
Post-traumatic elbow stiffness must be recognized and treated early, progressing from conservative management to surgical intervention when necessary, to restore optimal elbow function.
Dr. Priti Ranjan Sinha, Department of Orthopedics, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India. E-mail: drpritiranjansinha@gmail.com
Abstract
Introduction: Elbow movement is crucial for proper upper limb function, allowing the hand to be positioned accurately in space. However, the elbow is highly susceptible to stiffness, which can result from a variety of traumatic or non-traumatic causes. Diagnosis of elbow stiffness involves a thorough medical history and physical examination, often supported by relevant imaging studies. Managing a stiff elbow can be difficult, making prevention a key consideration. If preventive measures are insufficient, treatment typically progresses from non-surgical to surgical options. For patients presenting with mild contractures of 6 months or less, non-operative approaches such as static or dynamic splinting, serial casting, continuous passive motion, physical or occupational therapy, and joint manipulation may be utilized. When these conservative methods fail, surgical intervention, either arthroscopic or open, can be performed to remove soft tissue or bony obstacles that limit motion.
Case Report: A case report of a 15-year-old girl who developed elbow stiffness following a fall and subsequent undiagnosed fracture is presented. Despite conservative management, she experienced no significant improvement, prompting surgical intervention. The patient underwent a lateral approach to remove Heterotropic ossification and loose bodies, resulting in marked improvement in range of motion (ROM) and patient satisfaction post-operatively.
Conclusion: Post-traumatic elbow stiffness, frequently associated with heterotopic ossification, can be difficult to treat. Prompt recognition and timely intervention, whether through conservative measures or surgery, are key to achieving optimal results. In cases of severe contracture, surgical techniques such as the lateral column procedure have proven effective in restoring both ROM and overall elbow function.
Keywords: Post-traumatic elbow stiffness, heterotopic ossification, Range of motion, Rehabilitation
Post-traumatic stiffness of the elbow is relatively uncommon, occurring in roughly 5% of cases [1]. The elbow, a highly constrained synovial hinge joint, is particularly sensitive to trauma and has a strong tendency toward stiffness and degenerative changes. Its primary function is to position the hand effectively in space. Morrey et al. [2] identified the functional range of elbow motion required for daily activities as approximately 100°, including flexion-extension from 30° to 130° and pronation-supination of 50° in either direction. Even a modest loss of motion can result in functional limitations; clinically, a stiff elbow is generally defined as one with extension limited by more than 30° and flexion restricted to <120° [3]. Elbow stiffness is common due to the joint’s congruent structure, the close relationship of surrounding muscles such as the brachialis and triceps, and the frequent development of heterotopic ossification (HO).
HO
HO commonly occurs about the elbow in response to tissue trauma; this acts as a physical block to elbow motion. HO is the most common extrinsic cause of elbow contracture. Heterotopic bone or ossification is defined as the formation of mature lamellar bone in non-osseous tissues. Myositis ossificans is defined as the formation of HO in an inflammatory muscle. Periarticular calcification is defined as a collection of calcium pyrophosphates within soft tissues. Periarticular calcification lacks trabecular organization and occurs in distinct structures, such as the collateral ligaments and the capsule. Direct trauma to the elbow is the most frequent cause of HO in this region. Other contributing factors include injuries to the neural axis, thermal burns, and the rare genetic condition fibrodysplasia ossificans progressiva. The likelihood of developing HO appears to increase with the severity of the injury. In a study of isolated elbow dislocations, Thompson and Garcia reported an HO incidence of 3%. However, when the dislocation was accompanied by a nearby fracture or a radial head fracture, the incidence rose to 16% and 20%, respectively. This indicates that the risk of HO is approximately 5 times higher when a fracture occurs in conjunction with an elbow dislocation [4]. Post-traumatic elbow stiffness develops through a sequence of four stages: bleeding, edema, granulation, and fibrosis [5]. Stiffness can range from mild to severe and may significantly affect the patient’s quality of life due to pain and limitations in daily activities [6,7].
