
To highlight an entrapped Tillaux fragment as a rare cause of irreducible ankle fracture–dislocation in adolescents and should be suspected when closed reduction fails.
Ameya H Velankar, Department of Orthopaedics, MGM Institute of Health Sciences, Navi-Mumbai, Maharashtra, India. E-mail: ameya_velankar@yahoo.com
Abstract
Introduction: Tillaux fractures are Salter–Harris type III injuries of the anterolateral distal tibial epiphysis seen in adolescents. Entrapment of the Tillaux fragment within the syndesmosis is rare and may lead to an irreducible ankle fracture-dislocation.
Case Report: A 13-year-old girl sustained an ankle fracture–dislocation following an external rotation injury. Imaging revealed a displaced Tillaux fracture with an associated posterior malleolus fracture. Closed reduction was unsuccessful. Open reduction revealed incarceration of the Tillaux fragment within the syndesmosis, preventing reduction of the talus. Removal and anatomical fixation of anterior and posterior malleolar fragments restored syndesmotic stability. The patient achieved full functional recovery.
Conclusion: In adolescents, failure of closed reduction of ankle fracture–dislocation should raise a suspicion of an entrapped Tillaux fragment. Computed tomography evaluation and anatomical fixation are essential for restoring joint congruency and preventing long-term complications.
Keywords: Ankle fracture–dislocation, Tillaux fracture, posterior malleolus fracture, syndesmotic injury.
Tillaux fractures are avulsion injuries of the anterolateral distal tibial epiphysis that occur in adolescents and are classified as Salter–Harris type III fractures [1]. They typically result from a supination-external rotation mechanism, where the relatively strong anteroinferior tibiofibular ligament (AITFL) avulses the anterolateral epiphysis, which is the last part of the distal tibial physis to fuse [2,3].
These fractures are clinically significant due to their association with syndesmotic injury. Although Tillaux fractures are well described, incarceration of the fragment within the syndesmosis, causing an irreducible ankle fracture–dislocation, is extremely rare. We report such a case and discuss the mechanism, diagnostic challenges, and management considerations.
A 13-year-old girl presented with severe pain and deformity of the ankle following a twisting injury sustained while playing football. Clinical examination revealed an externally rotated, swollen ankle with restricted movements. Neurovascular status was intact.
Radiographs demonstrated a posterior ankle dislocation with a posterior malleolus fracture and suspected anterolateral tibial involvement (Fig. 1).
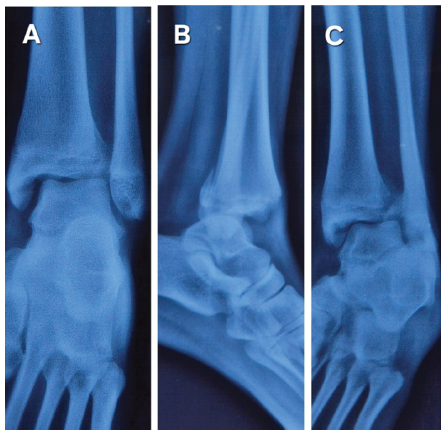
Figure 1: Initial ankle X-rays (a) antero-posterior view, (b) lateral view, (c) mortise view showing a double shadow at the antero-lateral corner of the distal tibia.
A gentle attempt at closed reduction failed. Computed tomography (CT) scan revealed a displaced Tillaux fracture with incarceration of the fragment within the syndesmosis, associated with a posterior malleolus fracture and persistent posterior talar dislocation (Figs. 2 and 3).
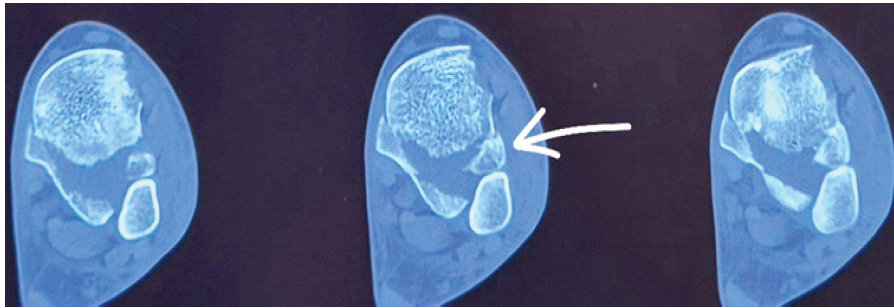
Figure 2: Axial computed tomography scan of the ankle showing the Tillaux fragment entrapped in the syndesmosis (white arrow), also showing a 360° view of the ankle.

