
Knowing exact beath pin length needed avoids risk of over penetration and complications due to it.
Dr. Hitendra G. Patil, Shri Guruji Hospital, Gangapur Road, Nashik, Maharashtra - 422 013, India. E-mail: drhitendrapatil@gmail.com
Abstract
Introduction: Arthroscopic jigs are specialized surgical instruments used in arthroscopy for drilling bone tunnels at the desired location. Neurovascular complications are known due to accidental over penetration of the beath pin in the posterior compartment.
Surgical Technique: We have provided a simple method to determine the minimum length needed of the beath pin so that when the chuck of the drill touches the stopper of the drill sleeve, we are sure that the beath pin has just exited at the desired point marked by the targeting guide and cannot go beyond that.
Conclusion: Our technique of accurate beath pin measurement avoids over penetration of beath pin while using an Arthroscopy jig and thus avoids neurovascular complications.
Keywords: Beath pin, arthroscopy jig, neurovascular injury.
Arthroscopic jigs are valuable tools in orthopedic surgery mainly used for ligament reconstruction and meniscus repair procedures [1,2,3,4,5]. They help to create accurate tunnel needed for arthroscopy procedures. Many a times when there is slight play in the jig or slight bend in the beath pin, the beath pin might get slip of from the stopping point of the arm of the jig and if the surgeon or assistant missed the feel of second cortex, it may penetrate in the soft tissue which may cause neurovascular injury. We present a simple trick to accurately measure the exact length of the beath pin so that the drill automatically stops when the tip of the beath pin exits the desired point chosen by the jig.
Arthroscopic jig consist of handle, targeting guide arm and drill sleeve (commonly called as bullet). First, we have to completely insert the drill sleeve inside the handle till the stopper (outer end) sits flush to the handle (Fig. 1a). Pass the beath pin completely till it reaches the exit point determined by the targeting guide arm (Fig. 1b). Mark the portion of the beath pin just outside the sleeve and measure the length (Fig. 1c).
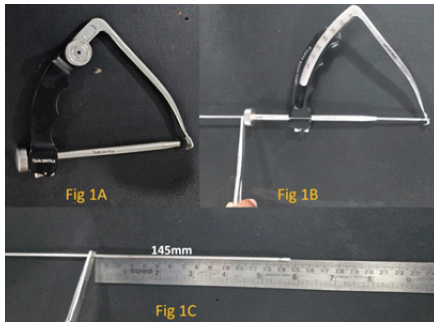
Figure 1: (a-c) When the drill sleeve is fully inserted, the basic length of beath pin measured is 145 mm.
In our case it is 145 mm. Then apply the jig to the bone (in our case tibia) such that the targeting guide arm is at desire point inside the joint and the drill sleeve touches the bone outside and lock it. Now measure the distance between the outermost part of the handle of jig where the drill sleeve is inserted and the inner margin of the stopper of drill sleeve (Fig. 2).
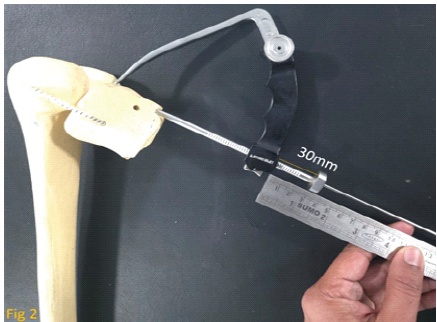
Figure 2: Place the Jig at the appropriate point and lock of drill sleeve. The length of the drill sleeve outside from the handle is measured (30 mm).
In our case it is 30 mm. Hence, now 145 + 30 = 175 mm will be minimum length of beath pin needed. Mark the 175 mm mark on the beath pin and attach the drill at 175 mm mark (Fig. 3a). Hence, now you can safely drill till the chuck of the drill touches the stopper of drill sleeve and you will find the beath pin has just exited at the desire point marked by targeting guide and cannot go beyond that (Fig. 3b).

Figure 3: (a and b) Now the minimum length of beath pin needed is 145 + 30 = 175mm. Drill is attached to the beath pin at this length. We will find that when the drill touches the stopper of drill sleeve beath pin has just exited at the desire point marked by targeting guide and cannot go beyond that.