Classification
The two primary elbow stiffness classification systems are those of Jupiter and Morrey [8,9]. While Kay’s classification is based on the structure impeding elbow motion, Morrey’s classification is based on the etiology and its anatomic location [9]. Kay’s five-part classification system includes soft-tissue contracture (type I), soft-tissue contracture with ossification (type II), non-displaced articular fracture with soft-tissue contracture (type III), displaced intra-articular fracture with soft-tissue contracture (type IV), and post-traumatic bony bars (type V) [9]. Morrey’s three-part system classifies elbow stiffness as extrinsic, intrinsic, or mixed [8,9]. Extrinsic stiffness is due to extra-articular causes, including capsular, collateral ligament, and muscle contractures, as well as HO and extra-articular malunions. Intrinsic stiffness is due to intra-articular adhesions, loose bodies, osteophyte formation, or malalignment of the articular surface. Extrinsic contractures developing as a result of intrinsic pathology are classified as mixed. Hastings and Graham developed a classification system of HO based on functional limitation [10]. Class I includes radiographically evident HO but without functional limitation. Class II includes a limited, yet functional, range of elbow motion. Class II can be subdivided into IIA, IIB, and IIC. Limitation in the flexion-extension plane is IIA, limitation in the pronation-supination plane is IIB, and limitation in both planes is IIC. Class III includes ankylosis of the particular articulation. Class III can be subdivided into A, B, and C, in the same manner as Class II. Evans noted that bridging bone in one plane is amenable to excision with good functional return and low recurrence rate, whereas synostoses in two or more planes showed diminished results [11]. A stiff elbow is challenging to treat; therefore, its prevention is of paramount importance. The loss of soft-tissue compliance that leads to elbow contracture results from bleeding, edema, granulation tissue formation, and ultimately fibrosis [12]. Splinting the elbow in full extension postoperatively creates sufficient pressure within tissues around the elbow to minimize bleeding and resist extravasation of fluid [8,12,13]. Continuous passive motion (CPM) applied to the elbow immediately postoperatively and continued for 3–4 weeks until soft-tissue swelling is controlled, drives fluids away from the joint and periarticular tissues, thus minimizing the cascade of events leading to soft-tissue contracture [8,12]. However, a requisite for splinting in extension and post-operative CPM is stable post-operative bony and soft-tissue support of the elbow.
A 15-year-old previously healthy girl, a student, presented to our orthopedic outpatient clinic with complaints of persistent pain, stiffness, and decreased range of movement in her left elbow for the last 4 months. She had an alleged history of trauma following a slip and fall on her left elbow. After the trauma, she developed pain and swelling in her left elbow. She was taken to a local quack, where she was informed that her elbow was dislocated (undocumented), and a reduction was done. There is a history of continuous massaging and bandaging for 1.5 months, with intervals of 4–5 days. The symptoms did not resolve over the subsequent weeks, and the child continued to experience discomfort and stiffness and was unable to perform her daily living activities with her left hand, which is non-dominant. After 4 months of trauma, when she came to our outpatient department, a proper clinical examination was done. Patient was able to flex her left elbow from 50° 90°. Moreover, pronation was painful and restricted by 10°. Neurological examination was done over the bilateral upper limbs. All nerves were intact bilaterally. Neurological examination was confirmed via the autonomous zone. A plain radiograph was done of the bilateral elbow, anteroposterior and Lateral views. X-ray of left elbow reveals slight heterotrophic ossifications over the distal humerus and a malunited medial epicondyle fracture with a coronoid fracture. Patient was advised for conservative management via dynamic splinting, CPM, occupational/physical therapy, and manipulation. After 3 months (7 months from the trauma), the patient did not get any relief. Despite undergoing a regimen of home exercises and anti-inflammatory medication, there was no significant improvement in her range of motion (ROM). So again she came to our hospital with the same complaint of stiffness and difficulty in doing activities of daily living. Surgery is generally considered after 3–6 months of structured conservative management (physiotherapy, splinting, CPM, and anti-inflammatory therapy) without significant improvement in ROM. The patient had a flexion-extension arc of 40° after more than 3 months of supervised conservative therapy, along with imaging evidence of HO and intra-articular loose bodies. Severe motion restriction, functional impairment, and mechanical obstruction, surgical intervention was clearly justified. From a cost-effectiveness perspective, prolonged conservative management of post-traumatic elbow stiffness can incur substantial indirect costs, including repeated physiotherapy sessions, splinting devices, pain medications, and loss of productivity, especially when functional recovery remains limited. Early surgical intervention, particularly in patients who demonstrate poor response to standardized conservative therapy within 3–6 months, may involve higher upfront costs but often results in faster restoration of ROM, reduced need for ongoing therapy, and earlier return to daily activities and work. Therefore, in select patients, timely surgical release can be cost-effective by shortening overall treatment duration and minimizing long-term disability-related costs. Bilateral elbow X-rays (anteroposterior and lateral) (Fig. 1) and bilateral upper limb scanogram were done (Fig. 2). All necessary routine investigations were done. Rheumatoid factor value is 2.54 IU/mL (negative), and CRP value is 1.53 mg/L (negative).