Figure 3: Three-dimensional computed tomography scan of the ankle joint.
Closed reduction under general anesthesia was again unsuccessful, and open reduction was undertaken. Intraoperatively, the Tillaux fragment was found to be entrapped within the syndesmotic joint, mechanically blocking reduction of the talus (Fig. 4).
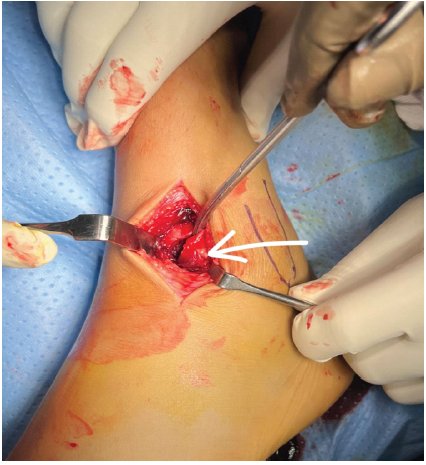
Figure 4: Incarcerated tillaux fragment in the syndesmosis (white arrow).
After disengagement and anatomical repositioning of the fragment, the ankle and syndesmosis were easily reduced. The posterior malleolus (Fig. 5) and Tillaux fragment (Fig. 6) were fixed using cannulated cancellous screws.
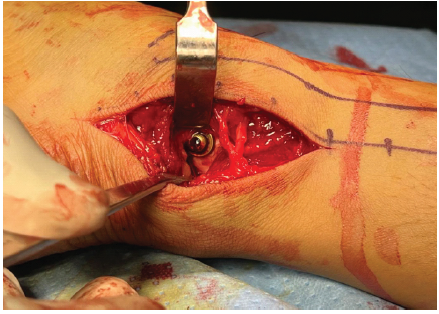
Figure 5: Posterior malleolus fixed with a 4 mm cannulated cancellous screw and washer.

Figure 6: Tillaux fragment fixed with a 4 mm cannulated cancellous screw and washer.
Post-operative imaging confirmed anatomical reduction and syndesmotic stability (Fig. 7).
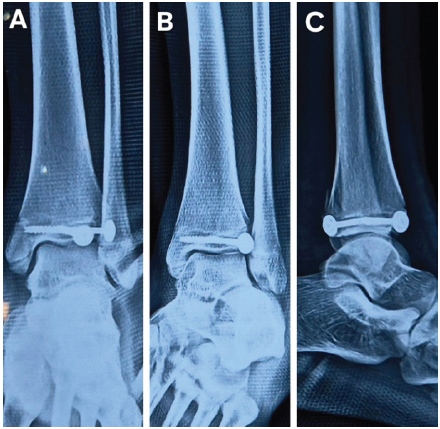
Figure 7: Immediate post-operative X-ray, (a) antero-posterior view, (b) lateral view, (c) mortise view.
Immobilization was maintained for 3 weeks, followed by progressive range-of-motion exercises. The patient remained non-weight-bearing for 6 weeks and returned to full weight-bearing by 10 weeks. At final follow-up, the patient demonstrated ankle dorsiflexion of 18°, plantarflexion of 45°, inversion of 32°, and eversion of 18°, comparable to the contralateral side, with no pain or instability (Fig. 8).
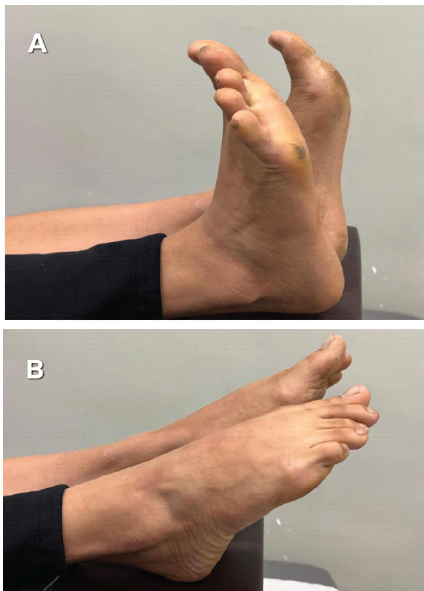
Figure 8: Clinical images of the ankle movements at 1 year postoperatively.