The primary purpose of an arthroscopic jig is to guide the precise placement and drilling of tunnels or fixation points in bones during arthroscopic procedures. For instance, in posterior cruciate ligament (PCL) reconstruction surgery performed using arthroscopy, PCL jigs are used to accurately position and drill tunnels in the tibia for passage of the graft. Many a times when there is slight play in the jig or slight bend in the beath pin, the beath pin might get slip of from the stopping point of the guide arm of the jig and if the surgeon or assistant missed the feel of second cortex, it may penetrate in the soft tissue which may cause neurovascular injury. This is a common threat in tibial tunnel placement in PCL reconstruction [6,7,8]. Same thing happens while creating tunnel for medial or lateral meniscus posterior root repair at the anatomical point [9,10]. If the surgeon or assistant miss the feel of second cortex while drilling beath pin it may go in posterior compartment and hit the neurovascular structures. Our technique of exact beath pin length measurement avoids this complication. Most of the times, surgeon is holding the jig at the desired point, so he has to depend on the assistant to drill. Our trick avoids the need of expert assistant to drill. When the chuck of the drill touches the stopper of the drill sleeve, we are sure that the beath pin has just exited at the desired point marked by the targeting guide and cannot go beyond that.
Our technique of accurate beath pin measurement avoids over penetration of beath pin while using with an Arthroscopy jig and thus avoids neurovascular complications.
Knowing exact beath pin length needed avoids risk of over penetration and complications due to it.
References
- 1. Razi M, Ghaffari S, Askari A, Arasteh P, Ziabari EZ, Dadgostar H. An evaluation of posterior cruciate ligament reconstruction surgery. BMC Musculoskelet Disord 2020;21:526. [Google Scholar] [PubMed]
- 2. Sookun PG, Jeetun H, Wang S, Zhang Z. Modified arthroscopic technique for repair of medial meniscus posterior root tear and centralization of the extruded Medial meniscus through a double transtibial tunnel (without use of accessory ports). Arthrosc Tech 2025;14:103888. [Google Scholar] [PubMed]
- 3. Keel TJ, Guerin G, Tollefson LV, Slette EL, Shoemaker EP, LaPrade RF. Transtibial tunnel and combined hashtag inside-out repair of lateral meniscus radial tear With marrow venting. Video J Sports Med 2025;5:26350254241305418. [Google Scholar] [PubMed]
- 4. Bhargava R, Sancheti P, Shyam A. Do the ACL reconstruction outcomes with hamstring autografts depend on percentage of native ACL tibial footprint area restored? Indian J Orthop 2025;59:1911-6. [Google Scholar] [PubMed]
- 5. Shetty SM, Alladu HK. The sironix ACL Jig: A solution for tibial tunnel angle and length. J Clin Orthop Trauma Care 2022;4:1-6. [Google Scholar] [PubMed]
- 6. Jackson DW, Proctor CS, Simon TM. Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. Arthroscopy 1993;9:224-7. [Google Scholar] [PubMed]
- 7. James EW, Taber CE, Marx RG. Complications associated with posterior cruciate ligament reconstruction and avoiding them. J Knee Surg 2021;34:587-91. [Google Scholar] [PubMed]
- 8. Marom N, Ruzbarsky JJ, Boyle C, Marx RG. Complications in posterior cruciate ligament injuries and related surgery. Sports Med Arthrosc Rev 2020;28:30-3. [Google Scholar] [PubMed]
- 9. Wu TY. Arthroscopic medial meniscus posterior root repair with centralization using knotless suture anchors. Arthrosc Tech 2022;11:e661-8. [Google Scholar] [PubMed]
- 10. Iqbal MS, Sood M, kaul R. Popliteal artery pseudoaneurysm following arthroscopic lateral meniscus root repair. Future Health 2025;3:50-2. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Anterior Bridge Plate Through Minimally Invasive Approach: A Game-changer for Humeral Shaft Fracture: A Clinical Case Series
May 1, 2026 Anterior Bridge Plate Through Minimally Invasive Approach: A Game-changer for Humeral Shaft Fracture: A Clinical Case Series March 10, 2024 Spontaneous Idiopathic Bilateral Sagittal Band Rupture: A Case Report
March 10, 2024 Spontaneous Idiopathic Bilateral Sagittal Band Rupture: A Case Report January 16, 2014 Authors Reply: Progressive Brachial Plexus Palsy after Osteosynthesis of an Inveterate Clavicular Fracture
January 16, 2014 Authors Reply: Progressive Brachial Plexus Palsy after Osteosynthesis of an Inveterate Clavicular Fracture January 1, 2026 From Hip Effusion to Hemophilia: Unveiling the Cause of Pain in 6-Month-Old Infant. A Case Report
January 1, 2026 From Hip Effusion to Hemophilia: Unveiling the Cause of Pain in 6-Month-Old Infant. A Case Report