
Stability of chronic syndesmotic injury is better restored with dual-screw fixation, especially in high, physically demanding patients.
Dr. Aya Ewida, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates. E-mail: U20100787@sharjah.ac.ae
Abstract
Introduction: Ankle syndesmotic injuries present a major challenge due to their high biomechanical complexity and high risk of instability if not properly managed. There remains a controversy between the use of single versus double-screw fixation, Tight Rope fixation, arthrodesis, and ligament reconstruction, particularly in chronic or high physical demand cases.
Case Report: A 25-year-old male presented to our trauma center after sustaining a bimalleolar fracture of the left ankle with chronic syndesmotic injury, lasted for 5 months, after a motorcycle accident. Initially, open reduction with internal fixation and single syndesmotic screw fixation was done. However, anterior subluxation of the syndesmotic joint was evident on computed tomography scan post-operatively, which necessitated revision surgery, after 1 week, with dual screw fixation to restore joint alignment.
Conclusion: Dual-screw syndesmotic fixation provided superior outcomes in comparison to single-screw in patients with chronic injury and high-instability risk. This approach, if routinely done in selected cases, may reduce the incidence of recurrent instability and therefore the need for revision surgeries, as well as improve long-term functional outcomes.
Keywords: Chronic syndesmotic injury, ankle injury, tibiofibular syndesmosis, Dual-screw fixation, case report.
Ankle fractures involving syndesmotic disruption account for approximately 10–20% of all ankle fractures, with the incidence rising with high-energy trauma and young athletic populations [1]. Such injuries present a major challenge due to both their biomechanical complexity and potential for long-term instability if not properly addressed. The syndesmotic ligaments, particularly the anterior inferior tibiofibular ligament, contribute significantly to ankle stability. When disrupted, even subtle diastasis can lead to altered load transmission, early osteoarthritis, and impaired functional outcomes [2]. The syndesmotic screw stabilization method remains one of the most commonly used fixation techniques. However, the optimal number of screws required for syndesmotic fixation remains controversial, with ongoing debate in orthopedic literature over whether a single screw provides sufficient stability or if dual-screw fixation offers better long-term outcomes [3]. An alternative gaining popularity is suture-button fixation, commonly referred to as Tight Rope fixation. This technique offers advantages, such as allowing physiological micromotion at the syndesmosis, reducing the need for routine implant removal, and providing quicker rehabilitation timelines [1,2]. Despite its advantages, this technique can be more technically challenging, incur higher costs, and may lead to issues, such as soft tissue discomfort or displacement of the implant [2]. Compared to screws, Tight Rope may be especially beneficial in dynamic syndesmotic instability, but long-term outcomes remain under active investigation. Chronic syndesmotic injuries (CSIs), defined as syndesmotic disruptions lasting longer than 6 weeks after the initial trauma with ongoing pain, functional impairment, or mechanical instability, are particularly vulnerable to fixation failure if not properly fixed during primary surgery [4]. This definition aligns with the European Society for Sports Traumatology, Knee Surgery and Arthroscopy (ESSKA) – Ankle and Foot Associates consensus guidelines, which emphasize imaging-confirmed diastasis and persistent functional impairment, with chronic instability typically detected after the acute phase using stress radiographs, computed tomography (CT), or magnetic-resonance imaging (MRI) [5]. In this case report, we present a 25-year-old male with a history of prior medial malleolar fixation who sustained a bimalleolar fracture with CSI following a motorcycle accident. His initial single-screw syndesmotic fixation failed post-operatively, necessitating revision surgery with the addition of a second screw. This case highlights the clinical implications of underestimating syndesmotic injury severity and questions whether dual-screw fixation should be considered more routinely in chronic or high-risk cases.
A 25-year-old male with a history of left medial malleolar fracture, previously fixed with two screws in February 2025, presented to the Emergency Department 5 months later following a motorcycle accident that resulted in a new bimalleolar fracture of the left ankle. On examination, there was moderate swelling and a limited range of motion (ROM) of the left ankle. Distal neurovascular status was intact, and all compartments were soft. A superficial abrasion was noted over the medial aspect of the left foot. An X-ray of the left ankle revealed a bimalleolar fracture along with non-union of the medial malleolar fracture (Fig. 1).
