
Careful clinical evaluation combined with LRINEC scoring and imaging can effectively distinguish benign subcutaneous emphysema from necrotizing fasciitis, preventing unnecessary surgical intervention.
Dr. Jamil Haddad, Department of Orthopedic Surgery, McLaren Macomb McLaren Macomb, 1000 Harrington St, Mount Clemens, Michigan 48043, United States. E-mail: jamil.haddad1@mclaren.org
Abstract
Introduction: Subcutaneous emphysema (SE) of the upper extremity following minor trauma is a rare clinical presentation that can closely mimic necrotizing fasciitis (NF), a life-threatening surgical emergency. This report presents a case of non-infectious SE of the hand, with emphasis on diagnostic strategies to differentiate it from NF and guide appropriate management to avoid unnecessary surgery.
Case Report: A 64-year-old male presented to the Emergency Department with swelling and crepitus of the right hand 10 h after sustaining a minor laceration from a pen knife. The patient reported using hydrogen peroxide for wound irrigation before symptom onset. Clinical examination revealed extensive subcutaneous air on palpation with preserved distal neurovascular status. Laboratory evaluation showed normal inflammatory markers, and the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score was 0, indicating low risk for NF. Radiographs and computed tomography imaging demonstrated widespread SE without abscess or cortical destruction. The patient was admitted for close monitoring and empiric antibiotics. Serial examinations remained stable with no signs of clinical deterioration. The patient was discharged on oral antibiotics and remained complication-free with full functional recovery at 1-year follow-up.
Conclusion: Non-infectious SE of the upper extremity is an uncommon but important differential diagnosis in cases of post-traumatic soft tissue swelling with crepitus. Careful clinical assessment, use of risk stratification tools, such as the LRINEC score, and appropriate imaging are critical to distinguish benign SE from NF. Awareness of this entity can help prevent unnecessary surgical intervention and improve patient outcomes.
Keywords: Subcutaneous emphysema, necrotizing fasciitis, upper extremity.
Subcutaneous emphysema (SE) involves the presence of air or gas within the subcutaneous tissue [1]. It can result from various sources, including surgical procedures, trauma, infections, or spontaneous events [1,2]. While SE in the hand and upper extremities following minor trauma is rare, it has been reported in a few clinical cases [1,3,4,5,6,7,8,9]. Healthy patients with minor trauma-induced SE, as presented in this case, typically do not warrant intensive or surgical treatment. Most patients with uncomplicated traumatic SE can be effectively managed with conservative treatment, including proper wound care and antibiotics [1,10]. This approach is recommended for patients who are systemically stable, have minimal pain, and show no signs of extensive cellulitis [9,11]. However, consideration for necrotizing fasciitis (NF) must be made through a thorough review of the patient’s history, clinical examination, and evaluation of the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, clinicians can guide management appropriately and prevent unwarranted surgical intervention in a high-stakes diagnosis [1,12]. The LRINEC score, developed by Wong et al. in 2004, uses six laboratory values – C-reactive protein (CRP), total white blood cell (WBC) count, hemoglobin (Hgb), sodium, creatinine, and glucose – to stratify patients into low, medium, or high risk for NF [12,13]. A score of 6 or more is concerning, while a score above 8 is highly predictive of the disease [1]. Distinguishing SE from more severe conditions, such as NF, is critical due to the rapid progression and potential for extensive damage involving the skin, fascia, subcutaneous tissues, and muscle [1]. This condition is frequently associated with an external injury that introduces skin or environmental pathogens into the deeper soft tissue layers [14]. The presence of acute swelling with crepitus on physical examination and subcutaneous gas seen on radiographs suggests a necrotizing soft tissue infection (Fig. 1) [14,15]. The incidence of NF is estimated to range from 0.3 to 15 cases/100,000 people [16].

Figure 1: Anteroposterior and lateral of the right forearm radiographs revealing soft tissue gas from the first and second webspace going proximal up the volar and lateral forearm.
Limb-related NF has a 30% mortality rate, underscoring the need for early diagnosis and timely surgery [17]. Distinguishing benign subcutaneous emphysema (BSCE) from necrotizing infections is crucial, as misdiagnosis can lead to unnecessary surgery or, conversely, delayed treatment results in severe consequences, such as amputation or death [1,14]. This case report describes non-infectious SE from minor hand trauma and offers recommendations for differentiating benign SE from serious infections to prevent unnecessary surgical intervention.
