
Sacral insufficiency fracture should be suspected as a cause of early post-operative radiculopathy after lumbosacral fusion, particularly in patients with impaired bone quality.
Dr. Joaquín Zúñiga Soria, Universidad del Desarrollo - Clínica Alemana de Santiago, Santiago, Chile. E-mail: j.zunigas@udd.cl
Abstract
Introduction: Sacral insufficiency fracture (SIF) is an uncommon but increasingly recognized complication following lumbosacral fusion, particularly in patients with compromised bone quality. The biomechanical vulnerability of the L5–S1 junction, combined with altered load transfer after anterior and posterior reconstruction, may predispose to early sacral failure. fusion, corticosteroid-associated bone fragility, cage subsidence, spinopelvic biomechanics, lytic spondylolisthesis, lumbosacral junction.
Case Report: A 55-year-old male with lytic spondylolisthesis at L5–S1, repeated corticosteroid exposure, and neurogenic claudication underwent staged circumferential L4–S1 fusion (L5–S1 anterior lumbar interbody fusion, L4–L5 oblique lumbar interbody fusion, and percutaneous posterior fixation). Initial post-operative recovery was satisfactory. At 8 weeks, the patient developed recurrent lumbosciatica. Computed tomography (CT) demonstrated collapse of the S1 superior endplate with anterior cage subsidence and foraminal compromise. Revision surgery included bilateral L5–S1 foraminal decompression and posterior refixation. Persistent unilateral radiculopathy required re-exploration, revealing a mobile bone fragment causing dynamic nerve compression, which was resected. The patient subsequently experienced progressive pain relief and returned to functional activity. Radiographs at 8 months confirmed advanced fusion and fracture consolidation.
Discussion: SIF after circumferential fusion may be precipitated by corticosteroid-associated bone fragility, preexisting pars defects, and increased shear forces across the lumbosacral junction. Early symptoms may mimic post-operative radiculopathy, contributing to delayed diagnosis. CT is the most sensitive modality for early detection. Revision strategies include posterior decompression and reinforcement of fixation; in higher-risk cases, pelvic fixation may be warranted.
Conclusion: Sacral fracture after lumbosacral fusion requires a high index of suspicion in osteoporotic patients presenting with recurrent radicular pain. Comprehensive biomechanical planning and pre-operative bone density evaluation are essential to mitigate risk.
Keywords: Sacral insufficiency fracture, circumferential fusion, anterior lumbar interbody fusion/oblique lumbar interbody
Circumferential lumbosacral fusion is commonly used for the treatment of lytic spondylolisthesis and foraminal stenosis, aiming to restore segmental alignment and achieve solid arthrodesis through combined anterior and posterior fixation [1,2]. The L5–S1 junction is a biomechanically vulnerable transition zone subjected to high shear forces, particularly in patients with pars defects and high pelvic incidence [3]. Sacral insufficiency fractures (SIF) have been increasingly recognized as a complication following lumbosacral fusion, especially in patients with compromised bone quality [4-6]. Risk factors include osteoporosis, corticosteroid use, and constructs terminating at S1 without pelvic fixation [5-7]. Pre-operative assessment of bone quality, including dual-energy X-ray absorptiometry (DEXA) or computed tomography (CT)-based Hounsfield units, has been shown to be critical in predicting mechanical complications such as cage subsidence and sacral failure [8-10]. We present a case of early SIF following L4–S1 circumferential fusion in a patient with corticosteroid-associated bone fragility, highlighting diagnostic challenges and surgical decision-making.
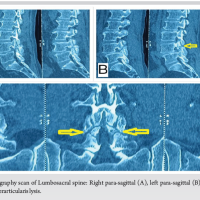
A 55-year-old male with a history of repeated corticosteroid exposure presented with a 3-month history of right-sided lumbosciatica, progressive paresthesias, and neurogenic claudication at approximately two blocks of ambulation. Magnetic resonance imaging demonstrated a grade I lytic spondylolisthesis at L5–S1 with severe foraminal stenosis and an L4–L5 disc herniation in the setting of a congenitally narrow canal (Fig. 1).
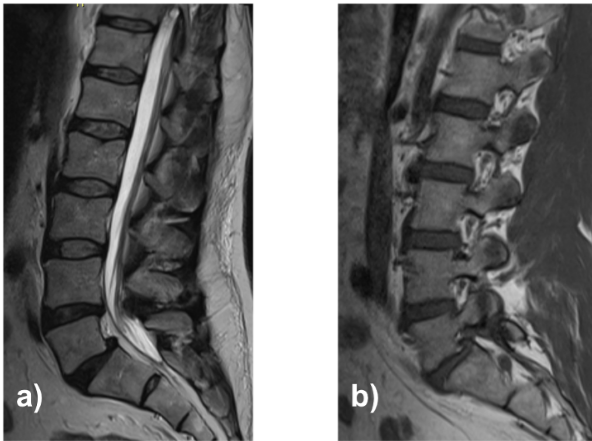
Figure 1: Lumbosacral magnetic resonance imaging: Sagittal T2-weighted (a) and right parasagittal T1-weighted (b).