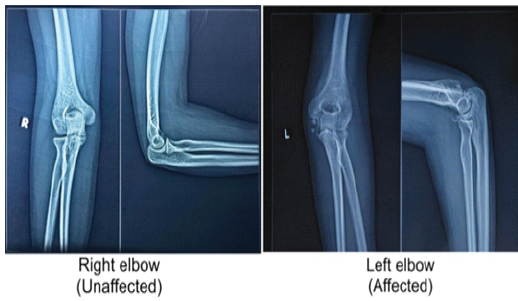
Figure 1: Pre-operative X-ray of the bilateral elbow joint shows heterotopic ossification on the posteromedial aspect of the distal humerus on the left side.
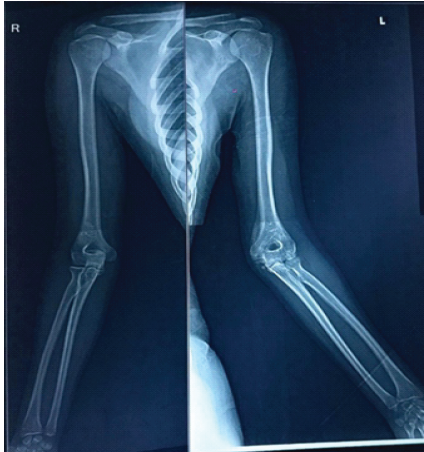
Figure 2: Scanogram of bilateral upper limb.
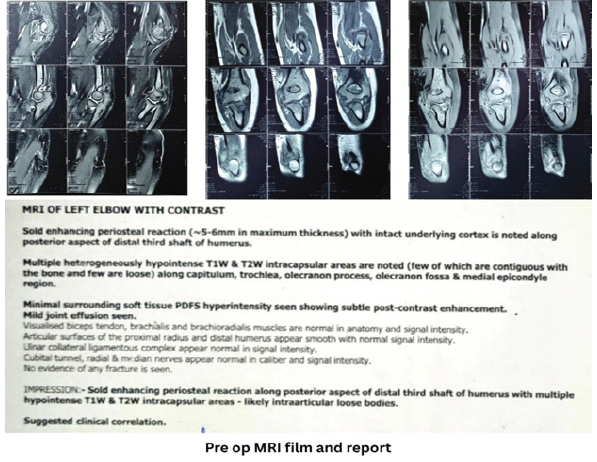
Contrast magnetic resonance imaging of the left elbow was done, which showed a solid enhancing periosteal reaction along the posterior aspect of the distal third of the humerus with multiple hypointense intra-articular loose bodies.
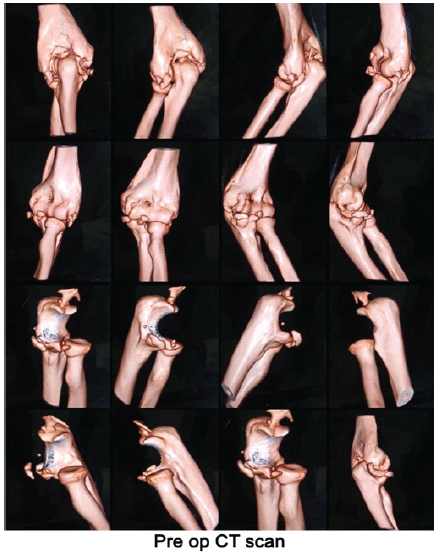
Pre-operative computed tomography scan with 3D reconstruction shows mature peri-articular HO predominantly involving the posterior aspect of the distal humerus and olecranon fossa, extending anteriorly to the coronoid region. The largest ossified mass measures approximately 3 cm in maximum dimension on the posterior side. There is partial bridging across the ulnohumeral joint, causing a mechanical block without complete ankylosis. A bony bridge is also present between the distal humerus and ulna, with findings consistent with Hastings Grade IIC heterotopic ossification.
