
Primary total hip arthroplasty with a long distal-loading stem is an effective single-stage solution for managing subtrochanteric femur fractures associated with advanced inflammatory hip arthritis.
Dr. K Praveen, Department of Orthopaedics, Vinayaka Mission’s Kirupananda Variyar Medical College and Hospital, Vinayaka Mission’s Research Foundation (Deemed to be University), Salem, Tamil Nadu, India. E-mail: kppraveenkumar1998@gmail.com
Abstract
Introduction: Subtrochanteric femur fractures associated with advanced hip arthritis present a complex surgical challenge, particularly in young patients with inflammatory arthropathies.
Case Report: We report a case of a 38-year-old male with bilateral psoriatic hip arthritis (Ficat and Arlet grade IV) who sustained a right-sided subtrochanteric femur fracture following a slip and fall. Given the coexistence of severe hip arthritis, femoral head collapse, and fracture morphology, a single-stage total hip arthroplasty (THA) using a long distal-loading monoblock stem was performed. The procedure successfully addressed both the fracture and arthritic pathology, allowing stable fixation and early functional recovery.
Conclusion: This case highlights the role of primary THA with a distal-loading stem as an effective treatment option in selected patients with subtrochanteric fractures and advanced inflammatory hip disease.
Keywords: Subtrochanteric femur fracture, psoriatic arthritism, total hip arthroplasty, distal-loading stem, case report.
Subtrochanteric femur fractures are biomechanically challenging injuries due to elevated cortical bone density and substantial muscle forces exerted at the fracture location [1]. The therapy of fractures gets more intricate when they occur alongside severe hip arthritis, particularly inflammatory types such as psoriatic arthritis. A subtrochanteric femoral fracture associated with pre-existing ipsilateral hip osteoarthritis (OA/STF) is uncommon [2]. Intramedullary nailing is generally the chosen treatment for subtrochanteric femur fractures. Arthritic abnormalities, including medial migration of the head and neck shortening, hinder the accurate positioning of the entry point and the implantation of the nail along the long axis of the femur [3]. The entry point is frequently positioned excessively laterally while utilizing a fracture table equipped with a perineal post. The fracture is corrected in varus malalignment, which must be avoided to prevent non-union. Traditional osteosynthesis may inadequately alleviate debilitating arthritic pain and anatomical deformities [4]. In such scenarios, primary total hip arthroplasty (THA) with a long stem offers a single-stage solution by treating both the fracture and the arthritic joint.
A 38-year-old male, a known case of bilateral psoriatic hip arthritis, presented to the emergency department following a slip and fall, with complaints of pain over the right hip and thigh. Clinical examination revealed tenderness over the right hip and proximal thigh, an externally rotated right lower limb, and widespread hyperpigmented healing psoriatic skin lesions. The patient had a history of cortisol insufficiency, managed in coordination with a general physician and dermatologist. He had undergone left THA 3 months earlier for advanced psoriatic arthritis. Radiographs of the pelvis demonstrated bilateral hip arthritis with femoral head collapse and acetabular sclerosis, consistent with Ficat and Arlet grade IV disease. Right hip radiographs revealed a transverse subtrochanteric femur fracture extending from the calcar to the lateral wall, along with severe arthritic changes of the hip joint. Multiple treatment strategies were considered, including isolated osteosynthesis, staged fracture fixation followed by delayed THA, and combined osteosynthesis with primary THA. Given the advanced arthritis, femoral head collapse, and fracture configuration, isolated fixation was deemed insufficient and technically challenging. A single-stage THA using a distal-loading long stem was planned to simultaneously manage the fracture and the arthritic hip (Figs. 1, 2, 3).

Figure 1: Clinical picture showing hyperpigmented healing psoriatic skin lesions.
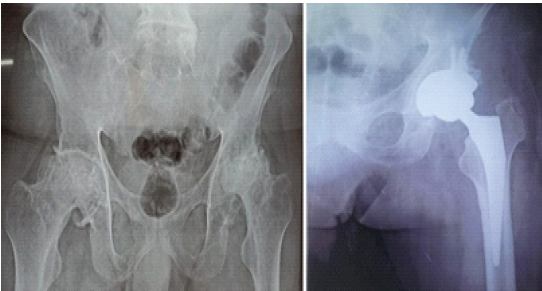
Figure 2: Radiographs of the pelvis demonstrated bilateral hip arthritis with femoral head collapse and acetabular sclerosis, with left total hip arthroplasty done.
