
This case highlights the critical importance of early diagnosis and appropriate management of acetabular fracture-dislocations to prevent complications such as AVN and failed THA. It also underscores the value of 3D imaging, individualized staged surgical planning, and structured rehabilitation in achieving successful outcomes in complex, previously mismanaged hip injuries.
Dr M. Harshith, Department of Orthopaedics, Postgraduate Institute of Medical Education and Research, Chandigarh - 160012, India. E-mail: mharshith211@gmail.com
Abstract
Introduction: Acetabular fracture-dislocations are complex injuries that, if misdiagnosed or mismanaged, can lead to avascular necrosis and early total hip arthroplasty (THA) failure.
Case Report: A 16-year-old male with a neglected acetabular fracture-dislocation underwent an ill-planned THA, with the cup placed in fracture callus, which was removed the next day. He later presented in a Girdlestone-like state. Imaging and 3D modelling revealed a malunited posterior wall and column fracture. A staged approach – corrective osteotomy with fixation followed by revision THA – was performed.
Result: At 10 months, he achieved excellent function and stable radiographic reconstruction.
Conclusion: Early recognition, detailed pre-operative planning, and 3D-assisted individualized surgical strategies are vital for successful reconstruction of neglected or failed acetabular fracture-dislocations.
Keywords: THA, Failed THA, 3D bone model, THA post trauma, Total hip arthroplasty
The hip joint, owing to its ball-and-socket configuration and surrounding musculature, is naturally well protected against traumatic disruptions. Still, when a person is subjected to high-impact forces – like those experienced during road traffic accidents – even this robust joint can be compromised. Acetabular fractures, although not very common (estimated at around 3/100,000 people annually), are considered severe injuries [1]. They frequently occur alongside posterior dislocations of the hip, especially in young individuals subjected to high-velocity trauma [1]. These injuries demand meticulous management, not only due to the fracture itself but also because of the potential complications that can arise if the diagnosis is missed or treatment is delayed. Unfortunately, in many parts of the world, particularly in rural or resource-limited settings, the ideal management of such complex injuries is often not possible. The lack of timely access to radiological imaging, experienced orthopedic surgeons, and appropriate surgical facilities means that many of these fractures go unnoticed or are inadequately treated. When left unaddressed for weeks, these injuries evolve into what is termed a “neglected acetabular fracture” – typically defined as one left untreated for more than 3 weeks [2]. As time passes, these fractures become more complicated to deal with due to the formation of scar tissue and abnormal bone healing, which distorts normal anatomy and makes surgical reconstruction more challenging [2,3]. One of the most feared consequences in these situations is avascular necrosis (AVN) of the femoral head. This occurs when the blood supply to the femoral head is interrupted – something that is not uncommon with posterior hip dislocations [4]. Once AVN sets in, it can lead to the collapse of the femoral head and degenerative changes within the joint. The longer the hip remains dislocated – especially beyond 12–24 h – the greater the risk of this complication, with some studies reporting rates as high as 30–35% in fracture-dislocation cases [5]. The situation becomes even more precarious when a total hip replacement is attempted without recognizing an underlying acetabular fracture. In such cases, improper implant positioning, poor fixation, and biological unpreparedness of the bone can lead to early failure of the prosthesis [3]. What was meant to be a definitive solution turns into a salvage scenario, demanding more complex and technically demanding revision surgeries. This is why individualized planning, detailed imaging (including 3D reconstructions), and a full understanding of the bony architecture are essential before proceeding with arthroplasty in such cases [2]. This case report discusses the journey of a 16-year-old boy who exemplifies the cascading effects of missed diagnosis and misdirected treatment. Initially treated conservatively for a lower leg fracture, his hip injury went unrecognized until significant pain and dysfunction developed. An early attempt at hip replacement – undertaken without appreciating the underlying fracture – had to be reversed the very next day. By the time he reached our center, he was in a state functionally similar to a Girdlestone procedure. Using a staged, carefully planned surgical approach that included anatomical reduction of the acetabular fracture and revision total hip arthroplasty (THA), we were able to restore function and stability. This report not only shares the technical aspects of our approach but also reinforces the importance of early recognition, comprehensive pre-operative assessment, and customized surgical planning in such complex post-traumatic hip injuries.
A 16-year-old male sustained a road traffic accident in February 2024 and was initially managed at a local hospital, where he was diagnosed with a closed fracture of both bones of the left leg. The fracture was treated conservatively with an above-knee cast, and the patient was kept on bed rest for 3 months. Subsequently, he was mobilized using a patellar tendon-bearing cast. Upon attempting weight-bearing, the patient began experiencing significant pain in his left hip. He consulted his primary orthopedician, who diagnosed a fracture-dislocation of the left hip (Fig. 1).

Figure 1: Radiograph showing fracture dislocation of the left hip.
He was then referred to a higher center, where a magnetic resonance imaging (MRI) of the left hip was performed. The MRI revealed osteonecrosis of the femoral head; however, an associated acetabular fracture was missed in the report. Based on the available diagnosis, the patient underwent THA in July 2024. Intraoperatively, the acetabular shell was inadvertently implanted into the fracture callus (Fig. 2).

