ultrasound screening at 1 month of age to reduce overtreatment [13]. When done during the first 3 days of life, universal ultrasound screening was positive in only 2.1% of children as per Graf classification in a study by Gyurkovits et al. [14]. In addition, four out of five patients were firstborn, which may support that increased intra-uterine pressure contributes to the development of CDK.
In the absence of club foot, breech presentation, or teratologic conditions, a few weeks of observation is advisable to allow for spontaneous reduction of CDK.
Idiopathic CDK appears to be a packaging disorder, occurring more frequently in females with cephalic presentation. A short period of observation is recommended before initiating casting.
References
- 1. Jacobsen K, Vopalecky F. Congenital dislocation of the knee. Acta Orthop Scand 1985;56:1-7. [Google Scholar] [PubMed]
- 2. Abdelaziz TH, Samir S. Congenital dislocation of the knee: A protocol for management based on degree of knee flexion. J Child Orthop 2011;5:143-9. [Google Scholar] [PubMed]
- 3. Johnson E, Audell R, Oppenheim WL. Congenital dislocation of the knee. J Pediatr Orthop 1987;7:194-200. [Google Scholar] [PubMed]
- 4. Morales-Roselló J, Loscalzo G, Hueso-Villanueva M, Buongiorno S, Jakaitė V, Perales-Marín A. Congenital knee dislocation, case report and review of the literature. J Matern Fetal Neonatal Med 2022;35:809-11. [Google Scholar] [PubMed]
- 5. Ko JY, Shih CH, Wenger DR. Congenital dislocation of the knee. J Pediatr Orthop 1999;19:252-9. [Google Scholar] [PubMed]
- 6. Cheng CC, Ko JY. Early reduction for congenital dislocation of the knee within twenty-four hours of birth. Chang Gung Med J 2010;33:266-73. [Google Scholar] [PubMed]
- 7. Shah NR, Limpaphayom N, Dobbs MB. A minimally invasive treatment protocol for the congenital dislocation of the knee. J Pediatr Orthop 2009;29:720-5. [Google Scholar] [PubMed]
- 8. Haga N, Nakamura S, Sakaguchi R, Yanagisako Y, Taniguchi K, Iwaya T. Congenital dislocation of the knee reduced spontaneously or with minimal treatment. J Pediatr Orthop 1997;17:59-62. [Google Scholar] [PubMed]
- 9. Roth S, Sestan B, Gruber B, Ledić D, Ostojić Z, Rakovac I. Bilateral congenital dislocation of the knee with ipsilateral developmental dysplasia of the hip – report of three patients. Coll Antropol 2010;Suppl 1:299-305. [Google Scholar] [PubMed]
- 10. Vicente‐Ferreira M, Ferreras C, Gomes AC, Freitas JM. Congenital dislocation of the knee with spontaneous resolution-a case report. Pediatr Int 2023;65:e15710. [Google Scholar] [PubMed]
- 11. Borges M, Barbosa L, Braglia J, Silveira I, Loureiro R. Congenital bilateral knee dislocation – a case of spontaneous reduction. Residência Pediátr 2024;14:1. [Google Scholar] [PubMed]
- 12. Ceylan HH, Elmadağ M, Erdil M, İmren Y, Bilsel K, Tuncay İ. Congenital dislocation of knee. Electron J Gen Med 2013;10:164-6. [Google Scholar] [PubMed]
- 13. Alassaf N. Universal ultrasound screening and early treatment of developmental dysplasia of the hip: A critical review. J Med Life 2024;17:755-60. [Google Scholar] [PubMed]
- 14. Gyurkovits Z, Sohár G, Baricsa A, Németh G, Orvos H, Dubs B. Early detection of developmental dysplasia of hip by ultrasound. HIP Int 2021;31:424-9. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 August 6, 2024 Traumatic Shoulder Dislocation in a Child: A Case Report
August 6, 2024 Traumatic Shoulder Dislocation in a Child: A Case Report August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report
August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases
July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases