
The MIPPO technique in the treatment of humerus shaft fractures has shown the procedure to be safe and effective with minimal soft-tissue injury and no major complications.
Dr. Priti Ranjan Sinha, Department of Orthopedics, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India. E-mail: drpritiranjansinha@gmail.com
Abstract
Introduction: Conventional open reduction and internal fixation of the humeral shaft often has a high chance of non-union and delayed union, because of primary healing. Furthermore, a shaft humerus fracture can be managed by conservative means. However, the problem of conservative management is stiffness of joints and the possibility of delayed union of fractures. Minimally invasive percutaneous plate osteosynthesis (MIPPO) utilizes the principles of both conservative and surgical management. Healing is through secondary healing, as in conservative management, while maintaining the principles of fixation and early mobilization of joints. The plane utilized for the anterior bridge plate of the humerus is a safe plane without any major neurovascular structures crossing it. We aimed to investigate the safety, feasibility, and advantages of MIPPO via an anterior approach in the treatment of humeral shaft fractures.
Materials and Methods: Between 2023 and 2025, 13 adult humeral fractures were treated using a minimally invasive anterior bridge plating approach, followed by fixation with a locking compression plate, to evaluate the functional and radiological outcomes of this technique.
Results: A total of 13 patients were included in the study. At the 1-year post-operative follow-up, no cases of infection or nerve damage were reported (0%). Only 1 (07.7%) patient had developed neuropraxia, which recovered. Shoulder function was excellent in 11 cases (84.6%) and good in the remaining 2 (15.4%) cases on the University of California-Los Angeles score. Elbow function was excellent in 9 (69.2%) cases, good in 2 (13.4%) cases, and fair in 2 (13.4%) cases on the Mayo elbow performance score.
Conclusion: No cases of iatrogenic nerve palsy occurred through MIPPO. This approach is easy, feasible, and has better functional results. It can be used as an alternative for the treatment of extra-articular fractures of the middle and distal thirds of the humerus.
Keywords: Humeral shaft fractures, distal third, minimally invasive percutaneous plate osteosynthesis, anteromedial, neurovascular injury, road traffic accident.
Fracture of the humeral shaft is common, accounts for approximately 3% of all orthopedic injuries, and results in a significant burden to society from lost productivity and wages. Complications can include nerve and blood vessel damage (especially the radial nerve), malunion (poor alignment), and non-union (non-healing) [1,2,3].
The conflict between the need for absolute anatomical reduction and, at the same time, the desire for soft-tissue preservation has been going on for a long time. Not only solid healing, but also immediate and continuous function of the limb is now a leading goal. However, precise reduction and absolute stable fixation has its biological price [4].
There has been evidence to show the superiority of biological fixation over a stable mechanical fixation [5]. This led to the development and improvement in the techniques of biological fixation for fractures, and also the development of stabilization systems that help in achieving a biological fixation [6,7].
Open reduction with internal fixation is a common treatment method. However, these methods involve great trauma and a risk of iatrogenic radial nerve injury of 5.1–31.3%, and there are high chances of non-union and delayed union [8,9].
The minimally invasive percutaneous plate osteosynthesis (MIPPO) technique is reported as a satisfactory procedure for the treatment of humeral shaft fractures by the anterior approach by several authors. MIPPO is emerging as an effective alternative.
In the treatment of humeral shaft fractures, three surgical approaches, namely, the anterior approach, anterolateral approach, and posterior approach, are commonly used. Each has its advantages and disadvantages.
We hypothesize that a minimally invasive anterior bridge plating approach for internal fixation of middle and distal third extraarticular humeral fractures is feasible, poses minimal risk of neurovascular injury, and can be effectively used to manage these fractures while allowing assessment of their proximity to adjacent neurovascular structures.
One of the advantages is the long working length of the anterior bridge plate technique. Working length is the distance between the nearest screws on either side of a fracture when a plate is used for fixation. It determines the stiffness and flexibility of the plate–bone construct. Long working length helps in more flexibility and promotes secondary bone healing (callus formation). Short working length helps in more rigidity and a higher risk of stress concentration and implant failure. Working length is important in bridge plating, minimally invasive plate osteosynthesis, and comminuted fractures [10,11].