 Operative options
Operative options
Various approaches can be utilized to release the contracted elbow. The anterior approach was described by Urbaniak and colleagues in 1985 [14]. The medial “over-the-top” approach was described by Kasparyan and Hotchkiss in 1997 [15]. The lateral approach (column procedure) was described by Morrey in 1990 [9].
The anterior approach allows access to the anterior capsule, brachialis muscle, and biceps tendon; however, the neurovascular structures must be manipulated. One must be certain that no posterior pathology is present, as the olecranon fossa cannot be visualized with the anterior approach. The anterior approach should be used for extrinsic contractures that limit extension. Flexion should be >120°. Radiographically, the joint surface should be essentially normal [14]. The medial “over-the-top” approach can also be used for the release of elbow contracture. The medial approach is preferred if the ulnar nerve requires exploration or release, there is a significant lack of flexion, or if there are osteophytes present along the posterior medial joint line. Limits in both extension and flexion can be addressed with this approach. Disadvantages of the medial approach include difficulty in removing heterotopic bone on the lateral aspect of the joint, and the medial approach provides poor access to the radial head [15]. If forearm rotation is limited, then the lateral column procedure is preferred. The lateral approach (column procedure) can also be used for the release of elbow contracture. The lateral approach is preferred for patients with at least 40° loss of extension and for those with restricted forearm motion. Extrinsic pathology that has minimal articular surface change responds well to the lateral approach. However, the medial approach is preferred in cases of ulnar nerve dysfunction or extensive medial HO. The column procedure consists of elbow arthrotomy, release of anterior and posterior capsules, and excision of osteophytes [9]. Alternative surgical options for post-traumatic elbow stiffness include arthroscopic release, which allows minimally invasive debridement and capsulotomy but entails greater technical demand and a higher risk of neurovascular injury, and combined medial-lateral open approaches, which provide extensive exposure for excision of HO, release of the anterior and posterior capsules, and removal of osteophytes. In this case, the lateral column (open) approach was preferred due to predominant loss of extension and extrinsic pathology, while medial or combined approaches could be considered if significant ulnar nerve involvement, severe flexion loss, or extensive medial HO were present.
Surgical procedure
Preoperative range of movement was seen in Fig. 3.
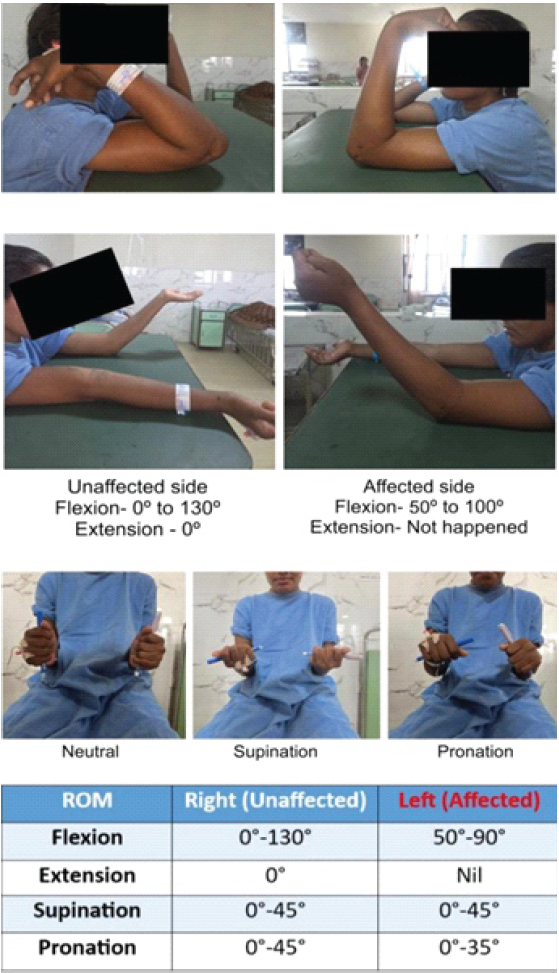
Figure 3: Pre-operative range of movement of the bilateral elbow joint.