Initial management included pregabalin, multiple corticosteroid courses (oral and intramuscular), two facet joint injections, and physical therapy without clinical benefit.

Figure 2: Dynamic lateral lumbar spine radiographs in flexion (a), neutral position (b), and extension (c).
Dynamic radiographs confirmed a stable grade I lytic anterolisthesis at L5–S1 and mild degenerative retrolisthesis at L4–L5 (Fig. 2). Full-spine standing radiographs showed pelvic incidence 70°, lumbar lordosis 68°, segmental lordosis L4–S1 42°, sacral slope 48°, thoracic kyphosis 45°, and sagittal vertical axis −12 mm, consistent with globally compensated sagittal alignment (Fig. 3).
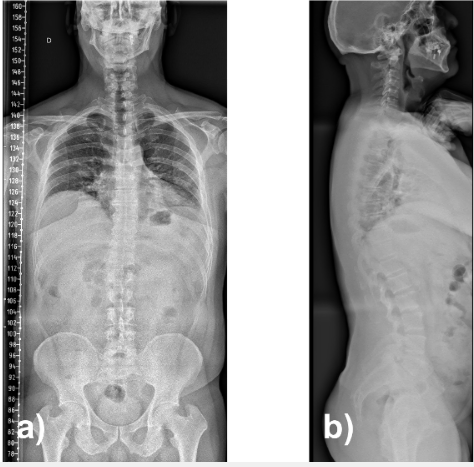
Figure 3: Full-spine radiographs in anteroposterior (a) and lateral (b) projections.
Given persistent symptoms and radiographic findings, a staged circumferential L4–S1 fusion was planned. Pre-operative bone mineral density assessment was not performed.
First, an L5–S1 anterior lumbar interbody fusion via a retroperitoneal approach was performed with complete discectomy and placement of a lordotic interbody cage achieving partial reduction of the listhesis. Second, an oblique lumbar interbody fusion at L4–L5 was performed through a left anterolateral approach with cage insertion and grafting. Finally, percutaneous posterior pedicle screw fixation from L4 to S1 was completed in the prone position. Construct alignment and fixation were satisfactory (Fig. 4), and the patient was discharged on post-operative day 3 with no neurological deficits.
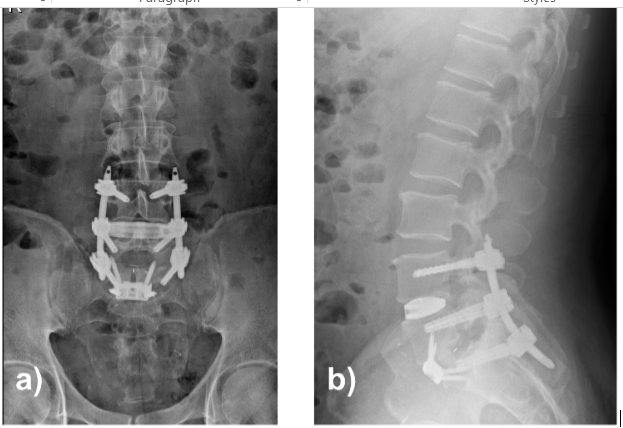
Figure 4: Lumbar spine radiographs in anteroposterior (a) and sagittal (b) projections. Solid fixation and restoration of the sagittal alignment are observed.
On post-operative day 6, the patient developed respiratory symptoms and was diagnosed with organizing pneumonia, which was treated with corticosteroids with a good clinical response.
At approximately 8 weeks postoperatively, the patient developed recurrent, progressively severe right-sided lumbosciatica. CT revealed collapse of the S1 superior endplate with anterior cage subsidence, loss of indirect foraminal decompression, and recurrent L5–S1 foraminal stenosis (Fig. 5). Revision surgery included bilateral L5–S1 foraminotomies and refixation using the existing rods, with stable reconstruction achieved.
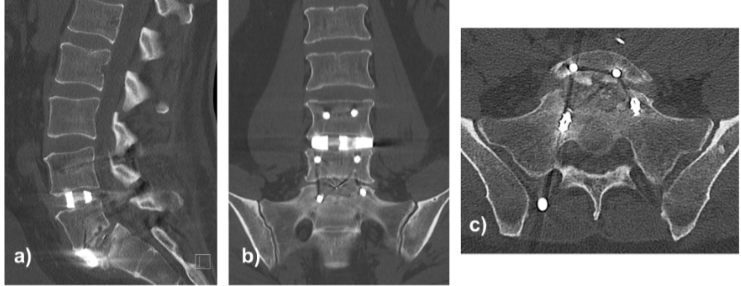
Figure 5: Lumbosacral computed tomography scan in sagittal (a), coronal (b), and axial (c) views depicting fracture of the superior endplate of S1 and anterior cage subsidence.