Operative management
The patient was positioned supine on a radiolucent table with the elbow in mild flexion. Screw position, fracture site, and incision sites were marked (Fig. 1a and b).
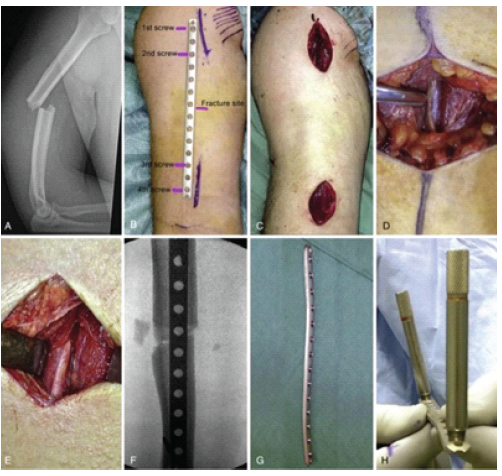
Figure 1: (a) Proximal and distal incisions for minimally invasive percutaneous plate osteosynthesis. (b) The brachialis muscle covers the distal half of the anterior humeral surface, through which the plate is advanced and the detached anterior deltoid insertion
(white arrow), to facilitate both plate advancement and positioning (Cadaver dissection). (c) The threaded drill guide is engaged to the locking plate to help with positioning.
A proximal deltopectoral incision was made using the biceps groove and pectoralis tendon as landmarks, exposing the proximal diaphysis lateral to the biceps tendon. A distal midline incision was made 1–2 cm proximal to the antecubital crease and extended proximally (Fig. 1c and d).
The interval between the biceps and brachialis was developed; the biceps was retracted medially, and the lateral antebrachial cutaneous nerve was identified and protected (Fig. 1e). The brachialis was split longitudinally, and the forearm was maintained in supination to protect the radial nerve.
Fracture reduction was achieved under fluoroscopy, ensuring acceptable alignment (<20° anterior angulation, <30° varus/valgus, <3 cm shortening). A submuscular extraperiosteal tunnel was created connecting both incisions using an MIPPO elevator (Fig. 1c).
Without radial nerve exploration, a locking compression plate was inserted (Fig. 1f). The proximal plate was fixed with one unlocked screw and contoured as needed (Fig. 1g and h). Additional locked screws were placed proximally, followed by distal fixation after confirming alignment.
Fracture compression was applied to reduce distraction, and rotational alignment was checked against the contralateral limb.
Cadaveric incision and plate placement are shown in Fig. 2, and intraoperative plate placement with C-arm guidance is shown in Fig. 3.

Figure 2: The incision of the proximal and distal, and intraoperative C-arm image intensifier placement of the humerus plate.
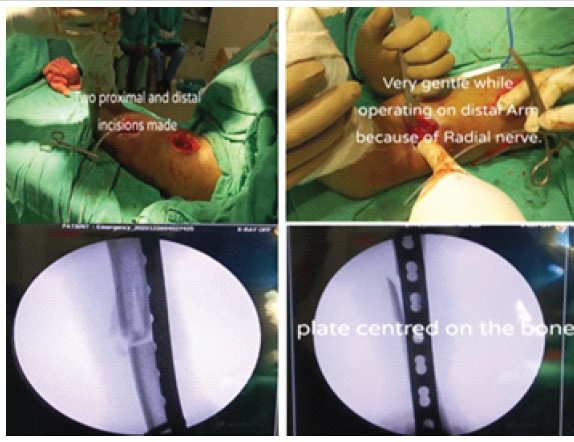
Figure 3: Case 1 – (a) Pre-operative, (b) Post-operative, (c) Function after 1 month of operation.
A total of 13 patients were selected for the study. There were 7 males and 6 females. The study protocol was approved by the institutional ethics committee, and written informed consent was obtained from all patients before inclusion in the study. All patients were treated with minimally invasive anterior bridge locking compressive plate fixation.