For this purpose, a lateral approach was used. The patient was placed in the supine position on the operating table with a sandbag under the ipsilateral shoulder. Approx 10–12 cm curved incision was given from the lateral epicondyle to the radial head. Superficial fascia and deep fascia were dissected. Proximally dissection was carried out on the supracondylar ridge. Brachialis was elevated from the anterior joint capsule. Retractors were placed deep to the brachioradialis and brachialis to expose the joint capsule. The ulnar nerve was carefully identified and protected throughout the procedure. Prophylactic transposition was not performed, as there was no pre-operative neuropathy or extensive medial pathology. Anterior capsulotomy was performed from the lateral to the medial direction. Triceps were elevated from the posterior aspect of the humerus to expose the joint capsule. Posterior capsulotomy was performed from the lateral to the medial direction [16]. HO over the posterior aspect of the distal humerus, and loose bodies were removed (Fig. 4a and b). Subsequently, flexion and extension were assessed, but no movement was achieved within an acceptable range. Hence, some part of the extensor bundle was incised with cautery at the lateral epicondyle (Fig. 4c). After that, flexion and extension were checked on the operating theater table (Fig. 5).
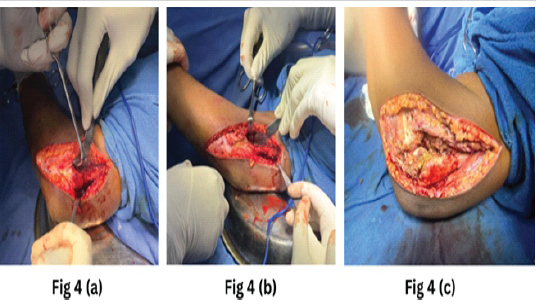
Figure 4: (a) Heterotopic ossification over the posterior aspect of the distal humerus was dissected and removed. (b) The loose tissue over the left elbow joint was removed. (c) To correct extension, some extensor insertions over the lateral epicondyle were removed with cautery.
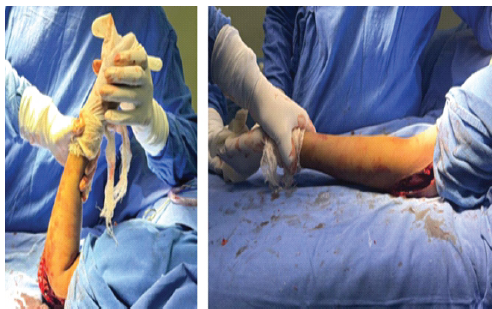
Figure 5: Intraoperatively, flexion and extension movements were checked after operation theatre procedure.
Post-operative care
After this procedure, the above-elbow slab was applied in full extension. Post-operative X-ray was done. In post-operative X-ray, heterotrophic ossifications and loose bodies were fewer compared to pre-operative X-ray (Fig. 6a & b).
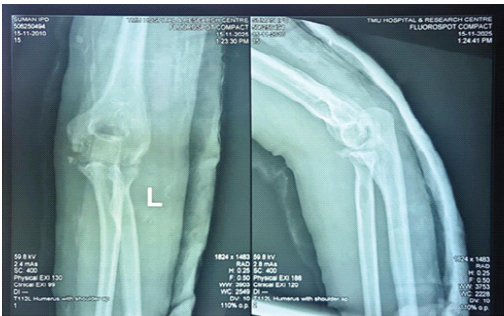
Figure 6: Post-operative X-ray of the left elbow with a slab was done.
Indomethacin 25 mg was administered every 8 h for 3 weeks. After 3 days of operation CPM exercise was done every 2 h. A CPM machine was used for 12 h a day for 1 week. Active and passive ROM exercises were performed hourly using the turn buckle splint (Fig. 7 and 8).
