
Skeletal traction through a distal femoral traction pin attached to the fracture table provides reliable intraoperative control of length and rotation for cephalomedullary nailing in lower-limb amputees when standard skin traction is inadequate.
Dr. Kishan C. Trivedi, College of Osteopathic Medicine, Michigan State University, Michigan, USA. E-mail: kishanctrivedi@gmail.com
Abstract
Introduction: Femoral fracture fixation in lower-limb amputees is challenging due to limited limb purchase, altered biomechanics, and sparse guidance. We describe an intraoperative skeletal-traction technique to facilitate cephalomedullary nailing (CMN).
Case Report: Two amputee patients with extracapsular proximal femur fractures underwent CMN. Under biplanar fluoroscopy, a 5-mm distal femoral traction pin was placed through the residual limb and secured to the traction boot to restore length, correct alignment, and permit controlled reduction.
Results: Patient 1 (65-year-old female; prior left below-knee amputation, contralateral above-knee amputation) achieved an acceptable reduction and implant position; she died on post-operative day 3 from cardiopulmonary arrest. Patient 2 (77-year-old male; prior right above-knee amputation) achieved anatomic reduction with the nail tip proximal to the traction pin; the pin was removed at the case end. At 13 months, his outcome remained satisfactory; he later required contralateral amputation for ischemia.
Conclusion: Intraoperative skeletal traction through a distal femoral pin offers reliable control of length and rotation during CMN in amputees and may provide superior stump control to skin traction. Careful pin placement is essential to mitigate neurovascular risk. This approach appears feasible for both above- and below-knee amputees; larger series are needed to define indications and long-term outcomes.
Keywords: Cephalomedullary nailing, intraoperative skeletal traction, distal femoral traction pin, intertrochanteric fracture, basicervical femoral neck fracture, lower limb amputation
Amputation, often resulting from severe trauma and vascular disease, presents unique challenges in orthopedic management. With the aging population and rising prevalence of conditions such as diabetes, the number of individuals requiring limb amputation is anticipated to increase. Lower limb amputees are at heightened risk of fragility fractures and osteoporosis due to decreased bone density in the hip and residual limb stump [1]. Another concern is the development of disuse osteopenia, which also results in decreased bone mineral density due to the lack of mechanical stress and normal weight-bearing activity on the bone. While such fractures are relatively uncommon in this population, their incidence is expected to rise with advancing age [2,3].
The surgical management of fractures in lower limb amputees is particularly complex due to the absence of standardized protocols and limited research [4]. One possible treatment is the use of a cephalomedullary nail (CMN), which has shown the greatest effectiveness in treating femoral neck and intertrochanteric fractures [5]. CMN placement is commonly done using either the InterTAN with proximal femoral nail anti-rotation (PFNA) or the Gamma3 nail. Both are effective for treatment; however, research indicates the InterTAN PFNA nail is superior in terms of reducing complications and improving outcomes [6]. Regardless of the nail type, CMN represents a viable treatment option for these fractures, especially in amputated patients, providing stable fixation while minimizing disruption to compromised soft tissues – a significant advantage in this patient cohort [7]. This stability promotes early weight-bearing and mobilization, thereby reducing the risk of secondary complications [8]. Nonetheless, complications such as malalignment and non-union with CMN are infrequent but possible [9].
Intraoperative traction may play a crucial role in CMN procedures for amputees by facilitating precise nail insertion and ensuring proper alignment of the implant. The fracture table, invented in 1913 by Dr. George Hawley, serves as the framework for intraoperative traction, which allows for suspension and immobilization of the lower extremities to provide reliable support and traction in the treatment of fractures [10]. In cases of lower extremity fractures, intraoperative traction is provided primarily with the use of skeletal traction, which involves placement of a pin through the bone, serving as the base of the pulley system, and is attached to the fracture table. Current literature predominantly addresses CMN in non-amputee cases, underscoring the need for further investigation into intraoperative traction techniques tailored specifically for amputated patients. In this case series, we discuss how we utilized intraoperative traction to successfully achieve fracture reduction in amputee patients with extracapsular proximal femur fractures.