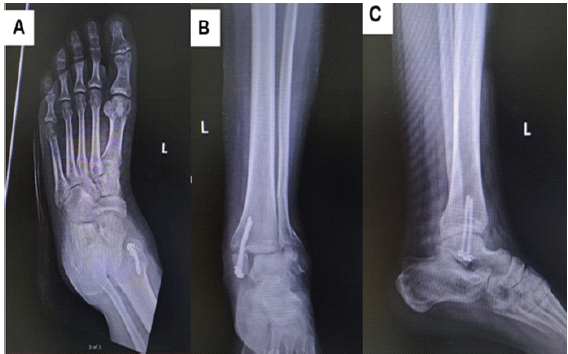
Figure 1: Pre-operative anteroposterior (a and b) and lateral (c) X-rays of the left ankle showing a bimalleolar fracture and bent medial malleolar screws with fracture non-union from previous fixation.
A CT scan showed evidence of a bimalleolar fracture of the left ankle and increased diastasis of the syndesmotic joint, seen using a side-to-side comparison of the tibiofibular clear space with the contralateral side (Fig. 2).
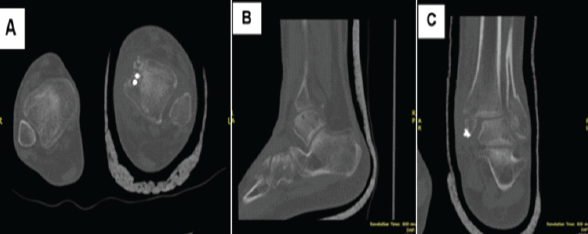
Figure 2: Preoperative axial (a), sagittal (b), and coronal (c) Computed tomography scans of the left ankle showing a bimalleolar ankle fracture and syndesmotic joint injury.
The patient was admitted under the orthopedic and trauma surgery team, kept nil per os, and started on analgesics and intravenous cefuroxime due to leukocytosis noted on complete blood count. A plan was made to perform surgical fixation the following day. The patient underwent open reduction and internal fixation the next day. Using a lateral ankle approach, the fibular fracture site was exposed, and callus from previous injury was debrided. Intraoperative findings suggest that the syndesmotic injury is chronic, with evident ligament fraying and fibrotic tissue consistent with longstanding instability. A disrupted syndesmosis with shortening of the distal fibula was confirmed. Reduction was performed and secured using a lateral plate with multiple screws, and a single 3.5 mm quadricortical syndesmotic screw was inserted under fluoroscopic guidance (Fig. 3).
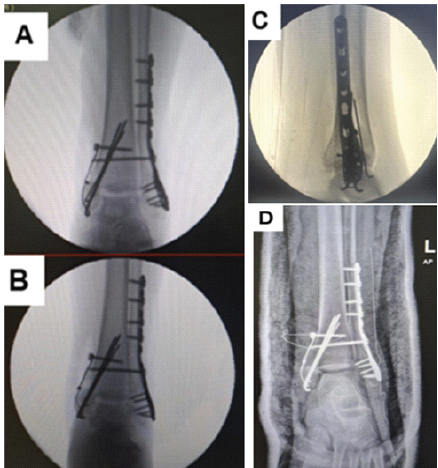
Figure 3: Fluoroscopic images showing initial single 4-cortex syndesmotic screw fixation following open reduction with internal fixation. Mortise (a), Anteroposterior (b), and Lateral (c) views. (d) Post-operative X-ray showing bimalleolar fixation with a single syndesmotic screw in situ.
Subsequently, through a medial ankle approach, the bent medial malleolar screws were removed. Debridement of fibrous tissue and periosteum from the fracture site was performed. Fixation was achieved using a tension band technique with additional K-wire stabilization. The surgical site was washed, wounds closed in layers, and a below-knee slab was applied post-operatively. However, follow-up imaging 1 week later demonstrated anterior subluxation of the syndesmosis (red arrow) (Fig. 4).