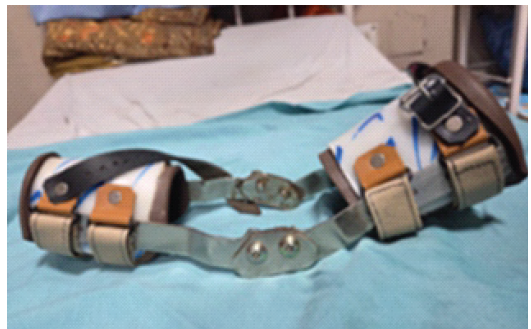
Figure 7: Turn buckle splint.

Figure 8: A turn buckle splint was given in flexion and extension in an intermittent pattern.
After 2 weeks of surgery, her elbow movement displayed improvement even without a turn buckle splint (Fig. 9), and sutures were removed after 2 weeks. At 6 weeks, daytime splinting is discontinued, whereas nighttime splinting is continued for an additional 6 weeks.

Figure 9: Range of movement at 2 weeks after operation.
The patient reported high satisfaction with the post-operative outcome. The Quick Disability of the Arm, Shoulder, and Hand score improved significantly from 56 preoperatively to 2 at final follow-up. Pain levels decreased from a visual analog scale score of 3 preoperatively to 0 postoperatively, with no pain reported during daily activities. No side effects or complications were observed from the time of surgery through the 6-month follow-up period. The Mayo elbow performance score improved markedly from 55 (Fair) preoperatively to 100 (Excellent) postoperatively. The patient underwent a structured 12-week conservative management program consisting of supervised physiotherapy 3 times/week (45–60 min/session), a daily home exercise regimen performed 3–5 times/day, dynamic splinting for 6–8 h daily, and CPM therapy for approximately 1.5–2 h/day; compliance was monitored through regular follow-up visits.
The elbow range of movement was shown at 3 months of follow-up in Fig. 10, and post-operative X-ray at 6 months of follow-up was shown in Fig. 11.

Figure 10: Range of movement at 6 months follow-up.

Figure 11: X-ray left elbow at 6 months follow-up.
X-ray at 1-year follow-up shows no HO, and clinically, there is full ROM with a satisfied patient, as shown in Fig. 12.
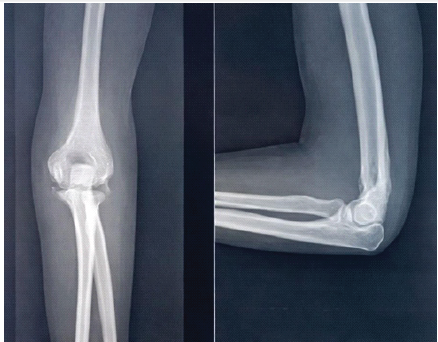
Figure 12: X-ray lest elbow at 1-year follow-up.
Delayed treatment has been described by Sing et al., who presented 10 weeks after injury [17]. In the current report, our patient presented to the local hospital emergency department immediately following the injury; the fracture remained undetected, resulting in a malunion of the fracture fragment, a finding also reported by Elmaraghy et al. If a fracture is left undetected, it may result in severe limitation of ROM due to malunion [18]. Kruse et al. Reported on 36 patients with stiff elbows who underwent a lateral-column approach combined with posterior mini-open access, with an average follow-up of 38 months. All patients showed improvements in their ROM. For those with post-traumatic contractures, elbow flexion improved from 99° to 128° at the final follow-up, while those with degenerative elbow contractures improved from 98° to 126°. Similarly, extension improved from an average of 52–19° in the post-traumatic group and from 41° to 17° in the degenerative stiffness group. The average gain in flexion-extension across both groups was 57° [19]. Ring et al. Conducted a study involving 46 participants with post-traumatic stiff elbows who underwent capsulotomy. The results showed an improvement in elbow arc to nearly 100°. Additional surgery is needed in 14 patients with persistent elbow contracture, ulnar neuropathy, or both, and gives additional improvement in ROM (±26°) [20]. To reduce the risk of recurrence, prophylactic measures such as nonsteroidal anti-inflammatory drugs, particularly indomethacin, or postoperative radiation therapy have been recommended [10]. Post-operative complications after elbow contracture release may include recurrence of HO, elbow instability, infection, and nerve injury, particularly involving the ulnar nerve. However, careful surgical technique and prophylactic measures minimize these risks [10,19,20]. Another potential complication is Elbow Instability, which may occur following extensive capsular release or disruption of the stabilizing ligamentous structures of the elbow. Instability is particularly associated with aggressive surgical releases, in which the collateral ligaments or important bony stabilizers are compromised [20].
