
Intertrochanteric fracture fixation in patients with severe peripheral vascular disease carries a rare but devastating risk of acute limb ischemia and amputation, requiring vigilant vascular assessment and cautious traction use.
Dr. Sai Surya Dinesh Pydi, Department of Orthopaedics, Post Graduate Institute of Medical Education and Research, PGIMER Chandigarh. Email: saisuryadinesh111@gmail.com
Abstract
Introduction: Intertrochanteric (IT) femur fractures are among the most commonly encountered injuries in orthopedic practice and are typically managed successfully with internal fixation using cephalomedullary devices. Vascular complications following such procedures are rare and are most often limited to localized arterial injury or pseudoaneurysm formation. Progression to acute limb ischemia with subsequent limb loss is exceptionally uncommon, particularly in the setting of routine fracture fixation. The presence of severe peripheral vascular disease (PVD) may significantly alter this otherwise predictable clinical course.
Case Report: We report the case of a 50-year-old male with advanced PVD who sustained a right IT femur fracture following a slip and fall at home. After thorough medical optimization and multidisciplinary evaluation, the patient underwent closed reduction and internal fixation with a proximal femoral nail. Despite an initially uneventful intraoperative course, the patient developed acute-on-chronic limb ischemia in the post-operative period, characterized by progressive loss of distal perfusion and tissue viability. Imaging confirmed diffuse multilevel arterial disease with poor distal runoff. Despite prompt anticoagulation, fasciotomy, and vascular consultation, limb salvage was not possible, and the patient ultimately required staged below-knee followed by definitive above-knee amputation.
Conclusion: This case highlights a rare but catastrophic complication following IT fracture fixation in a patient with severe PVD. It underscores the critical importance of meticulous pre-operative vascular assessment, cautious use of traction during fracture reduction, early multidisciplinary involvement, and realistic perioperative counseling regarding the potential risk of acute limb ischemia and limb loss in high-risk patients.
Keywords: Intertrochanteric fracture, peripheral vascular disease, limb ischemia, traction table, amputation.
Intertrochanteric (IT) femur fractures are common injuries in older adults and are usually managed successfully with dynamic hip screws or cephalomedullary nails. Although uncommon, vascular complications after proximal femoral fixation can be catastrophic, most often involving the deep femoral artery (DFA) or its branches due to over-penetration of the medial cortex, malpositioned distal locking screws, or impingement by a displaced lesser-trochanter fragment [1,2,3]. The traction table integral to closed reduction can bring the femoral vasculature into closer proximity to the cortex and transiently reduce limb perfusion, increasing susceptibility to injury in vulnerable vessels [1]. Patients with pre-existing peripheral vascular disease (PVD) have limited perfusion reserve and impaired collateralization. Even modest intraoperative or post-operative reductions in limb blood flow may precipitate acute-on-chronic ischemia and tissue loss [2,4]. Most reported cases describe pseudoaneurysm formation or arterial laceration after fixation, typically with successful limb salvage. Progression to irreversible ischemia requiring amputation remains extremely rare. We present a case of severe PVD with an IT fracture treated by proximal femoral nailing (PFN) that evolved to non-salvageable ischemia and above-knee amputation despite timely recognition and vascular co-management. This case highlights the interplay between traction-table mechanics and advanced PVD and emphasizes the need for rigorous vascular assessment and perioperative counseling.
A 50-year-old male presented 4 days after a slip and fall at home with dyspnea, desaturation, and right-hip pain with deformity and inability to bear weight. On arrival, the patient was assessed and resuscitated according to advanced trauma life support principles. The airway and cervical spine were stabilized; breathing was supported with supplemental oxygen; circulation monitored; and a secondary survey was completed. He had a past history of pulmonary tuberculosis (completed treatment).
On examination
Airway patent, SpO2 80% on room air (maintained on 5 L/min O2 by mask), tachypneic and tachycardic but hemodynamically stable, Glasgow coma scale 15/15. The right lower limb was shortened, externally rotated, and tender over the greater trochanter. A 5 × 4 cm bluish-black discoloured patch was noted over the anterolateral aspect of the mid-leg; it was non-tender, with no local temperature changes. Active ankle and toe movements were intact. Distal pulses – anterior tibial, posterior tibial, and dorsalis pedis were absent bilaterally, and the bilateral lower limbs were cold. Radiographs revealed an unstable right IT femur fracture (Fig. 1). Chest X-ray showed increased bronchovascular markings with ill-defined upper-lobe opacity. Bilateral lower-limb Doppler demonstrated monophasic flow with parvus-tardus waveform in the popliteal artery and no flow in the anterior and posterior tibial arteries on the right. The left leg also showed monophasic flow in the common femoral artery and superficial femoral artery. Pre-operative computed tomography (CT) angiography showed atherocalcific changes in abdominal and bilateral lower limb arteries (Fig. 2).