The inclusion criteria were as follows: (1) Diagnosis of unilateral closed humeral shaft fracture by imaging examination; (2) no neurovascular injury; and (3) patient consent to undergo surgery.
The exclusion criteria were as follows: (1) Pathological fracture; (2) associated nerve injury; (3) open fracture: Gustilo and Anderson type 3 open fracture; (4) history of mental illness or cognitive impairment; or (5) severe systemic disease resulting in an inability to tolerate surgery; (6) injury severity score >16.
Post-operative care
A sling was used for comfort for the first 2 weeks postoperatively. Active and assisted range-of-motion exercises of the shoulder and elbow were initiated immediately without restriction and were gradually increased, with emphasis on achieving full elbow extension. Minor functional limitations were maintained until radiographic evidence of bridging was observed, and unrestricted activity was typically resumed at 4–6 months.
The disability of arm, shoulder, and hand score was used to evaluate post-operative recovery. The shoulder and elbow function was assessed using the University of California at Los Angeles shoulder rating scale and Mayo elbow performance score (MEPS), respectively.
A total of 13 patients were included in this study, which were described in Table 1. Out of which 2 cases are described as Case 1 (Fig. 4, 5, 6) and Case 2 (Fig. 7, 8, 9). A total of 7 were male (53.8%), and 6 were female (46.2%). Out of 13 patients, 9 cases (69.2%) had injury in their dominant arm, and 4 cases (30.8%) had injury in their non-dominant arm.
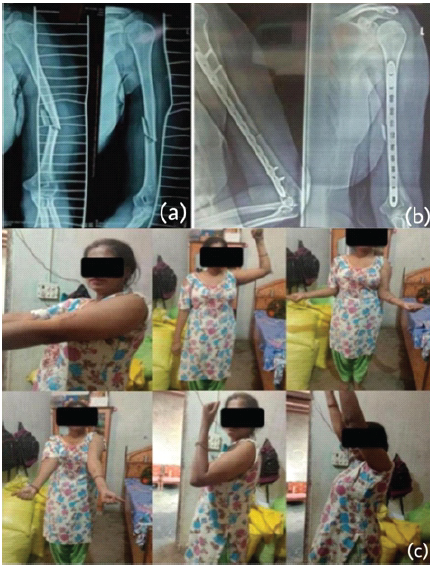
Figure 4: Case 1 – (a) At 1 year of follow-up, (b) At 2 years of follow-up, (c) After implant removal.
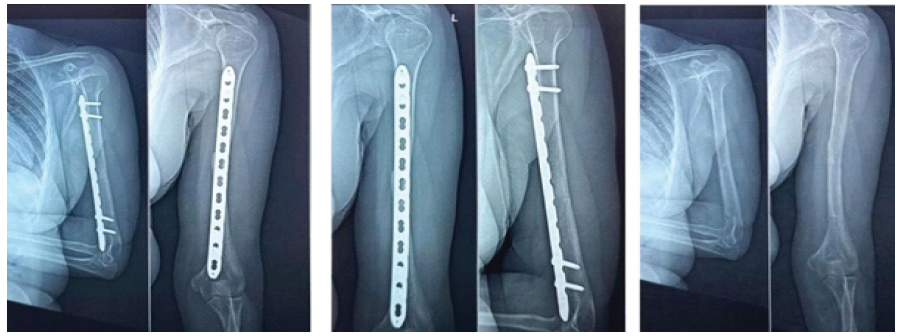
Figure 5: Case 1 – Function at 2 years of follow-up.
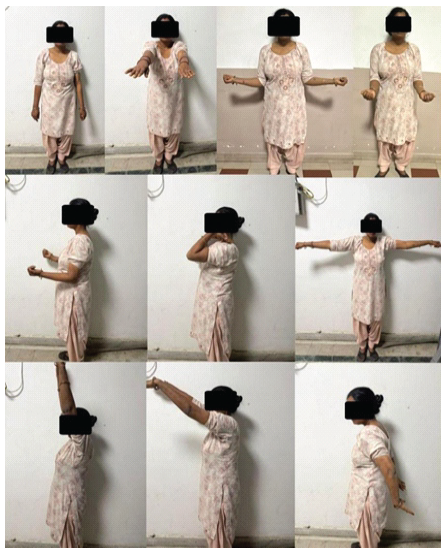
Figure 6: Case 1 – Function at 2 years of follow-up.
