
This case series can throw light on the varied injury patterns and reduction maneuvers in an obturator type of anterior hip dislocation.
Dr. Gopikrishnan Rajeev, Department of Orthopaedics, Government Medical College, Thiruvananthapuram, Kerala, India. E-mail: gopikrajeev@gmail.com
Abstract
Introduction: Anterior hip dislocations are rare injuries, usually produced by forceful abduction and external rotation of the hip. Two variants of anterior hip dislocation are described, based on the position of the femoral head-iliac and obturator variants.
Case Report: Four cases of the obturator type of anterior hip dislocations are described in this series. All the cases were reduced by closed reduction maneuvers. Post-reduction plain radiographs were taken to confirm reduction. Post-reduction computed tomography was also done to look for any associated injuries, such as femoral head fractures or acetabular labral injuries. All 4 cases in this series were reduced by closed reduction maneuvers consisting of axial traction followed by flexion, abduction and internal rotation.
Conclusion: Closed reduction techniques described in literature for anterior hip dislocations could be reliably reproduced in the clinical setting with good results. Long-term follow-up of these cases is essential as they are associated with a gamut of devastating complications.
Keywords: Hip dislocation, obturator variant, closed reduction, osteonecrosis.
Hip dislocations are the result of high-energy trauma, usually motor vehicle accidents. It is usually associated with other injuries, most commonly involving the ipsilateral knee. Systemic injuries have been documented in 40–75% of hip dislocation patients [1]. The position of the femur and the direction of the traumatic force determines the type of dislocation as well as any associated injuries to the femoral head or acetabulum [2]. An axially directed force on an adducted hip produces a posterior dislocation, with the injured limb being shortened, internally rotated, and adducted [1,2]. Anterior hip dislocations are rare injuries forming <10% of all hip dislocations [1]. The injured extremity is in an attitude of flexion, abduction and external rotation. Anterior dislocations are usually produced by forceful abduction and external rotation of the hip. Two types of anterior dislocations have been characterized based on the position occupied by the dislocated femoral head- iliac and obturator types. In obturator dislocations, higher degree of hip flexion at the time of injury forces the femoral head below the pubofemoral ligament to lie on the pubis or anterior to the obturator foramen [2,3]. A more extended hip forces the femoral head to dislocate anterosuperiorly between the iliofemoral and pubofemoral ligaments, leading to an iliac dislocation [3].
Hip dislocations are associated with serious long-term complications and must be reduced as soon as possible. Osteonecrosis, post-traumatic osteoarthritis, heterotopic ossification (HO) and sciatic nerve injury are the widely recognized complications of hip dislocations. Anterior hip dislocations, being a rare injury, there is a paucity of literature available regarding its management, prognosis and long term outcomes. This study includes 4 cases of traumatic obturator hip dislocations and describes the mechanism of injury as well as the reduction maneuvers.
Case 1
A 17-year-old male presented to the orthopedic emergency after sustaining a fall while running down a slope. He presented with severe pain in his right hip, with the hip fixed in an attitude of abduction and external rotation. He presented within an hour of the traumatic event. Plain radiographs of the pelvis showed a traumatic obturator type of anterior hip dislocation (Fig. 1).
Closed reduction was attempted in the emergency room (ER) under procedural sedation. Axial traction was initially given on the injured limb. An assistant applied a laterally directed force on the femoral shaft. Initially, flexion, abduction, and internal rotation were done, but the deformity persisted. In the second attempt, the external rotation was initially exaggerated, followed by traction and internal rotation. This maneuver resulted in the correction of deformity and equalization of limb lengths. No neurovascular deficit was present after reduction. After attaining congruous reduction, computed tomography (CT) was done to look for any associated lesions. The CT films were found to be unremarkable with no associated osteochondral lesions or pelvic ring disruptions. The patient was kept non-weight-bearing for a period of 6 weeks, hip range of motion was started at 3 weeks with partial weight bearing initiated at 6 weeks (Figs. 1 and 2).
Case 2
A 61-year-old male presented following a high-velocity motor vehicle accident. The patient had fallen from a scooter and presented with complete inability to move his right lower limb. The right lower limb was kept in a vicious attitude of flexion, abduction, and external rotation. The patient was referred from a peripheral hospital and presented about 4 h after the trauma with X-rays showing an anteroinferior, obturator type dislocation of the right hip (Fig. 3). No associated systemic injuries were present. A closed reduction was attempted under procedural sedation and adequate muscle relaxation in the ER. An audible jerk was heard after a maneuver of axial traction followed by flexion, abduction and internal rotation. An assistant provided a laterally directed thrust on the proximal femoral shaft. Post-reduction CT screening of the hip was done and showed no osteochondral lesions, intra articular loose fragments or pelvic ring injuries. The patient was kept non-weight-bearing for a period of 6 weeks. The patient, however; did not report for further follow-up.
