
Chronic patellar tendon ruptures require complex surgical reconstruction, and good functional outcomes depend on stable repair combined with structured rehabilitation.
Dr. Malick Diop, Dalal Jamm Hospital, Guediawaye, Senegal. E-mail: malickfatydiop@gmail.com
Abstract
Introduction: Neglected patellar tendon ruptures are uncommon injuries that result in disruption of the knee extensor mechanism. Their diagnosis is often challenging, and their management remains technically demanding, frequently necessitating advanced reconstructive procedures.
Case Report: We report three cases of neglected patellar tendon ruptures in patients over 40 years of age. Diagnosis was based on clinical examination and imaging findings . All patients underwent surgical repair of the tendon reinforced with a protective steel wire frame. Postoperatively, immobilization was achieved with a knee brace or removable orthosis, followed by structured rehabilitation. At final follow-up, all patients had regained active knee extension.
Conclusion: Chronic ruptures of the patellar tendon, more commonly encountered in low-resource settings, remain a challenging condition. Surgical intervention continues to represent the cornerstone of their management.
Keywords: Patellar tendon, neglected rupture, knee extensor mechanism.
Neglected ruptures of the patellar tendon are rare injuries of the knee extensor apparatus [1]. They usually occur in young individuals [2] and are highly disabling. These lesions represent both a diagnostic and therapeutic challenge. Management is difficult and essentially surgical, while rehabilitation plays a major role in functional recovery. We report three cases of neglected patellar tendon ruptures. All were treated by tendon repair reinforced with a protective frame, with favorable outcomes marked by the recovery of active knee extension.
Case 1
Mr. , a 43-year-old man with no medical history, presented 2 months after a domestic accident with an old injury to the left knee. He had slipped on the stairs and initially consulted a traditional healer. Examination revealed loss of active knee extension and a palpable gap along the patellar tendon. The overlying skin was intact. Radiographs of the left knee (anteroposterior and lateral views) showed patella alta with a Caton-Deschamps index of 1.9 (Fig. 1). Ultrasound confirmed rupture of the patellar tendon.

Figure 1: Standard radiographs of the left knee showing patella alta (Patient 1).
Surgery was performed under spinal anesthesia with the patient supine. A medial parapatellar approach revealed rupture of the tendon 1 cm distal to the patellar insertion with frayed edges. Tendon repair was performed and reinforced with a protective steel wire frame (Fig. 2).
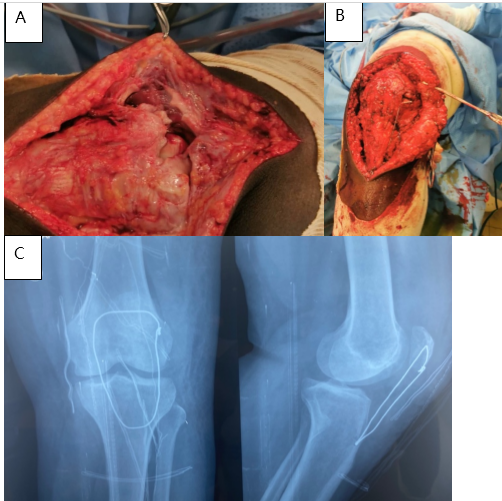
Figure 2: Intraoperative view of the patellar tendon rupture (a), tendon repair (b), and post-operative control radiograph (c) – Patient 1.
Rehabilitation was initiated 6 weeks postoperatively. At 8-month follow-up, the patient had regained full active knee extension.
Case 2
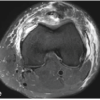
Mrs. , a 50-year-old woman with no significant medical history, presented 45 days after a closed injury of the left knee caused by a fall. Initial management had been performed in a non-specialized center. On examination, she walked with a limp. There was loss of active knee extension and a palpable defect along the patellar tendon, with intact skin. Standard radiographs revealed patella alta with a Caton-Deschamps index of 2 (Fig. 3). Magnetic resonance imaging (MRI) confirmed rupture of the patellar tendon (Fig. 3). Surgery was performed under spinal anesthesia with the patient supine. Intraoperative findings revealed a midsubstance rupture of the tendon. Tendon repair was performed and reinforced with a protective frame (Fig. 4). At 12-month follow-up, the patient had recovered active knee extension.
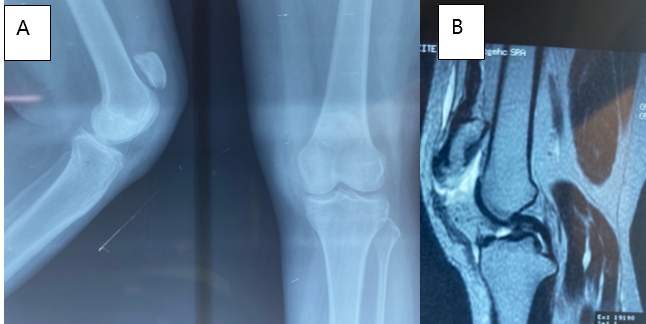
Figure 3: Standard radiograph (A) showing patella alta, and magnetic resonance imaging of the left knee (B) confirming patellar tendon rupture – Patient 2.