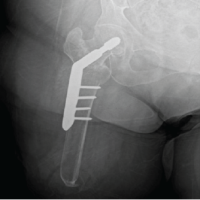
Figure 1: Pre-operative plain radiographs showing a stable intertrochanteric femur fracture of the right hip.
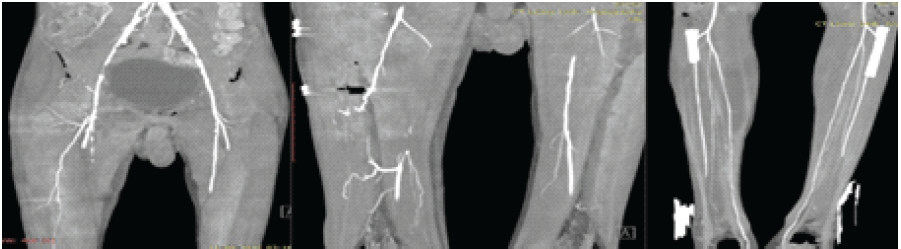
Figure 2: Pre-operative computed tomography angiography. On the right side, there is multifocal stenosis in the external iliac artery and common femoral artery, extending up to near complete occlusion in the external iliac artery, with a long segment complete stenosis of the superficial femoral artery; on the left side, there is multifocal stenosis in the external iliac artery and common femoral artery, extending up to severe stenosis in the external iliac artery.
The patient was managed in the intensive care unit with oxygen therapy, analgesics, and intravenous broad-spectrum antibiotics (cefuroxime, metronidazole, and amikacin). Skin traction was avoided due to evolving leg skin changes. Over the next few days, the discoloration enlarged (6 × 7 cm) with mottled skin, though motor and sensation initially remained intact.
After medical optimization, closed reduction and internal fixation with a proximal femoral nail were performed on day 11 post-injury (Fig. 3). Intraoperatively, there was minimal blood loss, and hemodynamics remained stable throughout.

Figure 3: Post-operative plain radiographs showing fracture fixation with a proximal femoral nail in situ.
Post-operatively, distal pulses remained absent, toe pulse oximetry was unrecordable, and the limb became progressively cold and insensate. Urgent fasciotomy revealed dusky, non-contractile muscles, indicating established ischemia (Fig. 4). CT angiography demonstrated diffuse narrowing and reduced caliber of bilateral lower-limb arteries, consistent with advanced PVD. Despite anticoagulation (systemic anticoagulation with unfractionated heparin) and vascular consultation, progressive mottling and malodor developed, necessitating below-knee amputation, followed by definitive above-knee amputation due to poor healing (Fig. 5). Recovery thereafter was uneventful, and the patient was fitted with a prosthesis during rehabilitation.
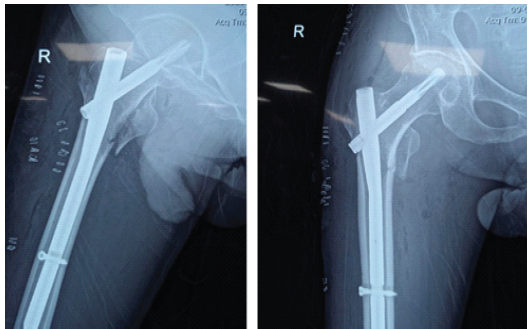
Figure 4: Clinical images depicting the course of the lesion: (a) Discoloration measuring 6 × 7 cm with mottled skin over the anterolateral aspect of the leg; (b) Fasciotomy wound showing non-contractile, necrotic muscle fibers.
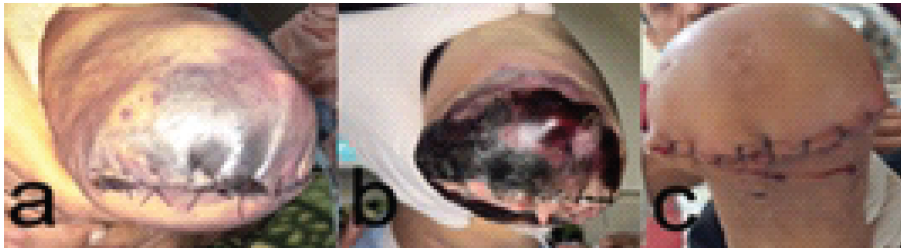
Figure 5: Clinical sequence showing progression of ischemic changes: (a) Necrotic changes in the below-knee stump; (b) Complete stump necrosis following below-knee amputation; (c) Healed above-knee amputation stump after revision surgery.