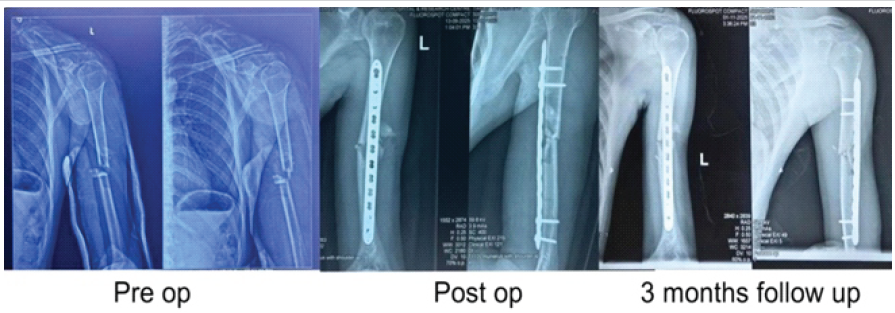
Figure 7: Case 2 – (a) Pre-operative, (b) Post-operative, (c) 3 months’ follow-up.
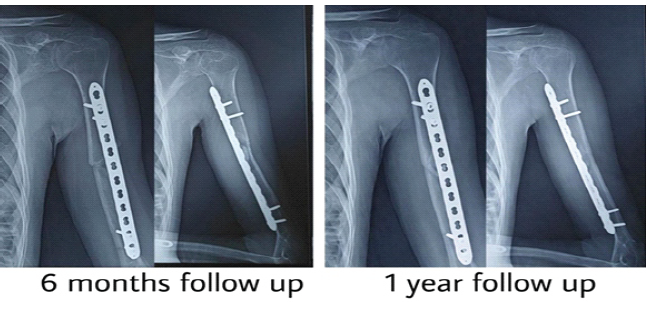
Figure 8: Case 2 – (a) 6 months’ follow-up, (b) 1 year follow-up.

Figure 9: Case 2 – (a) Small surgical scar mark, (b) Function at 1 year of follow-up.
Road traffic accident was the most common mode of injury, being reported by 10 cases (76.9%); the rest sustained injury following a fall on an outstretched hand, 2 (15.4%) cases, and direct trauma, 1 (07.7%) case. Mechanism of injury shown in Table no 2.
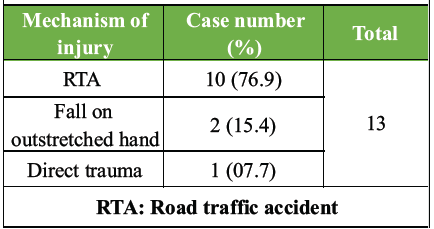
Table 2: Mechanism of injury
The mean follow-up of our cases was 12 months. Union was observed at a mean period of 12.9 weeks (range: 10–20 weeks). In 2 cases, where there was scanty callus at 12 weeks, which was kept under masterly observation, and these patients showed good union at 20 weeks. We accepted up to 5° of varus/valgus angulation intraoperatively and on following these patients, in 10 (76.9%) cases, of the cases the angulation had remodeled to correct alignment. In the remaining 3 cases, 2 had 3° of varus, and 1 had 5° of valgus.
Some degree of malunion of the humeral shaft fracture is acceptable because the shoulder function is compensated for by the wide range of motion of the glenohumoral joint. Klenerman reported that acceptable deformity of the humerus includes anterior angulation <20, varus or valgus <30, and shortening <2–3 cm [12].
At the 1-year postoperative follow-up, with no cases (0%) of infections. One patient (07.7%) had developed neuropraxia, which eventually recovered. Final evaluation showed full neurological recovery. Shoulder function was excellent in 11 (84.6%) cases and good in the remaining 2 cases (15.4%) on the University of California-Los Angeles score, as shown in Table 3. Elbow function was excellent in 9 (69.2%) cases, good in 2 (13.4%) cases, and fair in 2 (13.4%) cases on the MEPS, as shown in Table 4.