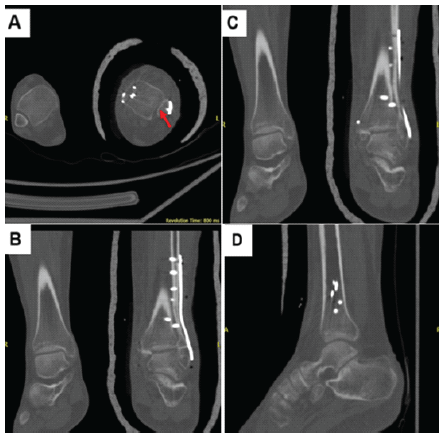
Figure 4: Follow-up computed tomography scan showing anterior subluxation (red arrow) of the syndesmosis. Axial (a), coronal (b and c), and sagittal (d) views.
As a result, the patient underwent revision surgery. Intraoperatively, the initial syndesmotic screw was found to be suboptimally positioned and was removed. Two new 3.5 mm syndesmotic screws were then placed.
Post-operative management included pain control, regular wound care, dressing changes every 72 h, a 5-day course of antibiotics due to compromised local tissue conditions around the ankle, and non-weight-bearing mobilization. A post-operative X-ray confirmed proper alignment of the ankle joint and internal fixation of the fibula and medial malleolus (Fig. 5). A CT scan revealed proper alignment of the syndesmotic joint (red arrow) (Fig. 6).
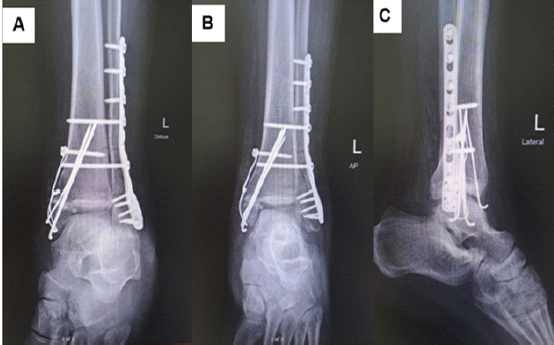
Figure 5: Post-operative oblique (a), anteroposterior (b), and lateral (c) X-rays showing dual syndesmotic screw fixation and confirming restored ankle joint.
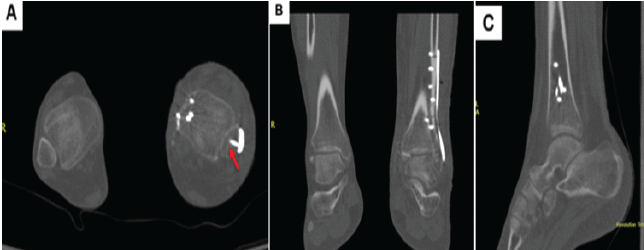
Figure 6: Computed tomography scan showing proper alignments of the fibular and medial malleolar fixations. Axial (a), coronal (b), and sagittal (c) views.
The patient was discharged with instructions for pain management, regular wound care, non-weight-bearing ambulation, and ankle elevation with intermittent cryotherapy. Full weight bearing was planned to be initiated in 8–12 weeks after surgery, with possible elective removal of the syndesmotic screws. Eight weeks post-operatively, the patient came in without walking difficulty with only mild swelling reported. Physical examination showed well-healed medial and lateral scars, soft compartments, and a full ROM of the left ankle joint. Subsequent follow-ups were carried out virtually, as the patient returned to his home country, and no pain or new complaints were reported.