Patient presentation
A 64-year-old right-hand-dominant male with no medical history presented with a swollen, painful right hand 10 h after a pen knife injury to the first web space. He irrigated the wound with hydrogen peroxide, but developed mild local numbness, tingling, and swelling 6 h later. He denied fever or chills. Examination revealed diffuse subcutaneous crepitus on the dorsum of the hand and forearm with intact distal sensation. Tetanus vaccination was updated. Vital signs were stable. Radiographs showed widespread SE, prompting an orthopedic consultation. The patient was admitted for observation to rule out NF. A contrast-enhanced computed tomography (CT) confirmed SE extending to the deltoid without abscess or cortical destruction (Fig. 2, 3, 4). Empiric IV antibiotics (Vancomycin, Zosyn, and Clindamycin) were initiated.
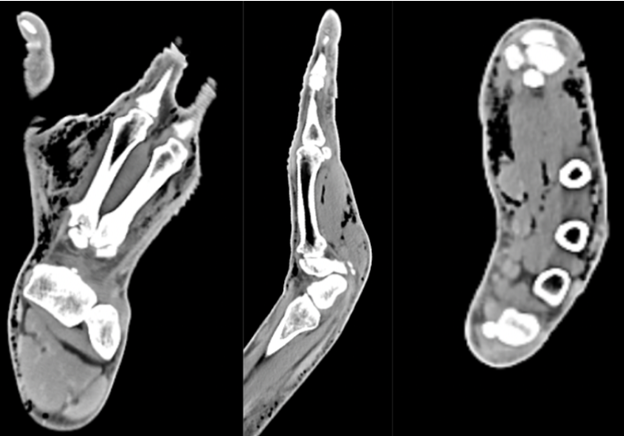
Figure 2: Computed tomography of right hand with contrast reveals no focal cortical destruction or osseous abnormality. There was moderate scattered subcutaneous emphysema diffusely through the hand.
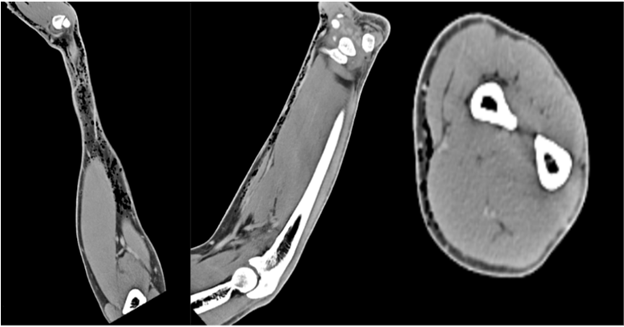
Figure 3: Computed tomography of right forearm with contrast reveals no focal cortical destruction or osseous abnormality. There was moderate scattered subcutaneous emphysema throughout the volar aspect of the forearm.
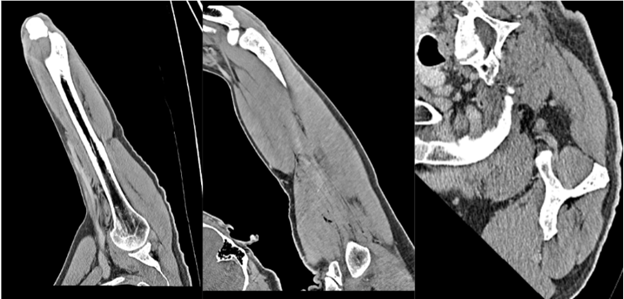
Figure 4: Computed tomography of right arm with contrast reveals no focal cortical destruction or osseous abnormality. There was mild soft tissue emphysema tracking and interspersed in the mid deltoid muscle with no drainable abscess.
On evaluation by the Orthopedic Surgery resident, the patient had mild non-pitting swelling of the right hand and forearm with a 3 mm superficial laceration in the first webspace without bleeding, erythema, or drainage (Fig. 5).

Figure 5: Clinical photos of the benign appearing forearm on initial clinical examination, revealing no obvious abnormalities besides the (non-pictured) distal 3 mm superficial laceration in the first webspace.