The American Orthopaedic Foot and Ankle score hindfoot score was 95/100, showing an excellent post-operative functional outcome. Implant removal was performed at 1 year without complications (Fig. 9).
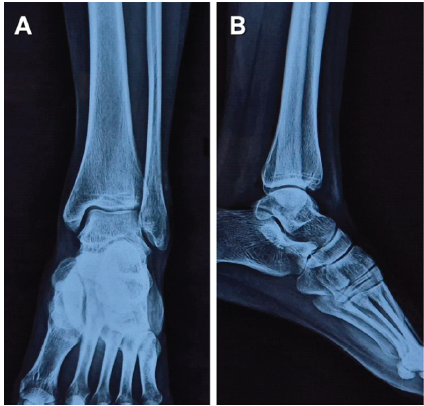
Figure 9: Ankle X-ray post-implant removal at 1 year.
The Tillaux fracture is a distal tibial epiphyseal injury and is the second most common physeal fracture seen in adolescents, accounting for approximately 17.8% of cases [4]. Skeletally immature athletes are particularly susceptible, as physeal ankle fractures constitute nearly 40% of sports-related injuries in children [5]. The lateral tibial epiphysis is the last portion of the distal tibial physis to fuse; therefore, during late adolescence, an external rotation injury results in avulsion of the AITFL, which is stronger than the partially fused epiphysis, leading to fracture of the anterolateral tibia. Since physeal closure has already begun at this stage, growth arrest following Tillaux fractures is uncommon [6].
These fractures may be overlooked if not carefully evaluated, as anteroposterior and lateral radiographs can appear normal when the fracture is undisplaced. A mortise or internal rotation view of the ankle improves visualization of the anterolateral tibial fragment, which is often obscured by the fibula on standard anteroposterior views [2]. Associated injuries, including posterior and medial malleolar fractures, may coexist and should be carefully assessed, as they influence syndesmotic stability and treatment planning.
The distal tibiofibular syndesmosis functions as a ligamentous ring, with the AITFL attached to the anterior malleolus and the posteroinferior tibiofibular ligament attached to the posterior malleolus [7]. In our case, the young girl was playing football, and her foot rolled over it, leading to a severe twisting injury, causing a supination and external rotation force, which was responsible for the disruption of the syndesmosis ring from the anterior to the posterior malleolus. As most of the distal tibial epiphysis had already fused, only a small anterolateral fragment fractured and became entrapped within the syndesmosis, mechanically preventing ankle reduction by reversing the injury mechanism by dorsiflexion and inversion of the foot.
CT is crucial for diagnosing such injuries, which may be missed on plain radiographs, and aids in fracture classification and surgical planning. It is a 360° approach for the evaluation of fracture geometry and fragment fixation in ankle fractures, where all four malleoli are evaluated [8]. Closed reduction with traction and internal rotation, along with direct pressure over the anterior fragment, may be attempted once under general anesthesia; however, fractures with more than 2 mm displacement or syndesmotic widening require open reduction and internal fixation [1,9]. Fixation of the posterior malleolus is particularly important for restoring syndesmotic stability. The rationale behind fixing both the Tillaux and posterior malleolus is a direct fixation principle described by Dr. Stefan Rammelt as a 360° approach, where direct fixation of the anterior and posterior malleolus is better than surrogate or indirect fixation by the syndesmotic screw [10].
Early diagnosis and appropriate management of distal tibial epiphyseal fractures with associated syndesmotic injury are essential to prevent complications such as malunion, non-union, and post-traumatic ankle arthritis, as reported in cases of delayed diagnosis [5,11]. Adequate post-operative follow-up and rehabilitation are necessary to ensure functional recovery and return to pre-injury activity levels. Many cases of Tillaux fracture have been reported in the literature; however, none of them had a Tillaux fragment entrapped in the syndesmosis, causing irreducible ankle dislocation. Only one similar case has been reported in the literature; however, that case did not involve ankle dislocation, the Tillaux fragment was smaller, fixation was achieved using a single Steinmann pin, and the posterior malleolus fracture was undisplaced. It did not require fixation [12].