Vascular complications following IT fracture fixation are uncommon but potentially devastating, with reported incidences of 0.2–0.5% [3]. Most involve the DFA or its perforators, caused by over-penetration of the medial cortex, misplaced distal locking screws, or migration of fracture fragments, such as the lesser trochanter [5,6,7,8,9,10,11,12,13]. While the majority of published cases describe pseudoaneurysm formation or arterial laceration managed successfully with repair or embolization, our patient progressed to irreversible ischemia and amputation, an outcome rarely reported in this context. Traction-table use introduces unique vascular challenges. Longitudinal traction and adduction/internal rotation narrow the safe corridor by bringing the DFA closer to the femoral cortex, increasing the risk that drilling or distal locking may violate the vessel’s proximity [1,8]. The perineal post and sustained traction can also depress limb perfusion, exacerbating endothelial stress and predisposing to intimal damage. These dynamics explain recurring mechanisms across the literature: Over-penetration during distal locking, guide-wire or drill-bit injury, and fragment-related impingement, all of which can produce immediate bleeding or delayed pseudoaneurysm [5,6,7,9,10,11,12,13]. In the setting of PVD, even minor mechanical or hemodynamic stress may precipitate acute ischemia. Chronic atherosclerosis causes fixed arterial narrowing, calcification, and diminished collateral capacity, while endothelial dysfunction and platelet activation create a prothrombotic milieu [2,3,4,14]. Consequently, traction-related compression, hypotension, or intraoperative vessel manipulation can trigger occlusion or spasm in already compromised arteries. In addition, chronically ischemic muscle is highly susceptible to reperfusion injury, and once ischemia develops, myonecrosis advances rapidly despite early fasciotomy or anticoagulation [2,3,4]. Several prior reports describe DFA pseudoaneurysm or rupture following PFN or intramedullary fixation in elderly, vasculopathic patients, typically managed with coil embolization or surgical repair and with limb salvage [5,6,7,9,10,11,12,13,14]. In contrast, our patient, who had documented bilateral absence of pedal pulses and no distal tibial flow on pre-operative Doppler developed fulminant ischemia immediately after fixation. Despite aggressive vascular management, prompt administration of anticoagulants and unfractionated heparin within 48 h of surgery, the process was irreversible and culminated in amputation [15]. This case, therefore, represents one of the most severe endpoints documented after IT fixation and highlights how advanced PVD can transform a routine orthopedic procedure into a limb-threatening event. Practically, three key points emerge, echoing prior literature [1,2,3,4,8,9,11,12,14]. First, risk-stratify early: Patients with absent pedal pulses or monophasic Doppler signals should undergo ankle-brachial pressure index, duplex, or CT angiography, and vascular teams should be involved pre-operatively. Second, modify the reduction and fixation technique: Minimize the traction magnitude and duration, avoid extreme adduction, use guarded sleeves during drilling, and verify the screw length, especially for distal interlocking screws, where the DFA proximity is greatest. Third, maintain a low threshold for post-operative vascular imaging when pain, swelling, or skin changes occur, as prompt identification of pseudoaneurysm or thrombosis can prevent irreversible ischemia. Compared with most IT fixation–related vascular injuries, where prompt repair results in good outcomes, this case’s progression to amputation underscores the synergy between traction-table mechanics, diffuse atherosclerotic disease, and microvascular failure. It reinforces that in severe PVD, even an optimal technique may not avert ischemia, and that realistic pre-operative counseling about the small but real risk of limb loss is essential.
PVD significantly magnifies the risk of vascular compromise following IT fracture fixation. This case demonstrates that despite timely surgery and vascular management, catastrophic ischemia may still occur. Early identification of PVD, judicious traction use, and multidisciplinary perioperative care are essential to optimize outcomes and prevent limb loss. The case also emphasizes the importance of clear pre-operative counseling for patients with advanced vascular disease.
Severe PVD should be considered a major risk factor for acute limb ischemia during IT fracture fixation, and patients must be counseled regarding the rare but real possibility of limb loss.