Case Report 1
Patient 1 was a 65-year-old female who presented to the emergency department with left hip pain status post fall out of bed. She had been non-ambulatory for 6 years. Past medical history was significant for stroke, peripheral arterial disease status post multiple stents, left below-knee amputation, right above-knee amputation, chronic obstructive pulmonary disease, insulin-dependent type 2 diabetes, and congestive heart failure (CHF).
Clinical findings
Physical examination demonstrated a prior left below-knee amputation with an intact stump. Motor and sensory functions were grossly intact throughout. There was a limited knee range of motion. Positive log roll of the left lower extremity.
Diagnostic assessment
X-rays and computed tomography (CT) of the left hip demonstrated an acute, stable intertrochanteric femur fracture with multiple calcified vessels and prior below-knee amputation (Fig. 1).
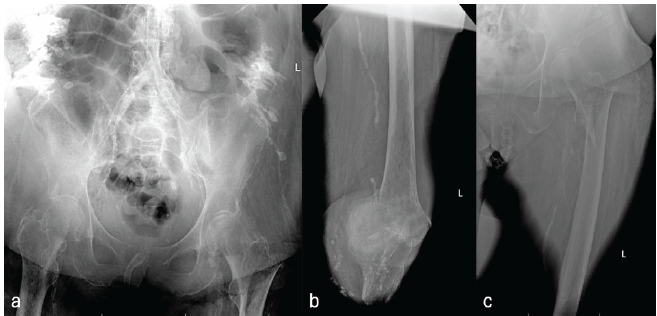
Figure 1: (a-c) Patient 1 – Stable left intertrochanteric femur fracture with calcified vessels.
Therapeutic intervention
Surgery was indicated due to her intractable pain. A short antegrade intramedullary femur nail was chosen (Stryker Gamma 4). Distal femoral traction was required to restore the length of the fracture, given her prior below-knee amputation. The patient was positioned supine on the Hana table. A 5.0 mm distal femoral traction pin was placed under the guidance of biplanar fluoroscopy. A small incision was made on the medial aspect of the left stump, and the pin was then placed through the distal femur. A second poke hole incision was then made laterally to accept the exiting pin. The entry and exit points of the skeletal traction pin were then wrapped with Kerlix, tied to the traction boot, and the extremity was placed in in-line traction. The fracture was reduced. The remainder of the procedure was carried out in the standard fashion.
Follow-up and outcomes
Final radiographs demonstrated acceptable fracture alignment with appropriately positioned hardware (Fig. 2). She unfortunately went into cardiopulmonary arrest on post-operative day 3 and expired.
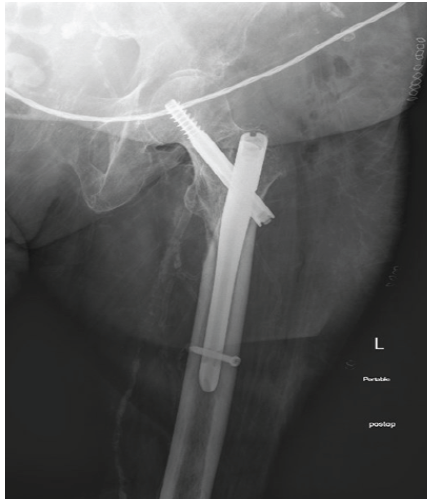
Figure 2: Patient 1 – Fixation of left intertrochanteric femur fracture post intraoperative traction.
Cardiopulmonary arrest on post-operative day 3 was felt unlikely to be directly attributable to the operative fixation or traction-pin technique, given the patient’s substantial baseline cardiopulmonary and vascular comorbidity burden (including prior cerebrovascular accident, peripheral artery disease status post-multiple stents, left below-knee amputation (BKA), right above-knee amputation, chronic obstructive pulmonary disease, insulin-dependent type 2 diabetes mellitus, and CHF); early post-operative mortality after geriatric hip fracture is frequently driven by patient factors such as age, American Society of Anesthesiologists status, and comorbid disease [11].
Case Report 2
Patient 2 is a 77-year-old male who presented to the emergency department with right hip pain status post fall. He had two falls within 1 week, 5 days, and 3 days before presentation. Both falls occurred when he got out of bed and fell on his right side. His primary complaint was right hip pain. He denied pain elsewhere. Past medical history was significant for coronary artery disease, chronic obstructive pulmonary disease, type 2 diabetes, hypertension, hyperlipidemia, peripheral vascular disease, and right above-knee amputation for ischemia. He ambulated well with a prosthetic, but otherwise did not require additional ambulatory assistive devices. Social history was significant for a history of smoking, approximately 50 pack years.