Early post-operative improvement was followed by new persistent left-sided radiculopathy. CT demonstrated a subfascial fluid collection, and re-exploration was performed. Hematic fluid was evacuated, and a mobile osseous fragment at the proximal S1 dome and L5 axilla was identified, causing dynamic root compression. The fragment was resected, and decompression extended. The construct remained stable. The patient was subsequently referred to endocrinology, where treatment for osteoporosis was initiated. Over subsequent follow-up, the patient demonstrated progressive reduction in radicular and axial pain with functional recovery. At final follow-up, the patient remained clinically stable without recurrence of symptoms, with imaging confirming progressive fusion and consolidation of the S1 fracture (Fig. 6).
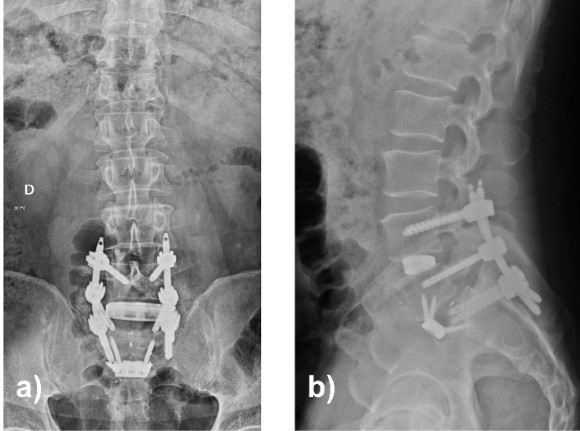
Figure 6: Lumbosacral radiographs 8 months postoperatively in anteroposterior (a) and lateral (b) projections.
SIFs following lumbosacral fusion are increasingly recognized but remain underdiagnosed complications. Several reports have described early sacral failure after short-segment constructs ending at S1, particularly in patients with compromised bone quality [4–6]. In this case, the combination of bilateral pars defects, anterior column reconstruction, and corticosteroid-associated bone fragility likely contributed to increased stress at the sacral dome, resulting in early endplate collapse and cage subsidence. Similar mechanisms have been reported in previous case series of post-fusion SIFs [5,7]. Diagnosis may be challenging, as symptoms often mimic recurrent radiculopathy, and radiographs may appear normal in early stages. Computed tomography remains the most sensitive imaging modality for early detection [11]. Surgical management should be individualized. While lumbopelvic fixation has been recommended in high-risk patients, posterior decompression and reinforcement of fixation without pelvic extension may be sufficient in selected cases, as demonstrated in this patient [7,12]. This case highlights the importance of pre-operative bone quality assessment and careful surgical planning in patients at risk of fragility-related complications.
Limitations
A limitation in this case is the absence of pre-operative bone mineral density evaluation, which may have helped identify the risk of insufficiency fracture. Although a formal bone mineral density evaluation was not performed preoperatively, the patient had multiple risk factors for poor bone quality, including repeated corticosteroid exposure.
SIF after short-segment circumferential lumbosacral fusion is an uncommon but clinically significant complication that may be under-recognized in the early post-operative period. Patients with lytic spondylolisthesis, compromised posterior tension band, and metabolic bone fragility – particularly corticosteroid-associated bone fragility – are at heightened risk due to altered biomechanics and reduced endplate strength. Early post-operative radicular symptoms or axial pain out of proportion to expected recovery should raise suspicion for sacral endplate failure, as conventional radiographs may appear normal, and computed tomography is the most sensitive modality for detection. In symptomatic cases, surgical revision is warranted, with goals of restoring neural decompression and construct stability. While lumbopelvic fixation with S2-alar-iliac instrumentation has demonstrated biomechanical advantages in high-risk patients, targeted posterior revision with stable hardware retention may be sufficient when global alignment is preserved and bone stock remains adequate, as illustrated in this case. Underlying conditions affecting bone metabolism, such as corticosteroid exposure, should raise concern for increased risk of insufficiency fractures, particularly when formal bone density evaluation is not available. Proactive strategies – including pre-operative bone quality assessment using DEXA and/or CT Hounsfield units, optimization of bone metabolism in steroid-treated patients, anterior cage placement at the ring apophysis, and consideration of prophylactic pelvic fixation in select individuals – may reduce the risk of post-operative sacral collapse. Ultimately, a tailored approach based on biomechanical demands and patient-specific bone quality is essential to improve outcomes and minimize revision burden in lumbosacral fusion surgery.