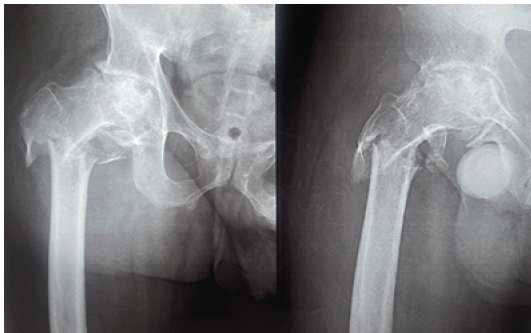
Figure 3: Right hip radiographs revealed a transverse subtrochanteric femur fracture with severe arthritic changes of the hip joint.
Surgical technique
After obtaining informed written consent, the patient was positioned laterally and operated under combined spinal-epidural anesthesia. A standard Hardinge (direct lateral) approach was used. The hip was dislocated, and a femoral neck osteotomy was performed. Acetabular preparation was completed, and the cup was implanted with approximately 37° of inclination and 15° of anteversion.
The lateral approach was extended distally through the vastus lateralis to expose the fracture. The distal fragment was controlled using bone clamps. Sequential proximal canal preparation was done based on the distal bone canal. A monoblock distal-loading fluted titanium stem (Pitkar) was implanted to achieve distal scratch-fit fixation. The proximal fragment was adequately stabilized by the stem itself, and no additional plate or cerclage fixation was required. The total operative time was 90 min, and the total blood loss was 200 mL (Fig. 4).
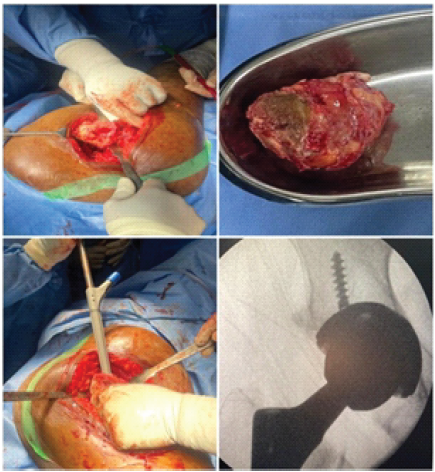
Figure 4: Intraoperative pictures.
Outcome and follow-up
Post-operative radiographs demonstrated satisfactory alignment of the subtrochanteric fracture and appropriate positioning of the prosthetic components. The patient had stable fixation and satisfactory early clinical recovery. Early mobilization was initiated as per standard post-operative protocol (Fig. 5). During 1st post-operative month patient had a Harris hip score of 83.8 was achieved. Patient improved functionally during the follow-up period. (Fig. 6) The 8th month follow-up X-ray demonstrated B/L implant in situ without any aseptic loosening. During 8th post-operative month patient had a Harris hip score of 91 was achieved (Fig. 7).
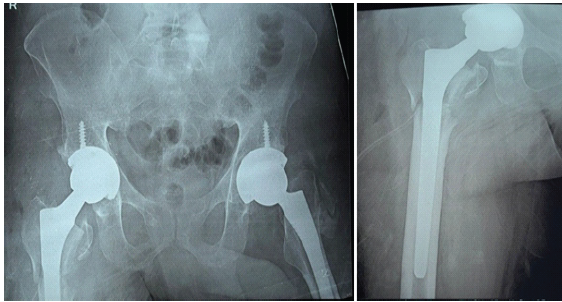
Figure 5: Post-operative radiographs demonstrated satisfactory alignment of the subtrochanteric fracture and appropriate positioning of the prosthetic components
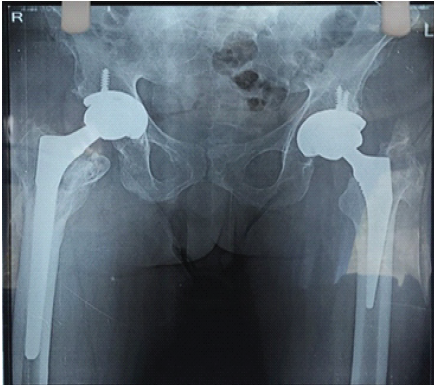
Figure 6: 3-month follow-up X-ray and bilateral hip range of motion pictures.
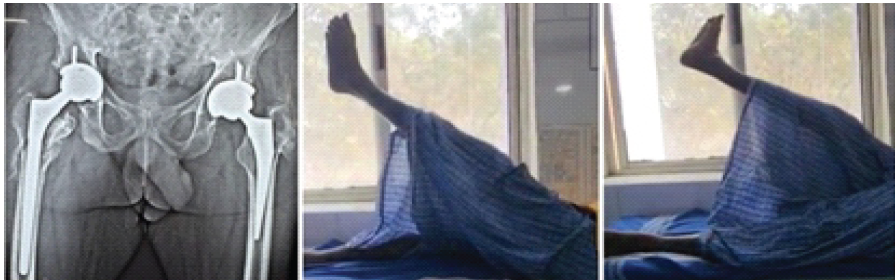
Figure 7: 9th month follow-up X-ray.