Post-operative Surgical Site Infection is relatively uncommon but remains a significant concern after elbow surgery. The incidence of infection following elbow contracture release has been reported to range from 1% to 5% [1,19]. Jeevannavar et al. reported a case of a 20-year-old woman with a malunited capitellum fracture who underwent corrective osteotomy and internal fixation using a Herbert screw, giving a good result with a functional elbow and absence of pain [21]. Although the use of 3D printing models is currently limited, it demonstrates considerable potential for broader adoption. These technologies are expected to improve, allowing for more realistic analyses of complex scenarios even on lower-spec devices [22]. We believe that 3D-printed models could be invaluable for surgeons in visualizing complex anatomy and selecting the most appropriate treatment or surgical strategy for a post-traumatic stiff elbow. However, further research with larger sample sizes is necessary to validate these benefits.
Summary
Elbow contractures can be categorized as intrinsic or extrinsic in origin. Post-traumatic stiffness is the most common intrinsic cause, whereas HO is the leading extrinsic contributor. Patients who experience significant elbow trauma and possess risk factors for HO should receive prophylactic treatment, such as indomethacin or radiation therapy, to prevent HO formation. Early surgical removal of HO is both safe and effective. Non-operative treatments are most beneficial when initiated within 6 months of contracture onset and typically involve physical therapy combined with an intensive splinting regimen. If these conservative approaches fail and the patient continues to experience functionally limiting loss of motion, surgical intervention may be indicated. Pre-operative evaluation of the ulnar nerve is essential, as transposition may be required during surgery. Arthroscopic releases of elbow contractures have demonstrated satisfactory outcomes but are technically demanding and carry a risk of significant neurovascular complications. Open surgical procedures have also yielded favorable results. The choice of surgical approach is guided by the primary direction of motion limitation, the presence of ulnar nerve involvement, and the location of osteophytes.
Post-traumatic elbow stiffness, frequently associated with HO, is an uncommon but functionally limiting condition. Early recognition and structured conservative management, including splinting, CPM, and physiotherapy, are most effective when applied within the first 6 months following injury. In patients who fail to achieve functional improvement despite standardized conservative therapy, timely surgical intervention, such as the lateral column procedure, can substantially restore ROM and improve patient outcomes. Prophylactic measures, including indomethacin or radiation therapy, are recommended for patients at high risk of HO formation. However, as this report describes a single case, these observations are descriptive, and no definitive conclusions regarding causality or the superiority of conservative versus surgical management can be drawn. Further studies with larger cohorts are necessary to establish evidence-based guidelines for optimal management.
Early diagnosis and timely non-operative management are key in post-traumatic elbow stiffness. When conservative treatment fails, surgical release, especially the lateral column approach combined with proper HO prophylaxis and rehabilitation, can effectively restore elbow function.