A syndesmosis is a fibrous joint defined as the connection of two adjacent bones by ligaments or a tough membrane [4]. Syndesmotic injury occurs in approximately 10–20% of ankle fractures, with an increase in incidence in high-energy trauma and young athletic populations [1]. The syndesmosis naturally widens about 1 mm when moving from full plantarflexion to dorsiflexion, as the joint is naturally dynamic. However, due to an injury, it can widen up to 7.3 mm and externally rotate an additional 10.2° from baseline [6]. Assessment of the syndesmotic widening can be done using conventional weight-bearing radiographs, CT scans, or MRI. MRI or CT scans were suggested to be used in post-traumatic conditions as they are more sensitive for detecting minor degrees of syndesmotic injury [7]. Persistent syndesmotic injury should be evaluated using intraoperative 3-D imaging or post-operative CT scans, after reduction and syndesmotic screw fixation of unstable syndesmotic injuries [8]. The most widespread protocol for managing acute syndesmotic injuries without instability is the three-phase conservative approach. This includes rest, ice, and non-weight-bearing immobilization as the first phase, physiotherapy and walking with a functional brace in the second phase, and finally training of neuromuscular control and proprioception until full recovery in the third phase [2]. Surgical management for unstable syndesmotic injuries includes open/arthroscopic debridement and either static cortical screw fixation, dynamic fixation using suture-button devices, or ligament reconstruction [9]. Screw fixation is used primarily in subacute injuries (6 weeks–6 months) [2]. No consensus exists currently on the treatment of CSI, but evidence demonstrates favorable outcomes for the different types of management [9,10]. A meta-analysis comparing suture-button fixation with syndesmotic screw fixation in acute syndesmosis disruption reported that the suture-button technique resulted in improved joint function and a lower rate of implant failure compared with syndesmotic screws. This difference is related to the physiological motion of the syndesmosis, which can place mechanical stress on the screw, unlike the suture-button, which maintains adequate reduction and stability while allowing controlled micromotion [11]. This concept may be reflected in our case, where early post-operative joint subluxation occurred following initial fixation with a single syndesmotic screw, which highlights the mechanical stress placed on rigid fixation constructs. Interestingly, the combined usage of suture-button and syndesmotic screw has been proposed for highly physically demanding individuals, as it may provide enhanced protection of the syndesmosis while allowing quicker restoration of the biomechanical action of the ligament complex [9]. In the present case, the injury resulted from high-energy trauma and was associated with a complex ankle fracture pattern, factors that may increase mechanical stress across the syndesmotic complex. There are arguments surrounding screw fixation with regard to the number of screws, screw size, and the number of cortices engaged. In acute and otherwise healthy patients, studies have shown no significant difference in clinical outcomes, patient satisfaction, or complication rates between single and double screw fixation [3]. Nevertheless, several studies suggest that although a single 3.5 mm tricortical screw may provide satisfactory initial fixation, dual-screw constructs may offer greater biomechanical stability in situations where increased mechanical stress is anticipated [2,12]. Moreover, a retrospective study also reported that screws with a diameter of 3.5 mm were more prone to breakage than screws measuring 4–4.5 mm and therefore recommended to use two 4.5 mm quadricortical screws as they offer greater resistance than a single screw and are easier to remove than a 3.5 mm screw if screw failure occurs [2,13]. In our case, early post-operative syndesmotic subluxation was observed following initial fixation with a single 3.5-mm quadricortical syndesmotic screw. Intraoperative findings during revision revealed that the initial screw was suboptimally positioned, which may have contributed to the loss of reduction. However, the CSI resulted in persistent posterior instability, making stabilization with a single screw insufficient even if placed optimally; therefore, the revision with a dual-screw construct provided improved rotational and translational stability in this complex setting. The successful outcome of the revision procedure may reflect both improved screw positioning and the use of a stronger fixation construct. Other methods recommended for treating CSI include tibiofibular fusion, but this procedure should be reserved for patients with degenerative changes of the tibiofibular joint [14]. The majority of published studies on CSI describe a wide range of management techniques, with very few studies specifically examining the syndesmotic screw approach [14].
Multiple approaches with favorable outcomes have been suggested for the management of syndesmotic injuries. Despite this, little evidence exists on the gold-standard approach to the use of syndesmotic screw fixation in chronic injuries. In our report, we presented a case of a 25-year-old male who sustained a left ankle bimalleolar fracture along with CSI. The bimalleolar fractures were fixed using a plate laterally and a tension band, along with Kirschner-wire stabilization medially. The initial single-screw fixation of the syndesmosis resulted in anterior subluxation of the joint, based on CT findings, which necessitated revision surgery for a dual-screw fixation. Full ankle ROM was achieved in addition to satisfactory patient outcomes. The post-operative failure in our case highlights the need to carefully consider stronger fixation methods in selected patients with high-instability risk. While a single-screw may be sufficient in acute or low-risk cases, it may not provide the necessary support in high, physically demanding individuals or chronic injury cases that might need extra reinforcement, such as dual-screw fixation or the combined usage of suture-button along with the syndesmotic screw to provide better restoration of normal biomechanical function of the ligament complex.