Figure 2: Radiograph showing malpositioned implant.
2016: Acute L1 fracture type A.
Postoperatively, the implant was removed on post-operative day 1 due to the intraoperative misjudgment. After this complex and distressing course of events, the patient presented to our institute in September 2024 with features resembling a post-Girdlestone status. Radiographic evaluation revealed a posterior wall and column acetabular fracture with associated foot drop (Fig. 3).

Figure 3: Radiograph with which the patient presented to our institute (PGIMER, Chandigarh).
Work-up at our institute:
We conducted a comprehensive evaluation, including radiographic studies to confirm the diagnosis, routine blood investigations to assess the general health, and rule out infection. Computed tomography (CT) scan of the pelvis, followed by construction of a 3D model of the affected hemipelvis to better understand the fracture anatomy and plan reconstruction, were also performed (Fig. 4).
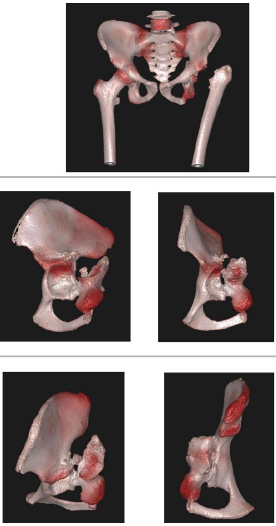
Figure 4: 3D computed tomography showing malunited posterior wall and
posterior column fracture.
Definitive management:
In October 2024, the patient was taken up for definitive surgical management. An osteotomy was performed at the malunited site. The posterior wall and column were anatomically reduced and stabilized using a pelvic reconstruction plate and two lag screws (Fig. 5). Acetabular reaming was then carried out, and a new acetabular shell was implanted. Standard steps were followed for the placement of the femoral component (Fig. 6).
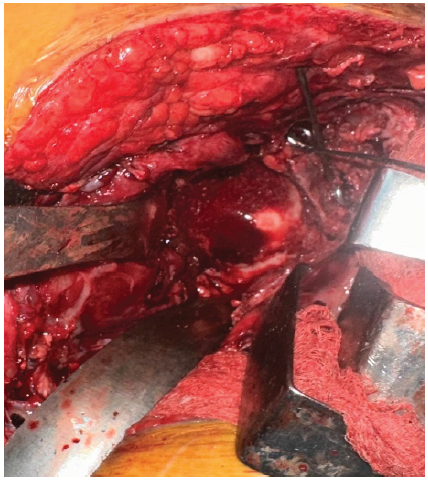
Figure 5: Intraoperative image after fracture reduction and osteosynthesis.

Figure 6: Post-operative radiograph.
Post-operative rehabilitation and follow-up:
Bedside sitting, straight leg-raising exercises, and knee range-of-motion exercises were initiated on post-operative day 1. The patient was kept non-weight-bearing for 4 weeks. After 4 weeks, he was mobilized using a walker and a foot-drop splint to assist ambulation. After 3 months, he was allowed to discontinue the walker and was instructed to use a cane/crutch as and when required. The patient has been ambulating without any aid for 4 months postoperatively. At the 10-month follow-up, the X-ray (Fig. 7) and clinical range of motion (Fig. 8) were satisfactory. The patient was ambulatory with full weight-bearing and reported no complaints.
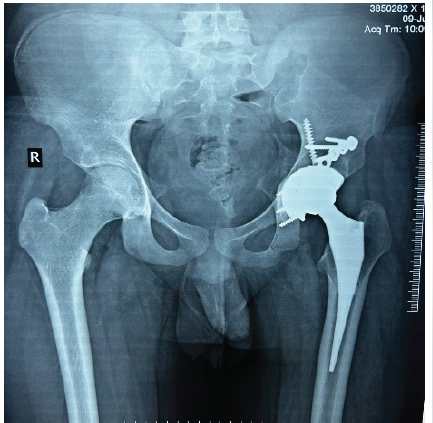
Figure 7: Radiograph at 10 months follow-up.