Entrapment of a displaced Tillaux fragment is a rare cause of irreducible ankle fracture–dislocation in adolescents. Failure of closed reduction should prompt CT evaluation. Anatomical reduction and fixation of associated malleolar fractures are essential to restore syndesmotic stability and achieve good functional outcomes.
In adolescents with ankle fracture–dislocation, an irreducible joint should raise suspicion of an entrapped Tillaux fragment. Early CT assessment and anatomical fixation are crucial to prevent long-term ankle instability and arthritis.
References
- 1. Habusta SF, Ponnarasu S, Mabrouk A, Griffin EE. Tillaux fracture. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 2. Bouzid YB, Berrada MS. About a rare ankle injury in adults: Case report of a Tillaux fracture in adult. Trauma Case Rep 2023;46:100869. [Google Scholar] [PubMed]
- 3. Birnie MFN, Van Schilt KL, Sanders FR, Kloen P, Schepers T. Anterior inferior tibiofibular ligament avulsion fractures in operatively treated ankle fractures: A retrospective analysis. Arch Orthop Trauma Surg 2019;139:787-93. [Google Scholar] [PubMed]
- 4. Peterson CA, Peterson HA. Analysis of the incidence of injuries to the epiphyseal growth plate. J Trauma 1972;12:275-81. [Google Scholar] [PubMed]
- 5. Santos-Pereira R, Aleixo C, Oliveira M, Sarmento A, Santos M. Painful nonunion after missed juvenile Tillaux fracture in an athlete – case report and description of a new fixation technique. J Orthop Case Rep 2018;8:7-10. [Google Scholar] [PubMed]
- 6. Barmada A, Gaynor T, Mubarak SJ. Premature physeal closure following distal tibia physeal fractures: A new radiographic predictor. J Pediatr Orthop 2003;23:733-9. [Google Scholar] [PubMed]
- 7. Ebraheim NA, Taser F, Shafiq Q, Yeasting RA. Anatomical evaluation and clinical importance of the tibiofibular syndesmosis ligaments. Surg Radiol Anat 2006;28:142-9. [Google Scholar] [PubMed]
- 8. Nenopoulos A, Beslikas T, Gigis I, Sayegh F, Christoforidis I, Hatzokos I. The role of CT in diagnosis and treatment of distal tibial fractures with intra-articular involvement in children. Injury 2015;46:2177-80. [Google Scholar] [PubMed]
- 9. Al-Ashhab ME, Mohamed AA. Treatment for displaced tillaux fractures in adolescent age group. Foot Ankle Surg 2019;36:295-8. [Google Scholar] [PubMed]
- 10. Rammelt S, Gonzalez Salas JI, Marx C. Syndesmotic ankle fractures. Fuß Sprunggelenk 2024;22:94-111. [Google Scholar] [PubMed]
- 11. Zatti G, D’Angelo F, Giughello A. Delayed diagnosis and treatment of Tillaux fracture-a case report. Acta Orthop Scand 2000;71:327-9. [Google Scholar] [PubMed]
- 12. Steinlauf SD, Stricker SJ, Hulen CA. Juvenile Tillaux fracture simulating syndesmosis separation: A case report. Foot Ankle Int 1998;19:332-5. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 December 10, 2023 How we do it? Trimalleolar Fractures: Posterolateral Approach for Fixing the Syndesmotic Ligament, Posterior Malleolus, and Fibula
December 10, 2023 How we do it? Trimalleolar Fractures: Posterolateral Approach for Fixing the Syndesmotic Ligament, Posterior Malleolus, and Fibula December 1, 2024 Enchondroma Protuberans of the Hand: A Rare Cartilaginous Tumor
December 1, 2024 Enchondroma Protuberans of the Hand: A Rare Cartilaginous Tumor March 2, 2019 Chronic Systemic Metal Ion Toxicity from Wear on a Revised Cobalt-chromium Trunnion
March 2, 2019 Chronic Systemic Metal Ion Toxicity from Wear on a Revised Cobalt-chromium Trunnion October 12, 2013 Tophus of the Pubis Bone: A Case Report
October 12, 2013 Tophus of the Pubis Bone: A Case Report