References
- 1. Flierl MA, Stahel PF, Hak DJ, Morgan SJ, Smith WR. Traction table-related complications in orthopaedic surgery. J Am Acad Orthop Surg 2010;18:668-75. [Google Scholar] [PubMed]
- 2. Al-Rumaih M, Al-Jaber F, Batheeb N. Vascular injuries and complications in orthopedic surgery procedures. J Orthop Rep 2025;4:100435. [Google Scholar] [PubMed]
- 3. Wilson JS, Miranda A, Johnson BL, Shames ML, Back MR, Bandyk DF. Vascular injuries associated with elective orthopedic procedures. Ann Vasc Surg 2003;17:641-4. [Google Scholar] [PubMed]
- 4. Abularrage CJ, Weiswasser JM, Dezee KJ, Slidell MB, Henderson SC, Sidawy AN. Predictors of lower extremity arterial injury after total knee or total hip arthroplasty. J Vasc Surg 2008;47:803-7; discussion 807-8. [Google Scholar] [PubMed]
- 5. Yoon HK, Oh HC, Park J, Oyunbat C, Kim T. Rupture of the deep femoral artery during proximal femoral nailing following an intertrochanteric fracture: A case report. Clin Orthop Surg 2016;8:221-5. [Google Scholar] [PubMed]
- 6. Li X, Luckeroth PD, Curry EJ, Eslami MH, Leclair W. Pseudoaneurysm of the profunda femoris artery following a long anterograde intramedullary nail for an unstable intertrochanteric hip fracture: A case report and review of the literature. Eur J Orthop Surg Traumatol 2011;21:293-9. [Google Scholar] [PubMed]
- 7. Vande Voorde K, Dauwe J, Van Oost J. Late presentation of an iatrogenic pseudoaneurysm of the profunda femoris artery following intramedullary nailing. Case Rep Orthop 2018;2018:8270256. [Google Scholar] [PubMed]
- 8. Bot R, Tirla A, Cavalu SD. Vascular complications following trans-trochanteric fracture fixation: Case and literature review. Vasc Health Risk Manag. 2025;8:191. [Google Scholar] [PubMed]
- 9. Orapiriyakul W, Chewakidakarn C, Dissaneewate K, Dissaneewate P, Kritsaneephaiboon A. Silent iatrogenic pseudoaneurysm after intertrochanteric fracture fixation with proximal femoral nailing and cerclage wiring: Case report and review of literature. Eur J Orthop Surg Traumatol 2023;33:2667-81. [Google Scholar] [PubMed]
- 10. Rajaesparan K, Amin A, Arora S, Walton NP. Pseudoaneurysm of a branch of the profunda femoris artery following distal locking of an intramedullary hip nail: An unusual anatomical location. Hip Int 2008;18:231-5. [Google Scholar] [PubMed]
- 11. Piolanti N, Giuntoli M, Nucci AM, Battistini P, Lisanti M, Andreani L. Profunda femoris artery pseudoaneurysm after intramedullary fixation for a pertrochanteric hip fracture. J Orthop Case Rep 2017;7:74-7. [Google Scholar] [PubMed]
- 12. Kim BS, Kim ST, Shin S, Yu CG. Delayed pseudoaneurysm of deep femoral artery caused by migration of lesser trochanter, subsequent to an intertrochanteric fracture surgery – a case report. J Musculoskelet Trauma 2021;34:76-9. [Google Scholar] [PubMed]
- 13. Beckett NC, Haglin J, Van Schuyver P, Spangehl MJ, Kalani MA, Lyons MK, et al. Traumatic disruption of profunda femoris artery branch following treatment of an intertrochanteric hip fracture with a cephalomedullary nail. Case Rep Orthop 2024;2024:5590091. [Google Scholar] [PubMed]
- 14. Ryzewicz M, Robinson M, McConnell J, Lindeque B. Vascular injury during fixation of an intertrochanteric hip fracture in a patient with severe atherosclerosis. A case report. J Bone Joint Surg Am 2006;88:2483-6. [Google Scholar] [PubMed]
- 15. Rosenberg H, Rosenberg E, Kubelik D. Acute limb ischemia. CMAJ 2023;195:E1383. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2024 Intertrochanteric Fracture Fixation Using a Traction Table in a Patient with Ipsilateral Above-knee Amputation – A Case Report and Review of Reduction Techniques
November 1, 2024 Intertrochanteric Fracture Fixation Using a Traction Table in a Patient with Ipsilateral Above-knee Amputation – A Case Report and Review of Reduction Techniques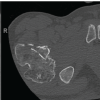 July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review
July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study
July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report