Subtrochanteric femur fractures are biomechanically challenging injuries because of high cortical bone content, limited vascularity, and strong deforming muscular forces acting on the proximal fragment [1,2]. The management becomes substantially more complex when such fractures coexist with advanced ipsilateral hip arthritis, particularly inflammatory arthritis such as psoriatic arthritis. This rare combination poses difficulties in fracture reduction, implant selection, and restoration of hip biomechanics, with no universally accepted treatment algorithm [3]. Conventionally, isolated osteosynthesis using intramedullary nailing is considered the treatment of choice for subtrochanteric fractures [4]. However, the presence of advanced hip arthritis significantly limits the effectiveness of this approach. Arthritic deformities such as femoral head collapse, acetabular sclerosis, neck shortening, and altered femoral version make correct entry point identification and nail insertion difficult, increasing the risk of varus malreduction, delayed union, or non-union [5,6]. Furthermore, osteosynthesis alone fails to address the underlying arthritic pain and functional disability, often necessitating a second major reconstructive procedure. Similar technical concerns with intramedullary nailing in arthritic hips have been emphasized in previous reports, where distorted proximal femoral anatomy predisposed to malalignment and compromised outcomes [7]. THA has been increasingly recognized as a viable option in selected patients with subtrochanteric fractures associated with severe hip arthritis [8]. Although arthroplasty is often avoided in younger patients due to concerns regarding implant longevity and revision risk, its role becomes justified when arthritis is advanced (Ficat and Arlet grade IV), symptomatic, and associated with femoral head collapse [9]. In such scenarios, arthroplasty addresses both the fracture and joint pathology in a single stage, facilitating early mobilization and improved functional recovery. Recent case reports and small series have demonstrated favorable outcomes using long-stem THA in similar fracture–arthritis combinations, supporting this treatment strategy [10,11,12]. The potential benefits of a single-stage procedure versus staged surgeries in terms of hospitalization, rehabilitation, and overall resource utilization were explained, and the patient opted for the single-stage approach that we proposed. Implant selection plays a pivotal role in achieving successful outcomes. Distal-loading long stems bypass the fracture site, achieve fixation in intact diaphyseal bone, and provide axial and rotational stability independent of proximal bone quality [13]. Monoblock fluted tapered titanium stems achieve reliable distal scratch-fit fixation and are particularly advantageous when proximal metaphyseal support is compromised. In the present case, the proximal fragment was intact and could be adequately stabilized by the stem itself, eliminating the need for supplementary plate or cerclage fixation. This approach minimized additional soft-tissue dissection and implant-related complications while maintaining stable fracture fixation [11,13]. It is well recognized that THA performed in fracture or post-traumatic settings carries higher complication rates than primary THA for degenerative osteoarthritis. Hung et al. reported that salvage THA following failed fixation or post-traumatic arthritis was associated with longer operative time, greater blood loss, delayed ambulation, and significantly higher rates of early dislocation, reoperation, and revision compared to primary THA [14]. These findings underscore the importance of meticulous surgical technique, accurate restoration of limb length and offset, appropriate component positioning, and careful soft-tissue balancing when performing THA in the setting of fractures. Inflammatory arthropathies such as psoriatic arthritis add another layer of complexity due to poor bone quality, altered biomechanics, and associated systemic comorbidities, including long-term steroid use and immunosuppression, which may increase the risk of infection and impaired wound healing [15]. Despite these challenges, addressing both the fracture and arthritic pathology in a single-stage procedure reduces the morbidity associated with staged surgeries and allows earlier functional rehabilitation. In the present case, primary THA using a distal-loading monoblock fluted stem provided stable fixation of the subtrochanteric fracture while simultaneously addressing advanced psoriatic hip arthritis. The early clinical and radiological outcomes were satisfactory, supporting the concept that treatment should be individualized based on fracture pattern, severity of arthritis, bone quality, and patient functional demands rather than chronological age alone [8,14]. Management of subtrochanteric fractures with advanced hip arthritis includes isolated osteosynthesis, staged fixation followed by delayed THA, and single-stage arthroplasty with or without supplementary fixation. Isolated osteosynthesis, typically with intramedullary nailing, is biomechanically sound for fractures but may be technically difficult in arthritic hips due to distorted proximal anatomy and does not relieve underlying arthritic pain, often necessitating later conversion to THA. A staged approach allows fracture union before arthroplasty but requires two major procedures, increasing morbidity, cost, and technical complexity during subsequent implant removal and reconstruction. In contrast, single-stage arthroplasty with a long distally fixed stem addresses both fracture and joint pathology simultaneously, provides stable fixation by bypassing the fracture site, and facilitates early mobilization, though it demands careful patient selection and meticulous surgical technique [3,10,12,14]. Limitations include a single case report and inherently limited in generalizability in our case report. We acknowledge that the decision to perform primary THA was based on individualized clinical judgment, and the rationale for choosing arthroplasty despite the patient’s age has been clarified based on advanced Grade IV disease and femoral head collapse. We also acknowledge that this represents a rare clinical presentation. This has been clearly stated in the revised manuscript, emphasizing that while the report provides insight into a possible management strategy, it does not establish standardized treatment guidelines.