References
- 1. Nandi S, Maschke S, Evans PJ, Lawton JN. The stiff elbow. Hand (N Y) 2009;4:368-79. [Google Scholar] [PubMed]
- 2. Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Jt Surg Am 1981;63:872-7. [Google Scholar] [PubMed]
- 3. Sojbjerg JO. The stiff elbow. Acta Orthop Scand 1996;67:626-31. [Google Scholar] [PubMed]
- 4. Thompson HC 3rd, Garcia A. Myositis ossificans: Aftermath of elbow injuries. Clin Orthop Relat Res 1967;50:129-34. [Google Scholar] [PubMed]
- 5. Adolfsson L. Post-traumatic stiff elbow. EFORT Open Rev 2018;3:210-6. [Google Scholar] [PubMed]
- 6. Vardakas DG, Varitimidis SE, Goebel F, Vogt MT, Sotereanos DG. Evaluating and treating the stiff elbow. Hand Clin 2002;18:77-85. [Google Scholar] [PubMed]
- 7. Myden C, Hildebrand K. Elbow joint contracture after traumatic injury. J Shoulder Elbow Surg 2011;20:39-44. [Google Scholar] [PubMed]
- 8. Jupiter JB, O’Driscoll SW, Cohen MS. The assessment and management of the stiff elbow. Instr Course Lect 2003;52:93-111. [Google Scholar] [PubMed]
- 9. Morrey BF. Post-traumatic contracture of the elbow. Operative treatment, including distraction arthroplasty. J Bone Joint Surg Am 1990;72:601-18. [Google Scholar] [PubMed]
- 10. Hastings H 2nd, Graham TJ. The classification and treatment of heterotopic ossification about the elbow and forearm. Hand Clin 1994;10:417-37. [Google Scholar] [PubMed]
- 11. Evans EB. Heterotopic bone formation in thermal burns. Clin Orthop Relat Res 1991;263:94-101. [Google Scholar] [PubMed]
- 12. O’Driscoll SW, Giori NJ. Continuous passive motion (CPM): Theory and principles of clinical application. J Rehabil Res Dev 2000;37:179-88. [Google Scholar] [PubMed]
- 13. Bain GI, Mehta JA, Heptinstall RJ. The dynamic elbow suspension splint. J Shoulder Elbow Surg 1998;7:419-21. [Google Scholar] [PubMed]
- 14. Urbaniak JR, Hansen PE, Beissinger SF, Aitken MS. Correction of post-traumatic flexion contracture of the elbow by anterior capsulotomy. J Bone Joint Surg Am 1985;67:1160-4. [Google Scholar] [PubMed]
- 15. Kasparyan NG, Hotchkiss RN. Dynamic skeletal fixation in the upper extremity. Hand Clin 1997;13:643-63. [Google Scholar] [PubMed]
- 16. Azar FM, Beaty JH, editors. Shoulder and elbow injury. Anterior and posterior release of elbow contracture. In: Campbell’s Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021. p. 2416. [Google Scholar] [PubMed]
- 17. Singh AP, Dhammi IK, Jain AK, Jain S. Neglected isolated fracture of the trochlea humeri. Chin J Traumatol 2010;13:247-9. [Google Scholar] [PubMed]
- 18. Elmaraghy A, Pennings A, Walton C. Unrecognized isolated medial trochlear fracture leading to malunion: A case report. JBJS Case Connect 2016;6:e8. [Google Scholar] [PubMed]
- 19. Kruse KK, Papatheodorou LK, Weiser RW, Sotereanos DG. Release of the stiff elbow with mini-open technique. J Shoulder Elbow Surg 2016;25:355-61. [Google Scholar] [PubMed]
- 20. Ring D, Adey L, Zurakowski D, Jupiter JB. Elbow capsulectomy for posttraumatic elbow stiffness. J Hand Surg Am 2006;31:1264-71. [Google Scholar] [PubMed]
- 21. Jeevannavar SS, Shenoy KS, Daddimani RM. Corrective osteotomy through the fracture site and internal fixation with headless screws for type I (Hahn-Steinthal) capitellar malunion. BMJ Case Rep 2013;2013:bcr2013009230. [Google Scholar] [PubMed]
- 22. Prakoso AT, Basri H, Adanta D, Yani I, Ammarullah MI, Akbar I, et al. The effect of tortuosity on the permeability of a porous scaffold. Biomedicines 2023;11:427. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Enhancing Functional Outcomes in Distal End Radius Fracture Rehabilitation
January 1, 2026 Enhancing Functional Outcomes in Distal End Radius Fracture Rehabilitation June 1, 2026 Comparative Analysis of Functional Outcomes in Robotic-assisted versus Conventional Total Knee Arthroplasty
June 1, 2026 Comparative Analysis of Functional Outcomes in Robotic-assisted versus Conventional Total Knee Arthroplasty June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework
June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework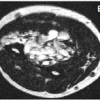 June 1, 2026 Zoledronic Acid in the Management of Melorheostosis of Radius and Ulna – A Rare Case Report with Literature Review
June 1, 2026 Zoledronic Acid in the Management of Melorheostosis of Radius and Ulna – A Rare Case Report with Literature Review