Clinical findings
Physical examination demonstrated a prior right above-knee amputation with an intact stump. Motor and sensory were grossly intact throughout. Positive log roll of the right lower extremity.
Diagnostic assessment
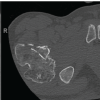
X-rays and CT of the right hip demonstrated an acute, comminuted basicervical femoral neck fracture with calcified vessels and prior above-knee amputation (Fig. 3).
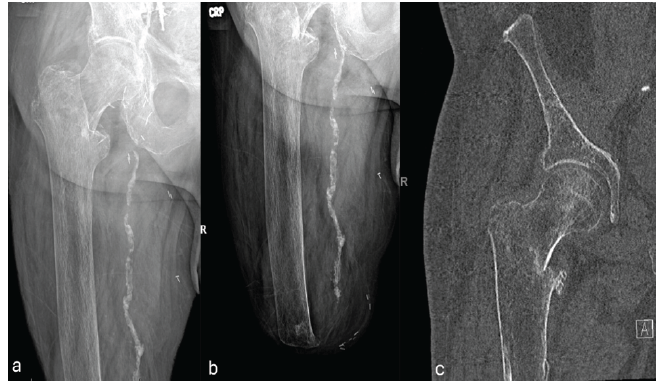
Figure 3: (a and c) Patient 2 – Comminuted basic cervical right femoral neck fracture with calcified vessels.
Therapeutic intervention
Surgery was indicated due to his ambulatory status and overall functionality. An antegrade intramedullary femur nail was chosen (Stryker Gamma 3). Distal femoral traction was required to restore the length of the fracture, given his prior above-knee amputation. The patient was positioned supine on a standard radiolucent fracture table. The left lower extremity was positioned utilizing the well leg holder. Attention was turned to the right lower extremity. A 5.0 mm distal femoral traction pin was placed under the guidance of biplanar fluoroscopy. A small incision was made on the lateral aspect of the right stump, and the pin was then placed through the posterior aspect of the distal femur. A second poke hole incision was then made medially to accept the exiting pin. The entry and exit points of the skeletal traction pin were then wrapped with Kerlix, tied to the traction boot, and the extremity was placed in in-line traction (Fig. 4a). The fracture was reduced, and the remainder of the operation was carried out similarly to the previously described procedure for Patient 1. Intraoperative fluoroscopy (Fig. 4b and c) demonstrated the distal tip of the intramedullary nail ending just proximal to the distal femoral traction pin. The traction pin was removed at the conclusion of the procedure.
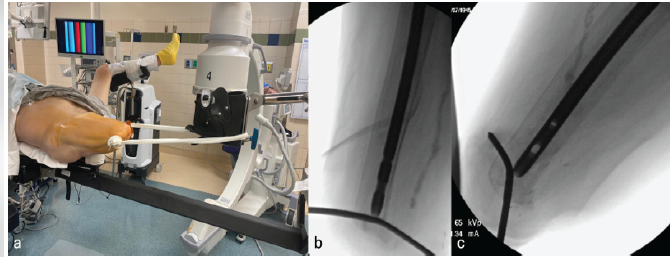
Figure 4: (a) Intraoperative traction; (b and c) intramedullary nail tip just proximal to the traction pin.
Follow-up and outcomes
Final radiographs demonstrated anatomic alignment of the fracture with appropriately positioned hardware (Fig. 5).
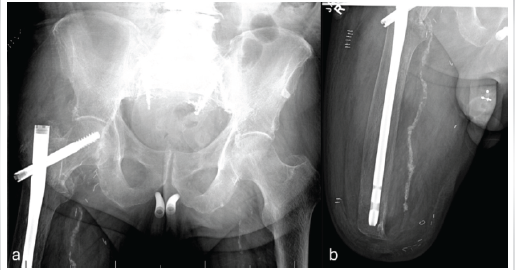
Figure 5: Patient 2 – Fixation of right femoral neck fracture post intraoperative traction.
He is now 13 months post-operative and doing well regarding his hip. He unfortunately required left above-knee amputation due to ischemia at 12 months postoperatively and is now only minimally ambulatory.