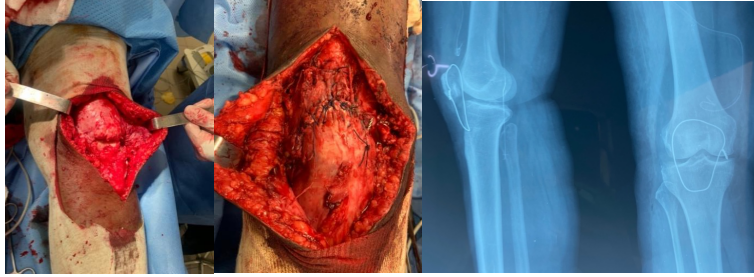
Figure 4: Intraoperative view of the rupture (a), tendon repair with protective frame (b), and post-operative control radiograph (c) – Patient 2.
Case 3
Mr. , a 43-year-old man, presented 1 year after a sports-related injury to the left knee. He had initially been treated surgically in another hospital, where a diagnosis of patellar tendon rupture had been made. He consulted us due to persistent symptoms. Examination revealed quadriceps atrophy, loss of active knee extension, and a high-riding patella palpable in the supracondylar region. Radiographs confirmed patella alta and the presence of a protective steel wire from previous surgery (Fig. 5).
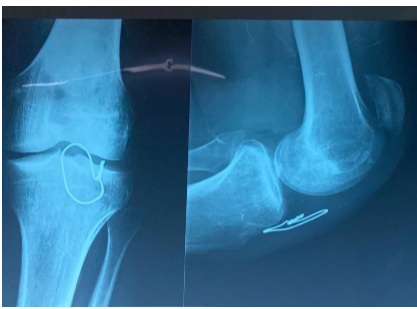
Figure 5: Standard radiograph of the left knee showing patella alta with cerclage wire in place – Patient 3.
Surgery was performed under spinal anesthesia. Intraoperative findings revealed a proximal rupture of the patellar tendon with quadriceps retraction. Repair required a V-Y lengthening of the quadriceps tendon, reinforced by a protective steel wire frame (Fig. 6). At 3-month follow-up, the patient had regained active knee extension, though quadriceps atrophy persisted. Radiographs showed the patella in an anatomical position over the femoral trochlea.
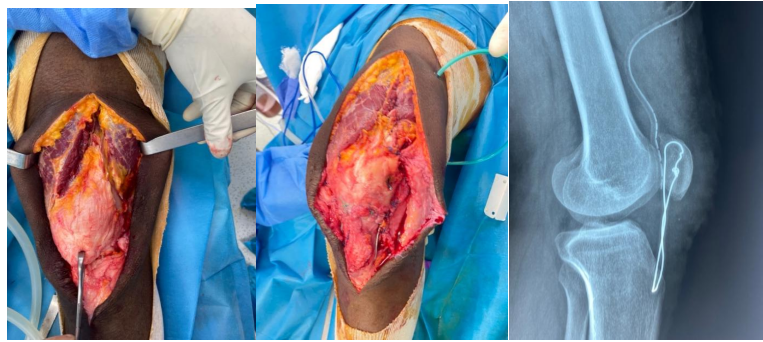
Figure 6: Intraoperative view of the rupture and tendon repair with V-Y quadriceps lengthening and protective cerclage wiring – Patient 3.
Patellar tendon ruptures are rare, particularly in their neglected forms. Most authors report isolated cases [1,3]. These lesions are highly disabling because they interrupt the continuity of the knee extensor mechanism [4,5]. The typical mechanism is a violent eccentric contraction of the quadriceps on a flexed knee, reversing the force ratio between the quadriceps and patellar tendons (such as during landing from a jump, stumbling, or rising from a squat) [6,7]. The injury may also result from a sudden contraction opposed by forced knee flexion beyond 90°. Alternatively, direct trauma to the flexed knee during road traffic accidents [2] or impact to the infrapatellar region at 90° flexion [3] may be responsible. In developing countries, delayed diagnosis is often due to consultation with traditional healers. In our series, only one patient was initially evaluated in a specialized center, while the others were seen by non-specialists or traditional practitioners. Diagnosis is based on clinical findings: loss of active knee extension, a palpable gap along the tendon, and patella alta. In some neglected cases, limited active extension may persist due to continuity of the retinacula [3,6]. In chronic presentations [8,9], clinical diagnosis may be more difficult, as signs are less obvious, making imaging essential. Standard radiographs typically reveal patella alta with a Caton-Deschamps index above 1.2. MRI further confirms the diagnosis, but should not delay surgical management, which remains the only effective treatment. Surgical repair of neglected ruptures is challenging due to quadriceps retraction and proximal patellar displacement. To address these issues, some authors recommend preoperative methods such as transpatellar traction, external fixation, or even release of the rectus femoris tendon through a Hueter approach to progressively reposition the patella before repair [7]. Various surgical techniques have been described depending on chronicity and tissue quality. Most authors perform end-to-end tendon repair reinforced with augmentation techniques, with or without protective wiring or prosthetic material such as polydioxanone sutures. Others have used tendon grafts to reinforce reconstruction [5,10]. In our series, two patients underwent direct end-to-end repair, while one required a V-Y quadriceps lengthening to achieve tension-free suturing. In all cases, the repair was protected by a steel wire frame. Post-operative immobilization with a knee brace or removable orthosis was applied in all patients. Rehabilitation is a cornerstone of treatment. Early quadriceps isometric contractions are encouraged to prevent stiffness. In our patients, all achieved satisfactory functional outcomes with restoration of active knee extension and no residual flexion contracture. These favorable results may be attributed to solid tendon repair, protection with cerclage wiring, and early, structured rehabilitation.
Neglected ruptures of the patellar tendon are rare but functionally disabling injuries characterized by loss of active knee extension. Their management is difficult and relies on surgical repair, often requiring reinforcement techniques. Rehabilitation is essential to achieve satisfactory functional recovery.
Neglected ruptures of the knee extensor mechanism are very rare. Functional recovery relies on optimal surgical management, while rehabilitation remains a crucial step in follow-up.
References
- 1. Boutayeb F, Amar MF, Elibrahimi A, Chraibi F, Ameziane L. Neglected iatrogenic rupture of the patellar tendon: A case report. J Traumatol Sport 2007; 2:50-52. [Google Scholar] [PubMed]
- 2. Boggione C, Marmorat JL. Treatment of complete patellar tendon ruptures. J Traumatol Sport 2004; 21:204-217. [Google Scholar] [PubMed]
- 3. Chagar B, Boussouga M, Lazrak KH, Taobane H. Neglected spontaneous bilateral rupture of the patellar tendon: A case report. Rev Chir Orthop Reparatrice Appar Mot 2003; 89:733-737. [Google Scholar] [PubMed]
- 4. Azagui Y, Haddoun AR, Belmoubarek A, Andaloussi YE, Ouarab M. Reconstruction of an old quadriceps tendon rupture using semitendinosus gracilis graft: A case report. Rev Maroc Chir Orthop Traumato 2014; 55:39-43. [Google Scholar] [PubMed]
- 5. Dejour H, Denjean S, Neyret P. Treatment of old or recurrent ruptures of the patellar ligament by contralateral autograft. Rev Chir Orthop Reparatrice Appar Mot 1992; 78:58-62. [Google Scholar] [PubMed]
- 6. Kelly DW, Carter VS, Jobe FW, Kerlan RK. Patellar and quadriceps tendon ruptures–jumper’s knee. Am J Sports Med 1984; 12:375-380. [Google Scholar] [PubMed]
- 7. Zaidane A, Haddoun AR, Elandaloussi Y, Bennani FR, Azagui Y, Aziz A et al. Management of neglected patellar tendon ruptures: Report of two cases. J Traumatol Sport 2010; 27:189-194. [Google Scholar] [PubMed]
- 8. Buquet P, Piétu G, Huguet D, Capelli M, Bresson C and Letenneur J. Patellar tendon rupture: Report of 17 cases. Ann Orthop Ouest 1999; 31:45-50. [Google Scholar] [PubMed]
- 9. Ecker ML, Lotke PA, Glazer RM. Late reconstruction of the patellar tendon. J Bone Joint Surg Am 1976; 61:884-886. [Google Scholar] [PubMed]
- 10. Williams S, Ireland J, El Zebdeh MY. Late reconstruction of the patellar tendon: Two case reports. Knee 1999; 4:113-115. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Bilateral Patellar Tendon and Unilateral Syndesmotic Injury in a Recreational Athlete
July 1, 2026 Bilateral Patellar Tendon and Unilateral Syndesmotic Injury in a Recreational Athlete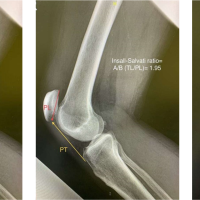 May 10, 2024 Knotless Anchor with FiberTape® for Fixing Pure Distal Patellar Tendon Rupture. A Case Report
May 10, 2024 Knotless Anchor with FiberTape® for Fixing Pure Distal Patellar Tendon Rupture. A Case Report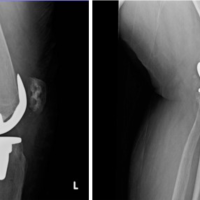 December 10, 2022 A Unique Patellar Tendon Rupture and Small Tibial Avulsion fracture in a Post-Menopausal Patient
December 10, 2022 A Unique Patellar Tendon Rupture and Small Tibial Avulsion fracture in a Post-Menopausal Patient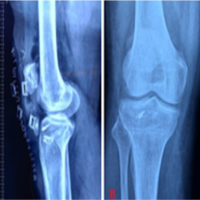 November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report
November 10, 2022 Management of Neglected Patellar Tendon Rupture by Peroneus Longus Autograft and Suture Anchor: A Case Report