No bullae or tenderness were noted, and compartments were soft. Significant crepitus was present on the volar and dorsal hand and forearm, extending to the proximal forearm but absent at the elbow or humerus. Sensation was intact, motor strength was 5/5 in all muscle groups, and there was no pain with passive stretching. The initial blood work from the Emergency Department revealed a WBC of 6.34 K/mcl. (Normal: 4.5–10). CRP of <0.29 mg/dL (Normal <0.30 mg dL). Sodium (Na) of 143 mmol/L (Normal 135–147). Glucose of 96 mg/dL (Normal 70–110). Hgb of 13.9 g/dL (Normal 13.0–17.0). Creatinine (Cr) of 1.050 mg/dL (Normal 0.550–1.300). LRINEC score was calculated and found to be 0, putting the patient at a low risk for NF. The patient was admitted due to concern for infection with gas-producing bacteria, which could progress to NF. A low threshold for surgery was discussed, and he was monitored closely every 2 h. Repeat compartment checks showed no bullae or expansile emphysema. Range of motion remained full and painless, with an unchanged neurovascular exam. Twelve hours after presentation, repeat labs remained normal: CRP <0.29, WBC 5.15, Na 143, glucose 13.2, Hgb 13.2, and Cr 0.970. The LRINEC score increased to 1 due to a minor Hgb drop (13.9–13.2). On Day 2, labs remained stable (WBC 4.24, Na 139, glucose 100, Hgb 13.6, Cr 1.1). After 24 h of stable SE and examinations, the patient was discharged on clindamycin 300 mg q8h and levofloxacin 500 mg qd for 10 days, with PCP follow-up. At 1-year follow-up, the patient had full range of motion, was neurovascularly intact, and showed no contractures, chronic infection, or residual SE.
Reports of non-infectious SE following minor skin trauma are uncommon [7,14,18,19]. It is essential to differentiate non-infectious SE from severe infections caused by gas-producing pathogens, such as Clostridium perfringens or group A streptococcus (GAS) [14,15]. Clostridial gas gangrene typically manifests within 12–18 h post-injury and progresses rapidly, whereas non-clostridial infections often have a slower onset over several days and frequently occur in patients with chronic underlying conditions [14]. Common causes of SE include injuries involving the thoracic cavity, sinus or facial bones, barotrauma, bowel perforation, surgical procedures, and pulmonary blebs [20]. A 10-year analysis found the average age of patients with SE was 53 ± 14.83 years, with 71% being male [20,21,22]. SE can result from parietal pleura injury, allowing air to infiltrate pleural and subcutaneous tissues, alveolar air traveling through the endovascular sheath, or mediastinal air spreading into cervical tissues [20]. External air sources or gas from necrotizing infections may also contribute [23]. A minor hand or wrist puncture can act as a one-way valve, trapping air in soft tissues, a process described by Kemp and confirmed by Brummelkamp in cadaver studies [14,24]. Continued motion can cause progressive air buildup, known as “sucking wounds” [6,25]. CT scans are crucial for detecting gas pockets and identifying injury sources not seen on X-rays [20]. Non-infectious traumatic SE should be considered a diagnosis of exclusion, and it is crucial to rule out NF due to its rapid progression and potential for severe outcomes, including limb amputation or death [6]. NF, first identified in the late 1800s and named by Dr. B. Wilson in 1952, is a rare, but severe soft tissue infection with up to 80% mortality [18,26,27]. It causes necrosis of muscle fascia and subcutaneous layers, spreading along poorly vascularized fascial planes while initially sparing the overlying skin. NF is classified into polymicrobial (Type I) and monomicrobial (Type II) forms [28]. Type I involves aerobic and anaerobic bacteria, leading to gas infiltration, such as gas gangrene, while type II, commonly linked to GAS and MRSA, can produce endotoxins, triggering toxic shock syndrome [15,16,28]. Necrotizing infections often present with intense, disproportionate pain and signs of systemic sepsis. Rapid progression within hours, along with symptoms, such as SE, paresthesia, and hypoesthesia from nerve injury, should raise a strong suspicion for NF [27]. It often presents systemic symptoms, such as fever, chills, hypotension, and tachycardia [15]. Severe pain disproportionate to physical findings is an early and sensitive indicator. Other signs may include skin discoloration, edema, and bullae [1,15]. Differentiating benign SE from more serious conditions is crucial, as management and outcomes differ significantly [20]. While soft tissue crepitus is commonly observed in traumatic SE, it can also indicate NF, a surgical emergency with high morbidity and mortality [1,6]. The LRINEC score, developed by Wong et al., helps differentiate NF from other soft tissue infections using six lab parameters: CRP, WBC, Hgb, sodium, creatinine, and glucose [12]. A score ≥6 raises suspicion, while >8 strongly indicates NF (92% positive predictive value, 96% negative predictive value) [1]. In this case, repeat labs at 12 h showed normal values (CRP <0.29, WBC 5.15, Na 143, glucose, Hgb 13.2, Cr 0.970), with a slight LRINEC increase to 1 due to a minor Hgb drop (13.9–13.2). NF was ruled out based on the low score and absence of clinical signs. Hydrogen peroxide irrigation has been implicated as a potential cause of benign SE in acute wound management [7,29]. In our case, the patient reported using hydrogen peroxide to clean the wound, which may have introduced oxygen into the soft tissues, leading to the development of SE. Clinicians should be aware of this phenomenon, particularly when assessing patients with atypical presentations of SE, to avoid unnecessary radical intervention. Most cases of uncomplicated traumatic SE can be managed effectively with conservative treatment, including proper wound care and antibiotics [20]. In this case, we chose a non-invasive treatment approach, guided by the patient’s history, clinical examination findings, and the LRINEC score. This evaluation confirmed a benign instance of SE rather than NF, allowing us to avoid unnecessary surgical intervention in a high-stakes diagnosis.