SIF should be suspected in patients with recurrent radicular pain after lumbosacral fusion, especially in those with corticosteroid exposure or poor bone quality. Early CT imaging and pre-operative bone assessment are essential to prevent delayed diagnosis and mechanical failure.
References
- 1. Bridwell KH, Lenke LG, McEnery KW, Baldus C, Blanke K. Anterior fresh frozen structural allografts in the thoracic and lumbar spine. Spine (Phila Pa 1976) 1995;20:1410–8. [Google Scholar] [PubMed]
- 2. Holderread BM, Shin CP, Syed IY, Avramis I, Rizkalla JM. Sacral insufficiency fracture after lumbosacral decompression and fusion. Proc (Bayl Univ Med Cent) 2022;35:451–4. [Google Scholar] [PubMed]
- 3. Odate S, Shikata J, Kimura H, Soeda T. Sacral fracture after instrumented lumbosacral fusion: Analysis of risk factors from spinopelvic parameters. Spine (Phila Pa 1976) 2013;38:E223–9. [Google Scholar] [PubMed]
- 4. Yagi M, King AB, Boachie-Adjei O. Sacral insufficiency fractures after multilevel spinal instrumentation and fusion for adult deformity. Spine 2012;37:E620–4. [Google Scholar] [PubMed]
- 5. Kolz JM, Mitchell SA, Elder BD, Sebastian AS, Huddleston PM, Freedman BA. Sacral insufficiency fracture following short-segment lumbosacral fusion: Case series and review of the literature. Global Spine J 2022;12:267–77. [Google Scholar] [PubMed]
- 6. Lee SH, Kim DH, Park JH, Lee DG, Park CK, Kang DH. Incidence and risk factors of sacral fracture following lumbosacral fusion for degenerative spinal stenosis with a minimum follow-up of 2 years: A case-control study. World Neurosurg 2024;191:e633–43. [Google Scholar] [PubMed]
- 7. Buell TJ, Yener U, Wang TR, Buchholz AL, Yen CP, Shaffrey ME, et al. Sacral insufficiency fractures after lumbosacral arthrodesis: Salvage lumbopelvic fixation and a proposed management algorithm. J Neurosurg Spine 2020;33:225–35. [Google Scholar] [PubMed]
- 8. Klineberg E, McHenry T, Bellabarba C, Wagner T, Chapman J. Sacral insufficiency fractures caudal to instrumented posterior lumbosacral arthrodesis. Spine (Phila Pa 1976) 2008;33:1806–11. [Google Scholar] [PubMed]
- 9. Singh M, Kim J, Nassar J, Xu A, Peresuh S, Shah K, et al. Generation and validation of a Hounsfield unit threshold for predicting mechanical complications following thoracolumbar or lumbar fusion: A systematic review and meta-analysis. Eur Spine J 2025. [Google Scholar] [PubMed]
- 10. Xu S, Liu X, Meng X. Endplate Hounsfield units outperform lumbar HU and VBQ in predicting cage subsidence after posterior lumbar interbody fusion: A retrospective cohort study. Eur Spine J 2025;34:4140–50. [Google Scholar] [PubMed]
- 11. Dougherty RW, Fessler RG. Spinal insufficiency fractures after fusion. Neurosurg Focus 2013;35:E3. [Google Scholar] [PubMed]
- 12. Rahmani R, Stegelmann SD, Andreshak T. S2 alar-iliac screws are superior to traditional iliac screws for spinopelvic fixation in adult spinal deformity: A systematic review and meta-analysis. Spine Deform 2024;12:829–42 [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 10, 2024 Hemorrhagic Ligamentum Flavum Cyst in the Adjacent Level of Lytic Spondylolisthesis – A Case of Diagnostic and Therapeutic Dilemma
April 10, 2024 Hemorrhagic Ligamentum Flavum Cyst in the Adjacent Level of Lytic Spondylolisthesis – A Case of Diagnostic and Therapeutic Dilemma July 30, 2019 The Limb beyond Salvage: A Case Report on Two Cases of Fibroblastic Variants of Osteosarcoma
July 30, 2019 The Limb beyond Salvage: A Case Report on Two Cases of Fibroblastic Variants of Osteosarcoma December 10, 2022 Analysis of Functional Outcomes Following Surgical Management of Neglected Multiple Carpometacarpal Dislocations: A Series of 4 four Cases and Review of Literature
December 10, 2022 Analysis of Functional Outcomes Following Surgical Management of Neglected Multiple Carpometacarpal Dislocations: A Series of 4 four Cases and Review of Literature May 1, 2025 Management of Chronic Achilles Tendon Rupture with Tibialis Anterior Allograft: A 2-Year Follow-up Study
May 1, 2025 Management of Chronic Achilles Tendon Rupture with Tibialis Anterior Allograft: A 2-Year Follow-up Study