This case highlights the critical importance of recognizing fixation failure in chronic syndesmotic injuries. It demonstrates that dual-screw fixation can restore stability where single-screw constructs fail, thus, highlighting a gap in current orthopedic guidelines and emphasizing the need to reconsider fixation protocols for high-demand or chronic cases to prevent recurrent instability and improve long-term outcomes.
References
- 1. Wang C, Ma X, Wang X, Huang J, Zhang C, Chen L. Internal fixation of distal tibiofibular syndesmotic injuries: A systematic review with meta-analysis. Int Orthop 2013;37:1755-63. [Google Scholar] [PubMed]
- 2. De-Las-Heras Romero J, Alvarez AM, Sanchez FM, Garcia AP, Porcel PA, Sarabia RV, et al. Management of syndesmotic injuries of the ankle. EFORT Open Rev 2017;2:403-9. [Google Scholar] [PubMed]
- 3. Peek AC, Fitzgerald CE, Charalambides C. Syndesmosis screws: How many, what diameter, where and should they be removed? A literature review. Injury 2014;45:1262-7. [Google Scholar] [PubMed]
- 4. Hermans JJ, Beumer A, De Jong TA, Kleinrensink G. Anatomy of the distal tibiofibular syndesmosis in adults: A pictorial essay with a multimodality approach. J Anat 2010;217:633-45. [Google Scholar] [PubMed]
- 5. Van Dijk CN, Longo UG, Loppini M, Florio P, Maltese L, Ciuffreda M, et al. Classification and diagnosis of acute isolated syndesmotic injuries: ESSKA-AFAS consensus and guidelines. Knee Surg Sports Traumatol Arthrosc 2016;24:1200-16. [Google Scholar] [PubMed]
- 6. Hogan MV, Boakye L, James NA, Brown CL, Yan AA. Syndesmosis injury. Oper Tech Sports Med 2021;29:150872. [Google Scholar] [PubMed]
- 7. Chen Y, Qiang M, Zhang K, Li H, Dai H. A reliable radiographic measurement for evaluation of normal distal tibiofibular syndesmosis: A multi‐detector computed tomography study in adults. J Foot Ankle Res 2015;8:32. [Google Scholar] [PubMed]
- 8. Franke J, Von Recum J, Suda AJ, Vetter S, Grützner PA, Wendl K. Predictors of a persistent dislocation after reduction of syndesmotic injuries detected with intraoperative three-dimensional imaging. Foot Ankle Int 2014;35:1323-8. [Google Scholar] [PubMed]
- 9. Gomaa AR, Mason L. Chronic syndesmotic instability – current evidence on management. J Clin Orthop Trauma 2024;50:102382. [Google Scholar] [PubMed]
- 10. Mahmoud E, Nabian MH. Chronic injury of distal tibiofibular syndesmosis with ankle fracture dislocation: A case report. J Orthop Spine Trauma 2020;6:16-25. [Google Scholar] [PubMed]
- 11. Shimozono Y, Hurley ET, Myerson CL, Murawski CD, Kennedy JG. Suture button versus syndesmotic screw for syndesmosis injuries: A meta-analysis of randomized controlled trials. Am J Sports Med 2019;47:2764-71. [Google Scholar] [PubMed]
- 12. Vohra R, Singh A, Thorat B, Patel D. Instability of the distal tibiofibular syndesmosis. J Orthop Surg (Hong Kong) 2023;31:10225536231182349. [Google Scholar] [PubMed]
- 13. Stuart K, Panchbhavi VK. The fate of syndesmotic screws. Foot Ankle Int 2011;32:S519-25. [Google Scholar] [PubMed]
- 14. Krähenbühl N, Weinberg MW, Hintermann B, Haller JM, Saltzman CL, Barg A. Surgical outcome in chronic syndesmotic injury: A systematic literature review. Foot Ankle Surg 2019;25:691-7. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report
June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report