Figure 8: Clinical images demonstrating the mobility on the operated side at 10 months followup.
Neglected acetabular fractures represent one of the most complex challenges in orthopedic trauma. This case involving a 16-year-old male demonstrates the serious consequences of a missed diagnosis. An initially unrecognized acetabular fracture resulted in the premature performance of a THA, which subsequently failed. Definitive management required a complex surgical approach, including anatomical reduction of the posterior wall and column, followed by revision THA. Restoration of hip function and stability was achieved only through a highly individualized and staged approach. This case emphasizes the importance of early diagnosis, detailed pre-operative assessment, and personalized surgical planning in the management of acetabular injuries. Successful management of acetabular fractures demands a comprehensive understanding of pelvic anatomy due to the complex three-dimensional (3D) orientation of the acetabulum. In recent years, the use of 3D-printed pelvic models has proven beneficial in enhancing pre-operative planning. These models allow improved visualization of fracture morphology and enable more accurate pre-contouring of fixation hardware, contributing to reduced operative time, intraoperative blood loss, and radiation exposure during surgery [6]. Evidence supports the utility of 3D modeling in this context. Brouwers et al. reported that 3D-printed models significantly improved interobserver agreement in classifying acetabular fractures compared to traditional imaging modalities [7]. Furthermore, a meta-analysis conducted by Lee et al. demonstrated that the incorporation of 3D modeling was associated with reductions in operative time, blood loss, and radiation exposure in pelvic and acetabular fracture surgery [8,9]. Beyond operative metrics, 3D models also enhance intraoperative planning, interdisciplinary communication, and patient education by providing a tangible and easily interpretable representation of the injury [10]. In the present case, 3D CT imaging was critical in guiding the surgical approach. It enabled detailed planning of the corrective osteotomy and facilitated precise reduction of the malunited posterior wall and column. A major intraoperative complication occurred during the initial THA, in which the acetabular shell was inadvertently positioned within an unrecognized fracture callus. This outcome highlights the need for individualized strategies when addressing neglected or malunited acetabular fractures, particularly those involving the posterior column or transverse components, which are notably difficult to reduce once healing has begun [2]. Performing THA in the absence of stable fracture fixation often results in early implant failure. Although THA can provide favorable outcomes in cases involving post-traumatic arthritis or AVN, preserving native acetabular bone and deferring arthroplasty, especially in younger patients, is generally preferred for long-term joint preservation. Post-operative rehabilitation is a critical, though often underemphasized, component of recovery. In this case, a structured rehabilitation protocol – comprising early mobilization, assistive device use, and regular follow-up – was essential in restoring functional capacity. Comprehensive rehabilitation plays a pivotal role in optimizing long-term outcomes following complex reconstructive procedures.
Neglected acetabular fractures remain some of the most difficult injuries to diagnose and treat, often leading to serious complications if not managed properly. In this case, a missed diagnosis and an ill-planned total hip replacement in a young patient led to a complex series of setbacks. Recovery was only possible after careful pre-operative planning, including the use of 3D imaging to understand the injury in detail. With a step-by-step surgical strategy that addressed the underlying fracture and a thoughtfully executed revision hip replacement, we were able to restore function. This case underscores how critical early diagnosis, personalized surgical planning, and the use of advanced imaging can be in achieving good outcomes in challenging post-traumatic hip injuries.
Neglected acetabular fractures demand meticulous evaluation and staged management; 3D-based pre-operative planning and fracture stabilization before arthroplasty are key to achieving durable results.
References
- 1. Nicholson JA, Scott CE, Annan J, Ahmed I, Keating JF. Native hip dislocation at acetabular fracture predicts poor long-term outcome. Injury 2018;49:1841-7. [Google Scholar] [PubMed]
- 2. Dilogo IH, Tobing JF. Neglected acetabular fracture: Fix or replace? J Clin Orthop Trauma 2017;8:S3-10. [Google Scholar] [PubMed]
- 3. Veerappa LA, Tripathy SK, Sen RK. Management of neglected acetabular fractures. Eur J Trauma Emergency Surg 2015;41:343-8. [Google Scholar] [PubMed]
- 4. Konarski W, Poboży T, Śliwczyński A, Kotela I, Krakowiak J, Hordowicz M, et al. Avascular necrosis of femoral head-overview and current state of the art. Inter J Environ Res Public Health 2022;19:7348. [Google Scholar] [PubMed]
- 5. Milenkovic S, Mitkovic M, Mitkovic M. Avascular necrosis of the femoral head after traumatic posterior hip dislocation with and without acetabular fracture. Eur J Trauma Emerg Surg 2022;48:618-9. [Google Scholar] [PubMed]
- 6. Ansari S, Barik S, Singh SK, Sarkar B, Goyal T, Kalia RB. Role of 3D printing in the management of complex acetabular fractures: A comparative study. Eur J Trauma Emerg Surg 2021;47:1291-6. [Google Scholar] [PubMed]
- 7. Brouwers L, Pullter Gunne AF, De Jongh MA, Van Der Heijden FH, Leenen LP, Spanjersberg WR, et al. The value of 3D printed models in understanding acetabular fractures. 3D Print Addit Manuf 2018;5:37-46. [Google Scholar] [PubMed]
- 8. Lee AK, Lin TL, Hsu CJ, Fong YC, Chen HT, Tsai CH. Three-dimensional printing and fracture mapping in pelvic and acetabular fractures: A systematic review and meta-analysis. J Clin Med 2022;11:5258. [Google Scholar] [PubMed]
- 9. Ivanov S, Valchanov P, Hristov S, Veselinov D, Gueorguiev B. Management of complex acetabular fractures by using 3D printed models. Medicina (Kaunas) 2022;58:1854. [Google Scholar] [PubMed]
- 10. Manganaro MS, Morag Y, Weadock WJ, Yablon CM, Gaetke-Udager K, Stein EB. Creating three-dimensional printed models of acetabular fractures for use as educational tools. Radiographics 2017;37:871-80. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report
August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report