Case 3
A 63-year-old female presented to the ER after falling from a height of around 6 feet. She clearly recalls landing directly on her knee. She sustained direct trauma to the knee while the hip was flexed and abducted (Fig. 4). She arrives at our Centre within 2 h of the fall.
An hour later, closed reduction was attempted under general anesthesia with good muscle relaxation. Again, we utilized the technique of exaggerating the external rotation deformity before giving traction and internal rotation. In patients where vigorous reduction maneuvers carry the risk of iatrogenic fractures, this technical pearl can be put to use to achieve reduction without the use of brute force (Figs. 5 and 6).
Case 4
A 51-year-old male presented to the ER following a motor vehicle collision where he was riding a scooter. He was referred from a peripheral center and presented to us about 5 h after the index event. He complains of severe pain in his right hip. The patient is unable to move his right lower limb which is kept fixed in flexion, abduction and external rotation (Fig. 7). Closed reduction was attempted in the emergency. The flexion abduction internal rotation maneuver; however, failed to correct the deformity. Under adequate analgesia and muscle relaxants, a second attempt was made. This time, with axial traction, the external rotation was exaggerated, following which the traction was released. This was followed by traction and internal rotation, which led to correction of the deformity. It was noted that, with initial exaggeration of the external rotation, vastly improved the ease of reduction. The post-reduction X-rays showed congruous reduction with no associated injuries evident on CT films (Figs. 8 and 9). Weight bearing was started at 6 weeks.
Anterior hip dislocations account for 7–13% of all hip dislocations [4]. The direction of hip dislocation is determined by the attitude of the hip at the time of impact. Anterior hip dislocations usually result from a high velocity trauma with direct impact on the medial side of the flexed knee. This impact on a hip kept in flexion, abduction and external rotation causes the femoral head to be extricated anteriorly from the acetabulum [5]. The ligamentous structures of the anterior hip capsule provide a strong restraint to anterior dislocations [6]. The femoral head comes out through the anterior capsule beneath the pubofemoral ligament and comes to rest anterior to the obturator foramen [7].
Like posterior dislocations, early and expeditious reduction is the panacea in anterior hip dislocations, improving prognosis and long-term outcomes. Timely reduction has been shown to reduce the risk of femoral head osteonecrosis and irreversible chondral damage in addition to improving patient comfort [8]. Delay in reduction also places the nearby neurovascular structures at risk. Cases of external iliac artery occlusion secondary to unreduced anterior hip dislocation have been reported [4]. However, there is no consensus regarding the critical interval before which anterior dislocations have to be reduced. However, it is unanimously agreed that early, emergent reduction improves the medium and long term prognosis of the femoral head. In a retrospective study of 127 cases, the incidence of avascular necrosis was found to be significantly higher in hips reduced after a delay of more than 6 h [8]. However, literature regarding the long term course of anterior hip dislocations are sparse.
The reduction maneuvers should be done with good muscle relaxation. Repetitive, vigorous reduction attempts must be avoided as it can aggravate the associated soft tissue and chondral damage. The reduction maneuver consists of gentle axial traction, followed by flexion and internal rotation of the hip. However, in 3 out of 4 cases in this series, the hip could not be reduced with this maneuver (Table 1). Irreducible anterior hip dislocations can be attributed to the antero inferior incarceration of the femoral head by the strong ligaments of the anterior hip capsule. This can be overcome by exaggerating the external rotation deformity, which relieves the femoral head from its soft tissue restraints. Once the femoral head is freed in this manner, it can easily reduced into the acetabulum with traction, flexion and internal rotation.
After successful reduction, a CT study of the hip was done in all the cases to look for associated injuries to the femoral head, acetabular rim and any intra articular loose bodies. None of the cases in our series had an associated injury to the femoral head or acetabulum. Some studies have shown that associated femoral head fractures resulted in significantly higher incidence of post-traumatic arthritis and poor long term function [9,10]. Acetabular fractures were reported in 27–30% of anterior hip dislocations, which were mostly rim fractures or anterior wall fractures [4,11].
While all the cases in our series could be reduced successfully by closed means, irreducible dislocations, large acetabular fractures affecting stability, and entrapped fragments in the joint are indications for open reduction.
Long-term outcomes of anterior hip dislocations are promising. In a study from Harborview Medical Center, only 1 in 16 anterior hip dislocations on long-term follow-up required conversion to total hip arthroplasty [6].