Primary THA using a long distal-loading stem can be an effective single-stage solution for subtrochanteric femur fractures associated with advanced inflammatory hip arthritis. Careful patient selection, appropriate implant choice, and meticulous surgical technique are essential to achieve stable fixation and favorable outcomes.
In selected patients with severe hip arthritis and concomitant subtrochanteric fractures, especially those with inflammatory arthropathies, primary long-stem THA can simultaneously restore stability, relieve pain, and enable early mobilization when meticulous technique and appropriate implant selection are employed.
References
- 1. Bedi A, Toan Le T. Subtrochanteric femur fractures. Orthop Clin North Am 2004;35:473-83. [Google Scholar] [PubMed]
- 2. Russell TA, Taylor JC. Subtrochanteric fractures of the femur. Instr Course Lect 2008;57:345-54. [Google Scholar] [PubMed]
- 3. Koval KJ. Subtrochanteric femur fracture below an arthritic hip: Opinion: Open reduction and internal fixation. J Orthop Trauma 2005;19:61-2. [Google Scholar] [PubMed]
- 4. Haidukewych GJ, Berry DJ. Nonunion of fractures of the subtrochanteric region of the femur. Clin Orthop Relat Res 2004;419:185-8. [Google Scholar] [PubMed]
- 5. Banaszkiewicz PA. Subtrochanteric fractures of the femur. In: Campbell’s Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021. p. 3103-25. [Google Scholar] [PubMed]
- 6. Lo YC, Su YP, Hsieh CP, Huang CH. Augmentation plate fixation for treating subtrochanteric fracture nonunion. Indian J Orthop 2019;53:246-50. [Google Scholar] [PubMed]
- 7. Iga T, Kato K, Karita T. Subtrochanteric fracture of the femur accompanying pre-existing ipsilateral osteoarthritis of the hip successfully treated with intramedullary nailing in the lateral decubitus position: A case report. Cureus 2018;10:e3081. [Google Scholar] [PubMed]
- 8. Koval KJ, Zuckerman JD. Hip fractures: I. Overview and evaluation and treatment of femoral-neck fractures. J Am Acad Orthop Surg 1994;2:141-9. [Google Scholar] [PubMed]
- 9. Azar FM, Beaty JH, Canale ST. Campbell’s Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021. [Google Scholar] [PubMed]
- 10. Tsakotos G, Stathopoulos IP, Papakostidis C, Giannoudis PV. Management of subtrochanteric femoral fractures associated with hip arthritis: A review. Injury 2019;50 Suppl 2:S47-54. [Google Scholar] [PubMed]
- 11. Faisal M, Kukde PN, Atilkar AJ, Maurya VO. Subtrochanteric femur fracture with pre-existing ipsilateral hip arthritis treated with long stem total hip arthroplasty: A case report. Int J Res Orthop 2025;11:939-41. [Google Scholar] [PubMed]
- 12. Deleanu B, Prejbeanu R, Vermesan D, Haragus H, Florea B. Combined femoral head osteonecrosis and subtrochanteric fracture treated with total hip arthroplasty. Orthop Traumatol Surg Res 2016;102:523-6. [Google Scholar] [PubMed]
- 13. Wagner M. Revision prosthesis for the hip joint in severe bone loss. Orthopade 1987;16:295-300. [Google Scholar] [PubMed]
- 14. Hung CC, Chen KH, Chang CW, Chen YC, Tai TW. Salvage total hip arthroplasty after failed internal fixation for proximal femur and acetabular fractures. J Orthop Surg Res 2023;18:45. [Google Scholar] [PubMed]
- 15. Gladman DD, Chandran V. Observations on the natural history of psoriatic arthritis. Rheum Dis Clin North Am 2015;41:581-97. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report
June 1, 2026 Lateral Femoral Cutaneous Nerve Neuroma Resection and Nerve Capping after Direct Anterior Approach: A Case Report July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures