
Os subtibiale, though a rare accessory ossicle, can mimic a medial malleolus fracture in acute ankle injuries, making careful clinical and radiological evaluation essential for accurate diagnosis. While most cases respond to conservative treatment, surgical excision provides excellent outcomes in patients with persistent symptoms affecting daily activities.
Dr. Akshant Chandel, Department of Orthopaedics, All India Institute of Medical Sciences, Marudhar Industrial Area, 2nd Phase, M.I.A. 1st Phase, Basni, Jodhpur - 342 005, Rajasthan, India. Email: akshant.akshant.chandel@gmail.com
Abstract
Introduction: Accessory ossicles of the ankle and foot are normal anatomical variants that are usually asymptomatic. The os subtibiale is a rare accessory ossicle located just inferior to the medial malleolus, with a reported prevalence of 0.9–1.2% in the general population. When symptomatic, it can mimic fractures or fracture non-union, leading to diagnostic confusion. Accurate diagnosis relies on careful clinical evaluation and appropriate imaging.
Case Report: A 20-year-old male presented with persistent pain around the right ankle, 7 months after sustaining a twisting injury while walking. He was initially treated by a local bonesetter and presented late to our facility with unresolved symptoms. Clinical and radiological evaluation initially suggested a medial malleolus fracture non-union. However, further imaging revealed a well-corticated, smooth-margined bone fragment inferior to the medial malleolus, consistent with a symptomatic os subtibiale. The patient underwent open excision of the ossicle under spinal anesthesia. Intraoperative findings confirmed the diagnosis. Postoperatively, ankle range of motion and weight-bearing were initiated as tolerated. At the 1-year follow-up, the patient was pain-free and had regained full ankle function.
Conclusion: This case highlights the importance of differentiating between a medial malleolus fracture non-union and a symptomatic os subtibiale, particularly in patients presenting late after ankle trauma. Awareness of this rare entity and its imaging characteristics is crucial to avoid misdiagnosis and ensure appropriate management, leading to excellent clinical outcomes.
Keywords: Os subtibiale, accessory ossicle, medial ankle pain, medial malleolus fracture non-union.
Accessory ossicles of the ankle and foot are normal variations in bone formation. They generally arise from accessory ossification centers adjacent to the main bone [1]. Most accessory ossicles in the ankle and foot are asymptomatic; however, following trauma or overuse, they may develop painful syndromes or degenerative changes. Furthermore, they can sustain or mimic fractures, potentially limiting ankle range of motion [2,3,4]. The os subtibiale is an uncommon accessory bone located just below the medial malleolus, affecting only 0.9–1.2% of individuals [5,6]. This rare anatomical variant may be mistakenly diagnosed and treated as a medial malleolus fracture when symptomatic. In this report, we present the case of a young male patient with a symptomatic os subtibiale who was initially treated by a local bonesetter and presented late to our hospital with persistent ankle pain. The condition was initially confused with a medial malleolus fracture non-union and was ultimately managed with open surgical excision of the ossicle.
A 20-year-old male presented to the outpatient department of our tertiary care center with a 7-month history of persistent pain around his right ankle following a twisting injury sustained while walking. He reported difficulty bearing weight on the affected limb immediately after the injury and was able to walk only with significant discomfort. At the time of injury, he sought treatment from a local bonesetter, who performed ankle manipulation and applied a crepe bandage, which was kept in place for approximately 1 month. Although the swelling gradually subsided, the patient continued to experience mild-to-moderate ankle pain. He did not seek hospital-based care at the time of injury; therefore, no initial radiographs were available for review. On examination, there was mild swelling on the medial aspect of the ankle, with no tenderness over the medial malleolus. A palpable, hard mass was noted just distal to the medial malleolus, which was tender and immobile. Ankle movements were painful. Plain radiographs revealed a small, oval-shaped bone fragment with rounded, smooth margins, completely separated from the tibia and located distal to the medial malleolus (Fig. 1).

Figure 1: Anteroposterior and mortise view of X-rays showing a small ossicle with rounded, smooth margins and completely separate from tibia.
Considering the regular, smooth, and non-sclerotic margins, an os subtibiale was regarded as the more likely diagnosis. However, a non-union fracture could not be ruled out, given the history of improper management of a previous ankle injury and persistent pain symptoms not typically associated with accessory ossicles.
A computed tomography scan was subsequently performed, which demonstrated smooth, corticated edges on both sides of the radiolucent cleft, with a well-formed medial malleolus and no evidence of sclerotic margins (Fig. 2).
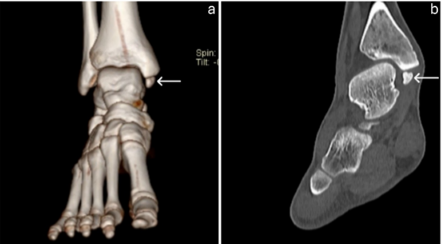
Figure 2: 3D and coronal view of computed tomography scan of the ankle showing ossicle with smooth, corticated edges.
These findings confirmed that it was not a fracture non-union. Based on these imaging findings and a review of the literature, a provisional diagnosis of os subtibiale was made.
Despite establishing this diagnosis, the cause of the patient’s pain remained unclear. After a detailed discussion, a magnetic resonance imaging (MRI) was obtained to evaluate the surrounding soft tissues for a potential source of pain. The MRI revealed bone marrow edema within the ossicle and impingement on the deltoid ligament (Fig. 3), which was considered the likely cause of the patient’s symptoms. The medial malleolus appeared well formed, and there was no cartilage continuity with the bone fragment, further confirming the diagnosis of an accessory ossicle.
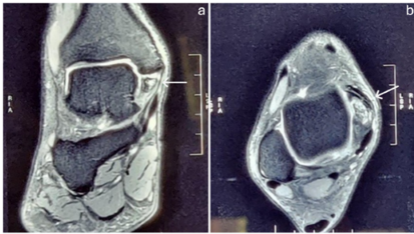
Figure 3: Coronal and axial view of T2-weighted magnetic resonance imaging image of the ankle showing edema within the ossicle and impingement on the deltoid ligament.
The patient was informed about his condition and initially managed conservatively with anti-inflammatory analgesics and ankle support. Although he experienced temporary improvement, persistent medial ankle pain led to the decision to excise the ossicle after a 1-month trial of conservative treatment. Under spinal anesthesia, a direct medial approach was used to excise the ossicle while preserving the deltoid ligament (Fig. 4 and 5).

Figure 4: Intraoperative image of the ossicle.
Figure 5: Clinical image of excised ossicle.
Intraoperative findings confirmed the diagnosis of os subtibiale. Postoperatively, ankle range of motion and weight-bearing were initiated as tolerated from the 1st post-operative day. Sutures were removed 15 days after surgery. At the 1-year follow-up, the patient was pain-free and able to walk and run comfortably, with a full range of motion in the affected ankle.
The os subtibiale is an uncommon accessory ossicle located distal to the medial malleolus. Between the ages of 7 and 10 years, accessory centers of ossification may appear near the medial malleolus; in rare cases, these centers persist into adulthood, forming the so-called os subtibiale [6]. Despite its rarity, this anatomical variant has important clinical implications, as it can be mistaken for more common conditions such as medial malleolus fractures. The ossicle often goes unnoticed unless it becomes symptomatic or is specifically identified during imaging evaluation (Table 1). When symptomatic, the os subtibiale can cause pain and discomfort, typically due to mechanical irritation or stress on surrounding structures. In acute symptomatic cases with a history of ankle injury, it can easily be misdiagnosed as a medial malleolus fracture, as reported by Coral [7] and Madhuri et al. [8]. Coral [7] even fixed the os subtibiale, mistaking it for a fracture, using a tension band technique, and the patient achieved a good recovery. Turan et al. [9] described that the os subtibiale can lead to posterior tibial tendon impingement and tenosynovitis. Their patient was initially managed conservatively for 3 months but eventually underwent surgical excision of the accessory ossicle, resulting in an excellent outcome. Madhuri et al. [8] outlined several distinguishing features to differentiate the os subtibiale from a fracture. First, on radiographs, the edges of the accessory bone appear smooth and rounded, unlike the irregular margins seen in fractures. Second, the os subtibiale is typically located just beneath the medial malleolus and is often bilateral. Third, the site of maximum tenderness is generally over the adjacent ligaments rather than directly over the medial malleolus. All these findings were evident in our case, except that the patient had direct tenderness over the ossicle, possibly due to edema within the ossicle itself. The first line of treatment is typically non-operative, involving immobilization, anti-inflammatory medications, muscle stretching and strengthening exercises, and rest, as described by Topal et al. [10]. Madhuri et al. [8] also reported excellent outcomes with conservative management in their cases. In our case, we initially attempted conservative treatment, but the patient did not achieve significant symptom relief. Surgery is generally reserved for cases in which conservative management fails or when the patient’s symptoms significantly interfere with daily activities. Surgical excision of the os subtibiale often provides substantial symptom relief [9,11,12]. Based on our experience and previously reported cases, excision of the ossicle results in favorable outcomes. Bandyopadhyay [12] described an 18-year-old patient with a symptomatic os subtibiale following trauma who failed conservative treatment and subsequently underwent excision, with intraoperative findings confirming the diagnosis. The procedure may be performed through either an open or arthroscopic approach [9,12,13]. In our case, we opted for open excision of the ossicle. The prognosis is generally favorable, particularly when the condition is accurately identified and appropriately managed. With correct diagnosis and timely intervention, most patients experience complete symptom resolution and return to pain-free daily activities, as observed in our patient and several previously reported cases.
Os subtibiale is a rare accessory ossicle that is usually asymptomatic but presents a diagnostic challenge when it becomes symptomatic. This case highlights the diagnostic approach and differentiation of os subtibiale from a medial malleolus fracture non-union, as well as the role of MRI in identifying the cause of symptoms in a previously asymptomatic ossicle. Clinicians should consider os subtibiale in the differential diagnosis of medial ankle pain, even in patients with a history of trauma. Awareness of this entity and careful interpretation of imaging can help avoid misdiagnosis and inappropriate treatment.
A symptomatic os subtibiale can closely mimic a medial malleolus fracture. Awareness of this rare variant and careful imaging evaluation is essential to avoid misdiagnosis and ensure appropriate management.
References
- 1. Keles-Celik N, Kose O, Sekerci R, Aytac G, Turan A, Güler F. Accessory ossicles of the foot and ankle: Disorders and a review of the literature. Cureus 2017;9:e1881. [Google Scholar] [PubMed]
- 2. Lawson JP. International skeletal society lecture in honor of Howard D. Dorfman. clinically significant radiologic anatomic variants of the skeleton. AJR Am J Roentgenol 1994;163:249-55. [Google Scholar] [PubMed]
- 3. Bencardino JT, Rosenberg ZS. MR imaging and CT in the assessment of osseous abnormalities of the ankle and foot. Magn Reson Imaging Clin N Am 2001;9:567-78, xi. [Google Scholar] [PubMed]
- 4. Miller TT. Painful accessory bones of the foot. Semin Musculoskelet Radiol 2002;6:153-61. [Google Scholar] [PubMed]
- 5. Tsuruta T, Shiokawa Y, Kato A, Matsumoto T, Yamazoe Y, Oike T, et al. Radiological study of the accessory skeletal elements in the foot and ankle (author’s transl). Nihon Seikeigeka Gakkai Zasshi 1981;55:357-70. [Google Scholar] [PubMed]
- 6. Mellado JM, Ramos A, Salvadó E, Camins A, Danús M, Saurí A. Accessory ossicles and sesamoid bones of the ankle and foot: Imaging findings, clinical significance and differential diagnosis. Eur Radiol 2003;13 Suppl 4:L164-77. [Google Scholar] [PubMed]
- 7. Coral A. Os subtibiale mistaken for a recent fracture. Br Med J (Clin Res Ed). 1986;292:1571-2. [Google Scholar] [PubMed]
- 8. Madhuri V, Poonnoose PM, Lurstep MS. Accessory Os subtibiale: A case report of misdiagnosed fracture. Foot Ankle Online J 2009;2:3. [Google Scholar] [PubMed]
- 9. Turan A, Kose O, Acar B, Unal M. Posterior tibial tendon impingement due to os subtibiale: A case report and up-to-date review. Skeletal Radiol 2017;46:705-14. [Google Scholar] [PubMed]
- 10. Topal M, Köse A, Dinçer R, Baran T, Köse M, Çağatay Engin M. Os subtibiale: Mimicking medial malleolar fracture. Am J Emerg Med 2017;35:940.e1-3. [Google Scholar] [PubMed]
- 11. Iliev AA, Georgiev GP, Landzhov BV, Slavchev SA, Dimitrova IN, Ovtscharoff WА. Symptomatic Os subtibiale associated with chronic pain around the medial malleolus in a young athlete. Folia Med (Plovdiv) 2016;58:60-3. [Google Scholar] [PubMed]
- 12. Bandyopadhyay A. Symptomatic Os subtibiale following injury: A case report of failed conservative treatment, leading to differential diagnosis made intraoperatively. J Orthop Case Rep 2021;11:6-10. [Google Scholar] [PubMed]
- 13. Yabiku H, Nagamoto H, Tome Y, Nishida K, Kumai T. Arthroscopic resection of symptomatic ossicles of the medial malleolus combined with deltoid ligament repairs in athletes: A report of three cases. Cureus 2024;16:e64521. [Google Scholar] [PubMed]
- 14. Park HG, Sim JA, Koh YH. Posterior tibial tendon dysfunction secondary to os subtibiale impingement: A case report. Foot Ankle Int 2005;26:184-6. [Google Scholar] [PubMed]
- 15. Han SH, Choi WJ, Kim S, Kim SJ, Lee JW. Ossicles associated with chronic pain around the malleoli of the ankle. J Bone Joint Surg Br 2008;90:1049-54. [Google Scholar] [PubMed]
- 16. Vega J, Marimón J, Golanó P, Pérez-Carro L, Salmerón J, Aguilera JM. True submalleolar accessory ossicles causing impingement of the ankle. Knee Surg Sports Traumatol Arthrosc 2010;18:254-7. [Google Scholar] [PubMed]
- 17. Bellapianta JM, Andrews JR, Ostrander RV. Bilateral os subtibiale and talocalcaneal coalitions in a college soccer player: A case report. J Foot Ankle Surg 2011;50:462-5. [Google Scholar] [PubMed]
- 18. Kim JR, Nam KW, Seo KB, Shin SJ, Son IS. Treatment for symptomatic os subtibiale in a preadolescent athlete: A report of 3 cases in preadolescence. Eur J Orthop Surg Traumatol 2012;22 Suppl 1:229-32. [Google Scholar] [PubMed]
- 19. Shinohara Y, Tanaka M, Yokoi K, Kumai T, Tanaka Y. Arthroscopic resection of symptomatic ossicle of the medial malleolus: A case report. J Foot Ankle Surg 2016;55:1302-6. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair
June 1, 2026 A Rare Pediatric Cause of Lateral Foot Pain: Symptomatic Os Vesalianum Pedis Requiring Excision and Peroneus Brevis Repair February 10, 2021 Symptomatic Os Subtibiale Following Injury: A Case Report of Failed Conservative Treatment, Leading to Differential Diagnosis Made Intraoperatively
February 10, 2021 Symptomatic Os Subtibiale Following Injury: A Case Report of Failed Conservative Treatment, Leading to Differential Diagnosis Made Intraoperatively May 10, 2024 Minimally Invasive Corrective Osteotomy (MICO) of the Hand a Novel Technique
May 10, 2024 Minimally Invasive Corrective Osteotomy (MICO) of the Hand a Novel Technique June 1, 2025 Flexor Carpi Radialis Tendon Stabilization for Chronic First Carpometacarpal Joint Instability: Clinical Outcomes from a Case Report
June 1, 2025 Flexor Carpi Radialis Tendon Stabilization for Chronic First Carpometacarpal Joint Instability: Clinical Outcomes from a Case Report