BSCE of the upper extremity, while rare, can closely mimic NF and should not be underestimated during initial evaluation. In cases where crepitus and soft tissue gas are present, careful clinical assessment combined with LRINEC scoring and imaging is essential to distinguish benign SE from life-threatening infections. While surgical intervention is warranted for NF, most cases of benign SE can be safely managed with conservative treatment. Clinicians must be familiar with this differential to guide appropriate management and avoid unnecessary surgery.
Clinicians should consider benign subcutaneous emphysema in the differential diagnosis when patients present with soft tissue crepitus of the upper extremity following minor trauma. In such cases, combining LRINEC scoring with imaging and serial examinations can guide appropriate management. When necrotizing fasciitis is ruled out, conservative treatment can result in excellent functional outcomes while avoiding unnecessary surgical intervention.
References
- 1. Saela S, Decilveo A, Isaac R, Patel DV. Traumatic subcutaneous emphysema of the hand/forearm: A case report. Chin J Traumatol 2022;25:395-9. [Google Scholar] [PubMed]
- 2. Das S, Shaikh O, Gaur NK, Balasubramanian G. Iatrogenic benign subcutaneous emphysema of the left upper limb. Cureus 2022;14:e22808. [Google Scholar] [PubMed]
- 3. Hiruma K, Suzuki K, Kato A, Yamaga H, Nakamura M, Inoue G, et al. Benign noninfectious subcutaneous emphysema with minor injury: A case report. Heliyon 2022;9:e12317. [Google Scholar] [PubMed]
- 4. Lo SJ, Hughes J, Armstrong A. Non-infective subcutaneous emphysema of the hand secondary to a minor webspace injury. J Hand Surg Br 2005;30:482-3. [Google Scholar] [PubMed]
- 5. Clayton-Smith MA, Sivathasan N. A case of benign subcutaneous emphysema. BMJ Case Rep 2014;2014:bcr2013202261. [Google Scholar] [PubMed]
- 6. Mack JA, Woo SL, Haase SC. Noninfectious subcutaneous emphysema of the upper extremity. J Hand Surg Am 2015;40:1233-6. [Google Scholar] [PubMed]
- 7. Rabiul Islam SM, Mamman KG, Pande KC. Benign subcutaneous emphysema of the upper limb: A case report. Malays Orthop J 2016;10:39-41. [Google Scholar] [PubMed]
- 8. Butt M, Hird GF. Surgical emphysema of the dorsum of the hand. J Hand Surg Br 1990;15:379-80. [Google Scholar] [PubMed]
- 9. Ozalay M, Akpinar S, Hersekli MA, Ozkoç G, Tandoğan RN. Benign noninfectious subcutaneous emphysema of the hand. Arch Orthop Trauma Surg 2003;123:433-5. [Google Scholar] [PubMed]
- 10. Fox A, Sheick H, Ekwobi C, Ho-Asjoe M. Benign surgical emphysema of the hand and upper limb: Gas is not always gangrene–a report of two cases. Emerg Med J 2007;24:798-9. [Google Scholar] [PubMed]
- 11. Van Der Molen AB, Birndorf M, Dzwierzynski WW, Sanger JR. Subcutaneous tissue emphysema of the hand secondary to noninfectious etiology: A report of two cases. J Hand Surg Am 1999;24:638-41. [Google Scholar] [PubMed]
- 12. Wong CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (laboratory risk indicator for necrotizing fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med 2004;32:1535-41. [Google Scholar] [PubMed]
- 13. Hoesl V, Kempa S, Prantl L, Ochsenbauer K, Hoesl J, Kehrer A, et al. The LRINEC score-an indicator for the course and prognosis of necrotizing fasciitis? J Clin Med 2022;11:3583. [Google Scholar] [PubMed]
- 14. Christen SM, Gruenert JG, Winsauer S. Benign subcutaneous emphysema: A rare and challenging entity a case report and review of the literature. Case Rep Plast Surg Hand Surg 2021;8:153-7. [Google Scholar] [PubMed]