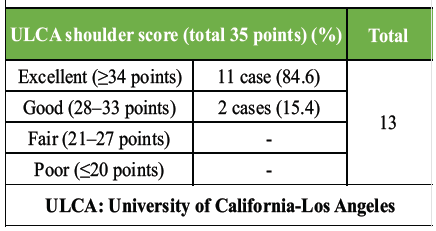
Table 3: ULCA shoulder score
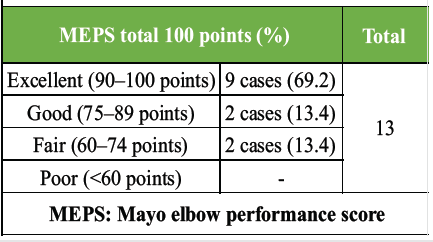
Table 4: MEPS score
The present study demonstrates that MIPPO using an anterior bridge plating technique provides reliable union and favorable functional outcomes in humeral shaft fractures. All fractures in our series united at a mean of 12.9 weeks, which is comparable to previously reported outcomes with biological fixation techniques [13,14,15]. The consistent union observed may be attributed to preservation of the fracture hematoma and periosteal blood supply, key principles underlying secondary bone healing [13].
Iatrogenic radial nerve injury remains a major concern in operative fixation of humeral shaft fractures, with reported rates ranging from 5.1% to 31.3% in open techniques [8,9]. In contrast, no permanent nerve palsy was observed in our series, and only one case of transient neuropraxia (7.7%) recovered completely. The anterior approach avoids direct manipulation of the radial nerve and utilizes a relatively safe anatomical plane, which likely explains the low incidence of nerve-related complications, consistent with previous reports [14,15].
Functional outcomes in this study were favorable, with 84.6% of patients achieving excellent shoulder function and the majority demonstrating excellent-to-good elbow scores. These results are comparable with existing literature and reflect the advantage of minimal soft-tissue disruption, which facilitates early mobilization and preservation of joint function [14,15].
Minor angular malalignment observed in a few cases did not adversely affect functional outcomes and showed remodeling over time. This aligns with previously described acceptable limits of deformity in humeral shaft fractures, owing to compensatory shoulder motion [12]. Furthermore, the use of a long working length in bridge plating likely contributed to optimal construct flexibility, promoting callus formation and reducing implant-related complications [16].
The absence of infection and implant failure in our study further supports the biological and minimally invasive nature of this technique. However, limitations include the small sample size and lack of a control group. Larger comparative studies are necessary to further validate these findings.
The minimally invasive anterior bridge plate approach for the treatment of fractures of the middle and distal thirds of the humerus has some limitations. This clinical therapeutic study included a small number of cases, and this MIPPO technique is not suitable for proximal humeral fractures; there is not enough space proximally for screw fixation, resulting in a smaller amount of humerus available for purchase than in the lateral or anterior-lateral MIPPO approach, which allows the entire humerus/head to be available for purchase.
The limitation of the study was that we did not have a control group for comparison or another group treated with some other technique of humeral diaphyseal fracture fixation. A larger multicenter study with control groups will help us to arrive at a definitive conclusion.
The present study involving the MIPPO technique in the treatment of recent humerus shaft fractures has shown the procedure to be safe and effective with minimal soft-tissue injury and no major complications. Fracture union is augmented by the process of bridging callus, which progresses to complete union. This retrospective case series substantiates the superiority of the MIPPO technique as an effective method of shaft humerus fracture fixation with fewer disadvantages and shorter fracture union time and fewer incidences of radial nerve palsies.
Minimally invasive anterior bridge plating (MIPPO) for humeral shaft fractures is a safe and effective technique that preserves soft tissue biology, minimizes the risk of radial nerve injury, and allows early mobilization with excellent functional outcomes. It is a reliable alternative for extra-articular fractures of the middle and distal humerus.