The use of intraoperative traction for cephalomedullary nailing (CMN) in amputated patients is a nuanced approach aimed at optimizing the stability and alignment of the femur in a challenging scenario. Surgical management of femur fractures in this population presents important considerations due to reduced soft tissue integrity, stability, and altered biomechanics. In addition, positioning and fracture reduction difficulties arise due to the absence of some or all of the leg/foot. This case series underlines that intraoperative traction in such scenarios can be used as a method to enhance surgical outcomes.
Both fractures in this series were extracapsular proximal femur fractures (intertrochanteric and basicervical). Arthroplasty is primarily indicated for displaced intracapsular femoral neck fractures, whereas extracapsular fracture patterns are typically managed with internal fixation (e.g., CMN) to preserve the native hip joint [12,13]. Pre-operative CT angiography is not routinely obtained for hip fractures in the absence of clinical concern for acute vascular compromise. Given the patients’ severe vascular calcification and amputated stumps, traction was applied through a distal femoral pin placed at the most distal feasible aspect of the residual limb under biplanar fluoroscopy. Available anatomic and clinical data suggest distal femoral traction pin placement has a low risk of major vascular injury when performed within recommended safe zones, and temporary traction pins have low pin-site infection rates – particularly when removed immediately after the procedure, as in both cases [14,15].
Utilizing intraoperative traction served several critical purposes. Intraoperative traction allowed for ideal stabilization and alignment of the nail by providing controlled traction, which was instrumental in fracture reduction. The proper alignment of the nail can reduce complications such as non-union and nail migration.
The approach used for these patients involved in-line traction with the use of a skeleton traction pin that was anchored to a traction boot. Although this method was appropriate for these patients, one study found other methods of intraoperative traction to also be effective. Anjum and McNicholas utilized skin traction on the 22-year-old BKA stump with an elastic bandage while the patient was on the fracture table. This was then secured by the traction cord to maintain optimal traction [16]. In our experience, we feel that skeletal traction provides better control of the stump, despite a small risk of damage to the surrounding neurovasculature.
In our case, intraoperative traction contributed to the successful fracture reduction and CMN placement. In addition, the procedure was well tolerated with no signs of immediate or later complications associated with CMN placement and traction. Despite the patient’s successful recovery, it is still important to acknowledge the risk of complications as well as limitations to the procedure. Complications include infection, skin injury, and neurovascular compromise. The generalizability of our findings may be limited by the anatomical and physiological variations of each patient. Factors including bone density, soft-tissue integrity, and overall patient health may influence the use of intraoperative traction. Therefore, attention to patient-centered factors and a tailored approach to each case is necessary.
A conservative (non-operative) approach for displaced hip fractures is generally reserved for patients with end-of-life goals of care or prohibitive perioperative risk, as it is associated with very high short-term mortality and substantial pain-related morbidity. In a cohort of very frail elderly hip-fracture patients managed nonoperatively after shared decision-making, mortality was 87% at 30 days and 99% at 1 year [17]. Accordingly, even in high-risk surgical candidates, operative fixation is commonly recommended as a palliative intervention to improve comfort, facilitate nursing care, and potentially allow earlier mobilization when aligned with patient goals [18].
Intraoperative traction for CMN in amputation patients is a valuable approach that can aid in achieving optimal fracture reduction and stability. Our experience highlights the importance of meticulous planning as well as technique refinement in cases that include amputated patients. Further studies, including larger case series, are warranted to better define indications, outcomes, and long-term implications of the use of intraoperative traction for CMN in amputated patients.
In amputee patients with proximal femur fractures, a distal femoral skeletal traction pin connected to the fracture table can provide stable intraoperative control of the residual limb, enabling safe and reproducible CMN when conventional skin traction is insufficient or unreliable.