Avascular necrosis and HO have also been reported following anterior hip dislocations. Widely varying rates of avascular necrosis have been reported in the literature [4,9,10]. There is a higher risk of HO after anterior hip dislocations which may cause debilitating stiffness necessitating resection [6]. The incidence of HO seems to be more in cases requiring open reduction and in iliac dislocation variants [6].
This case series characterizes the injury mechanisms, mode of presentation, associated injuries, and initial reduction techniques of obturator variant hip dislocations at a tertiary-level trauma center. All cases in our series were successfully reduced by closed methods with no associated acetabular or femoral head fractures. However the scope of the study is limited to a large extent due to the absence of long-term follow-up. Most of the patients failed to turn up for follow-up after 3 months resulting in lack of long term clinical and radiological data.
Anterior hip dislocations are quite amenable to closed reduction techniques. Timely reduction can alleviate the incidence of long-term complications. As seen in a couple of cases in this series, exaggerating the external rotation can aid in the reduction of initially irreducible dislocations. Open reduction of anterior dislocations need technically competent hands, which may not always be at hand. Timely closed reduction can increase patient comfort and prevent long-term sequelae.
References
- 1. Newhouse KE. Campbell’s operative orthopaedics. 7th ed. Yale J Biol Med 1987;60:495. [Google Scholar] [PubMed]
- 2. Pringle JH. Traumatic dislocation at the hip joint. An experimental study on the cadaver. Glasgow Med J 1943;139:25-40. [Google Scholar] [PubMed]
- 3. Erb RE, Steele JR, Nance EP Jr., Edwards JR. Traumatic anterior dislocation of the hip: Spectrum of plain film and CT findings. AJR Am J Roentgenol 1995;165:1215-9. [Google Scholar] [PubMed]
- 4. Bastian JD, Turina M, Siebenrock KA, Keel MJ. Long-term outcome after traumatic anterior dislocation of the hip. Arch Orthop Trauma Surg 2011;131:1273-8. [Google Scholar] [PubMed]
- 5. Zengui ZF, El Adaoui O, Fargouch M, Adnane O, El Andaloussi Y, Fadili M. Traumatic obturator dislocation of the hip joint: About 2 cases and review of the literature. Int J Surg Case Rep 2022;93:106983. [Google Scholar] [PubMed]
- 6. Wojahn RD, Kleweno CP, Agel J, Githens MF. Anterior hip dislocation: Characterization of a rare injury and predictors of functional outcome. Injury 2021;52:2327-32. [Google Scholar] [PubMed]
- 7. Jensen BV, Sandermann J. Traumatic anterior dislocation of the hip. Case report. Arch Orthop Trauma Surg 1989;108:327-8. [Google Scholar] [PubMed]
- 8. Hougaard K, Thomsen PB. Coxarthrosis following traumatic posterior dislocation of the hip. J Bone Joint Surg Am 1987;69:679-83. [Google Scholar] [PubMed]
- 9. Epstein HC. Traumatic dislocation of the hip. Clin Orthop Relat Res 1973;92:116-41. [Google Scholar] [PubMed]
- 10. DeLee JC, Evans JA, Thomas J. Anterior dislocation of the hip and associated femoral-head fractures. J Bone Joint Surg Am 1980;62:960-4. [Google Scholar] [PubMed]
- 11. Dussault RG, Beauregard G, Fauteaux P, Laurin C, Boisjoly A. Femoral head defect following anterior hip dislocation. Radiology 1980;135:627-9. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Inferior Hip Dislocation – A Case Report and Literature Review
August 1, 2025 Inferior Hip Dislocation – A Case Report and Literature Review May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report
May 1, 2026 Atypical Hip Pain due to Intra-articular Osteoid Osteoma Treated by Surgical Hip Dislocation in an Adolescent: Case Report April 1, 2026 Multifocal Osteonecrosis in the Hips and Shoulders Bilaterally after Severe COVID-19 Infection Misdiagnosed as Fibromyalgia: A Case Report
April 1, 2026 Multifocal Osteonecrosis in the Hips and Shoulders Bilaterally after Severe COVID-19 Infection Misdiagnosed as Fibromyalgia: A Case Report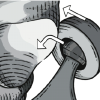 April 1, 2026 Dislocation and Iatrogenic Dissociation of Bipolar Hip Hemiarthroplasty: A Case Series and Literature Review
April 1, 2026 Dislocation and Iatrogenic Dissociation of Bipolar Hip Hemiarthroplasty: A Case Series and Literature Review