References
- 1. Epps CH Jr., Grant RE. Fractures of the shaft of the humerus. In: Rockwood CA Jr., Green DP, Bucholz RW, editors. Rockwood and Green’s Fractures in Adults. 3rd ed. Philadelphia, PA: Lippincott Williams and Williams; 1991. [Google Scholar] [PubMed]
- 2. Praemer MA, Furner S, Price DP. Musculoskeletal Conditions in the United States. Park Ridge, IL: American Academy of Orthopaedic Surgeons; 1992. [Google Scholar] [PubMed]
- 3. Tsai CH, Fong YC, Chen YH, Hsu CJ, Chang CH, Hsu HC. The epidemiology of traumatic humeral shaft fractures in Taiwan. Int Orthop 2009;33:463-7. [Google Scholar] [PubMed]
- 4. Wagner M, Frigg R. Concepts of fracture fixation. In: AO Manual of Fracture Management: Internal Fixators. Chapters 1, 2. Germany: Thieme; 2006. [Google Scholar] [PubMed]
- 5. Baumgaertel F, Buhl M, Rahn BA. Fracture healing in biological plate osteosynthesis. Injury 1998;29 Suppl 3:C3 6. [Google Scholar] [PubMed]
- 6. Dickson KF, Munz JW. Locked plating: Biomechanics and biology. Tech Orthop 2007;22:E1-6. [Google Scholar] [PubMed]
- 7. Wagner M, Frenk A, Frigg R. Locked plating: Biomechanics and biology, and locked plating: Clinical indications. Tech Orthop 2007;22:209-18. [Google Scholar] [PubMed]
- 8. Claessen FM, Peters RM, Verbeek DO, Helfet DL, Ring D. Factors associated with radial nerve palsy after operative treatment of diaphyseal humeral shaft fractures. J Shoulder Elbow Surg 2015;24:e307-11. [Google Scholar] [PubMed]
- 9. An Z, Zeng B, He X, Chen Q, Hu S. Plating osteosynthesis of mid-distal humeral shaft fractures: Minimally invasive versus conventional open reduction technique. Int Orthop 2010;34:131-5. [Google Scholar] [PubMed]
- 10. Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: Choosing a new balance between stability and biology. Injury 2002;33 Suppl 2:B1-4. [Google Scholar] [PubMed]
- 11. Azar FM, Beaty JH, Canale ST, editors. Campbell’s Operative Orthopaedics. 13th ed. Philadelphia, PA: Elsevier; 2017. p. 3065. [Google Scholar] [PubMed]
- 12. Klenerman L. Fractures of the shaft of the humerus. J Bone Joint Surg Br 1966;48:105-11. [Google Scholar] [PubMed]
- 13. Claes LE, Heigele CA. Magnitudes of local stress and strain along bony surfaces predict the course and type of fracture healing. J Biomech 1999;32:255-66. [Google Scholar] [PubMed]
- 14. Livani B, Belangero WD. Bridging plate osteosynthesis of humeral shaft fractures. Injury 2004;35:587-95. [Google Scholar] [PubMed]
- 15. Apivatthakakul T, Arpornchayanon O, Bavornratanavech S. Minimally invasive plate osteosynthesis (MIPO) of the humeral shaft fracture. Is it possible? A cadaveric study and preliminary report. Injury 2005;36:530-8. [Google Scholar] [PubMed]
- 16. Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury 2003;34 Suppl 2:B63-76. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Tips for Accurate Beath Pin Length Measurement While Using an Arthroscopic Jig to Avoid Neurovascular Injury Due to Over Penetration (Hit-Pat’s Method)
April 1, 2026 Tips for Accurate Beath Pin Length Measurement While Using an Arthroscopic Jig to Avoid Neurovascular Injury Due to Over Penetration (Hit-Pat’s Method) October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures
October 1, 2025 Comparative Study of Minimally Invasive Plate Osteosynthesis Versus Open Reduction and Internal Fixation in the Treatment of Distal Fibular Fractures September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report
September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report April 1, 2025 Minimally Invasive Posterior Plating for Comminuted Middle to Distal One-Third Humeral Shaft Fractures: A Case Report
April 1, 2025 Minimally Invasive Posterior Plating for Comminuted Middle to Distal One-Third Humeral Shaft Fractures: A Case Report