- 15. Stevens DL, Bryant AE, Goldstein EJ. Necrotizing soft tissue infections. Infect Dis Clin North Am 2021;35:135-55. [Google Scholar] [PubMed]
- 16. Chen LL, Fasolka B, Treacy C. Necrotizing fasciitis: A comprehensive review. Nursing 2020;50:34-40. [Google Scholar] [PubMed]
- 17. Gan RK, Sanchez Martinez A, Abu Hasan MA, Castro Delgado R, Arcos González P. Point-of-care ultrasonography in diagnosing necrotizing fasciitis-a literature review. J Ultrasound 2023;26:343-53. [Google Scholar] [PubMed]
- 18. Karahan N, Oztermeli A. Subcutaneous emphysema or necrotizing fasciitis after insect bite? Trauma Case Rep 2020;29:100353. [Published correction appears in Trauma Case Rep 2023;45:100816]. [Google Scholar] [PubMed]
- 19. Onwochei VE, Kelly ME, Lyons R, Khan W, Barry KM. Benign subcutaneous emphysema: A case report with bite. Int J Surg Case Rep 2015;9:89-91. [Google Scholar] [PubMed]
- 20. Kukuruza K, Aboeed A. Subcutaneous emphysema. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 21. Molasy B, Frydrych M. Necrotizing fasciitis – two case reports and literature review. Pol Przegl Chir 2023;96:103-8. [Google Scholar] [PubMed]
- 22. Chou PY, Hsieh YH, Lin CH. Necrotizing fasciitis of the entire head and neck: Literature review and case report. Biomed J 2020;43:94-8. [Google Scholar] [PubMed]
- 23. Olsen RJ, Musser JM. Molecular pathogenesis of necrotizing fasciitis. Annu Rev Pathol 2010;5:1-31. [Google Scholar] [PubMed]
- 24. Brummelkamp WH. Tissue emphysema of the hand and fore-arm simulating gas gangrene infection, following minimal injury. Report on six cases. Arch Chir Neerl 1964;16:227-35. [Google Scholar] [PubMed]
- 25. Fowler JR, Rerko MA, Grand AG. Benign subcutaneous emphysema of the upper extremity. Orthopedics 2013;36:e1458-60. [Google Scholar] [PubMed]
- 26. Green RJ, Dafoe DC, Raffin TA. Necrotizing fasciitis. Chest 1996;110:219-29. [Google Scholar] [PubMed]
- 27. Wallace HA, Perera TB. Necrotizing fasciitis. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 28. Al Shukry S, Ommen J. Necrotizing fasciitis – report of ten cases and review of recent literature. J Med Life 2013;6:189-94. [Google Scholar] [PubMed]
- 29. De M, Stevenson J. Subcutaneous emphysema of upper limb. Emerg Med J 2001;18:522. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Necrotizing Fasciitis of the Forearm in a 68-Year-Old Patient Treated with Split-Thickness Skin Graft: A Case Report
May 1, 2026 Necrotizing Fasciitis of the Forearm in a 68-Year-Old Patient Treated with Split-Thickness Skin Graft: A Case Report February 1, 2026 Post-Traumatic Subcutaneous Emphysema of the Upper Extremity Associated with an Open Scapular Fracture: A Case Report and Review of Literature
February 1, 2026 Post-Traumatic Subcutaneous Emphysema of the Upper Extremity Associated with an Open Scapular Fracture: A Case Report and Review of Literature May 1, 2025 Induced Membrane Wrist Fusion with Ring External Fixator Assistance in a Mangled Upper Extremity: A Case Report
May 1, 2025 Induced Membrane Wrist Fusion with Ring External Fixator Assistance in a Mangled Upper Extremity: A Case Report January 10, 2024 Isolated Upper Extremity Compartment Syndrome: A Case of Rhabdomyolysis-induced Myoglobinuria and Acute Kidney Injury after Opioid Overdose
January 10, 2024 Isolated Upper Extremity Compartment Syndrome: A Case of Rhabdomyolysis-induced Myoglobinuria and Acute Kidney Injury after Opioid Overdose