References
- 1. Haleem S, Yousaf S, Hamid T, Nagappa S, Parker MJ. Characteristics and outcomes of hip fractures in lower limb amputees. Injury 2021;52:914-7. [Google Scholar] [PubMed]
- 2. Milella FM, Paolocci M, Persi E, Mezzoprete R. Total hip arthroplasty (THA) in a patient with subcapital femoral neck fracture and ipsilateral above-knee amputation: A case report. Trauma Case Rep 2024;51:101027. [Google Scholar] [PubMed]
- 3. Kim DS, Shon HC, Kim YM, Choi ES, Park KJ, Im SH. Postoperative mortality and the associated factors for senile hip fracture patients. J Korean Orthop Assoc 2008;43:488-94. [Google Scholar] [PubMed]
- 4. Huguet J, Mariscal G, Balfagón A, Mayorga D, Ulldemolins P, Guillot A, et al. Management and outcomes of hip fractures in lower limb amputees: A case series. Indian J Orthop 2023;57:1063-7. [Google Scholar] [PubMed]
- 5. Bali K, Gahlot N, Aggarwal S, Goni V. Cephalomedullary fixation for femoral neck/intertrochanteric and ipsilateral shaft fractures: Surgical tips and pitfalls. Chin J Traumatol 2013;16:40-5. [Google Scholar] [PubMed]
- 6. Yang F, Li X, Zhao L, Yang Q. Dual-screw versus single-screw cephalomedullary nails for intertrochanteric femoral fractures: A systematic review and meta-analysis. J Orthop Surg Res 2023;18:607. [Google Scholar] [PubMed]
- 7. Ricci WM, Gallagher B, Haidukewych GJ. Intramedullary nailing of femoral shaft fractures: Current concepts. J Am Acad Orthop Surg 2009;17:296-305. [Google Scholar] [PubMed]
- 8. Dekhne MS, Thomas HM, Haider T, Mortensen S, Rodriguez EK, Weaver MJ, et al. Treatment and outcomes of basicervical femoral neck fractures: A systematic review. J Orthop Surg (Hong Kong) 2021;29:23094990211003344 , p2-5. [Google Scholar] [PubMed]
- 9. Ricci WM, Bellabarba C, Lewis R, Evanoff B, Herscovici D, Dipasquale T, et al. Angular malalignment after intramedullary nailing of femoral shaft fractures. J Orthop Trauma 2001;15:90-5. [Google Scholar] [PubMed]
- 10. Hawley GW. Fracture orthopedic table. JAMA 1913;60:1850-1. [Google Scholar] [PubMed]
- 11. Canbeyli ID, Çırpar M, Oktaş B, Çoban M. Analysis of factors among 30-day and 1-year mortality rates in patients with borderline stable-unstable intertrochanteric hip fracture. Acta Orthop Traumatol Turc 2021;55:16-21. [Google Scholar] [PubMed]
- 12. Switzer JA, O’Connor MI. AAOS management of hip fractures in older adults evidence-based clinical practice guideline. J Am Acad Orthop Surg 2022;30:e1297-301. [Google Scholar] [PubMed]
- 13. Yoo JI, Cha Y, Kwak J, Kim HY, Choy WS. Review on basicervical femoral neck fracture: Definition, treatments, and failures. Hip Pelvis 2020;32:170-81. [Google Scholar] [PubMed]
- 14. Kwon JY, Johnson CE, Appleton P, Rodriguez EK. Lateral femoral traction pin entry: Risk to the femoral artery and other medial neurovascular structures. J Orthop Surg Res 2010;5:4. [Google Scholar] [PubMed]
- 15. Austin DC, Donegan D, Mehta S. Low complication rates associated with the application of lower extremity traction pins. J Orthop Trauma 2015;29:e259-65. [Google Scholar] [PubMed]
- 16. Anjum SN, McNicholas MJ. Innovative method of traction on fracture table in femoral neck fracture fixation in a below knee amputee. Injury Extra 2006;37:277-8. [Google Scholar] [PubMed]
- 17. Wijnen HH, Schmitz PP, Es-Safraouy H, Roovers LA, Taekema DG, Van Susante JL. Nonoperative management of hip fractures in very frail elderly patients may lead to a predictable short survival as part of advance care planning. Acta Orthop 2021;92:728-32. [Google Scholar] [PubMed]
- 18. Sullivan NM, Blake LE, George M, Mears SC. Palliative care in the hip fracture patient. Geriatr Orthop Surg Rehabil 2019;10:2151459319849801 , p2-6. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review
July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study
July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report
June 1, 2026 Early Mechanical Dissociation of Helical Blade-Barrel Interface in Proximal Femoral Nail: A Case Report