
Slipped capital femoral epiphysis can occur as a rare late complication after pediatric femoral neck fracture fixation despite initial union. Residual coxa vara, altered biomechanics, and possible physeal stress may predispose to delayed slip, highlighting the importance of restoring normal proximal femoral alignment and maintaining long-term follow-up.
Dr. Mansha Madan, Department of Anaesthesiology, Fellowship in Pain and Palliative Medicine, Adesh Institute of Medical Sciences and Research, Bathinda, Punjab, India. E-mail: drmansha.madan@gmail.com
Abstract
Introduction: Slipped capital femoral epiphysis (SCFE) occurring after surgical treatment of femoral neck fractures in children is exceedingly rare. Awareness of this complication is essential because delayed diagnosis may result in progressive deformity and significant morbidity.
Case Report: We report the case of a 9-year-old female child who sustained a right-sided femoral neck fracture (Delbet Type III) and a left subtrochanteric femoral fracture following a fall from height. She underwent closed reduction and internal fixation of the femoral neck fracture with cannulated cancellous screws and open reduction with plating for the subtrochanteric fracture. Although fracture union was achieved, residual coxa vara deformity was noted. Fifteen months postoperatively, she developed hip pain and limping. Radiographs revealed SCFE with retained implants in situ. Endocrine evaluation was normal. Revision surgery was advised; however, the patient was lost to follow-up.
Conclusion: SCFE developing after femoral neck fracture fixation in children is a rare but important complication. Residual deformity, altered proximal femoral biomechanics, and possible physeal stress may predispose to slip. Anatomical reduction, stable fixation, and careful post-operative management are crucial to minimize this risk.
Keywords: Slipped capital femoral epiphysis, pediatric femoral neck fracture, coxa vara, rare complication, case report.
Femoral neck fractures in children are uncommon injuries but are associated with a high incidence of complications, including avascular necrosis, non-union, and malunion [1]. Slipped capital femoral epiphysis (SCFE) occurring after treatment of such fractures is exceptionally rare, with only a few cases reported in the literature [2]. The adequacy of fracture reduction and the timing of intervention following injury play a critical role in determining the clinical and radiological outcomes of femoral neck fractures in the pediatric population [3]. This case report highlights a delayed presentation of SCFE following surgical fixation of a femoral neck fracture in a child without identifiable endocrine abnormalities. To the best of our knowledge, this represents one of the few reported cases of delayed SCFE following surgically treated pediatric femoral neck fracture with residual coxa vara deformity.
A 9-year-old female child presented after a fall from height with a right-sided femoral neck fracture and a left-sided subtrochanteric femoral fracture. The femoral neck fracture was classified as Delbet Type III. The child was of average build, with a body mass index of 21. Pre-operative laboratory investigations, including hormonal and endocrine evaluations, were within normal limits.
The patient underwent surgical management under general anesthesia. Closed reduction and internal fixation of the right femoral neck fracture were performed using two partially threaded cannulated cancellous screws. The left subtrochanteric fracture was treated with open reduction and internal fixation using a seven-hole proximal humerus internal locking system plate.
Radiographs demonstrated fracture union with residual varus deformity of the proximal femur, with a neck-shaft angle of approximately 110°. The patient remained asymptomatic and was mobilized to full weight-bearing without external support.
Fifteen months postoperatively, she developed progressive pain in the affected hip associated with limping. Clinical examination revealed restricted hip movements with an external rotation deformity. Radiographic evaluation confirmed SCFE with retained cannulated screws and associated coxa vara deformity. Vitamin D levels and repeat endocrine evaluation were normal. Revision surgery was advised; however, the patient was lost to follow-up.
SCFE following surgical treatment of femoral neck fractures in skeletally immature patients is a rare but clinically significant entity. In the absence of endocrine abnormalities, mechanical factors such as inadequate fracture reduction, residual coxa vara deformity, and altered shear forces across the proximal femoral physis are likely contributors.
The retained cannulated screws may also have contributed to altered stress distribution across the proximal femoral physis. Previous reports have suggested that screw proximity, penetration, or tethering effects near the physis may increase local mechanical stress and predispose to epiphyseal instability. In the present case, detailed implant trajectory analysis was not available; however, implant-related physeal stress cannot be excluded as a contributing factor.
Previous reports have suggested implant-related irritation, premature weight-bearing, delayed union or non-union, avascular necrosis, and post-traumatic angular deformities as possible etiological factors. The residual varus deformity observed in our patient may have increased physeal shear stress, predisposing to epiphyseal slip.
Gopinathan et al. reported a case of a 10-year-old boy who sustained bilateral femoral neck fractures and was treated with closed reduction and internal fixation using percutaneous cannulated screws. The patient subsequently developed non-union and SCFE on one side 5 months after surgery. (Fig. 1 & 2).
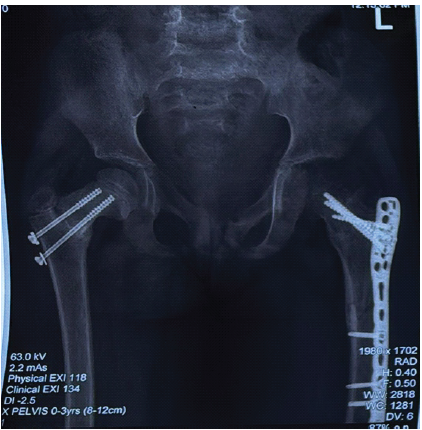
Figure 1: Immediate post-operative radiograph.
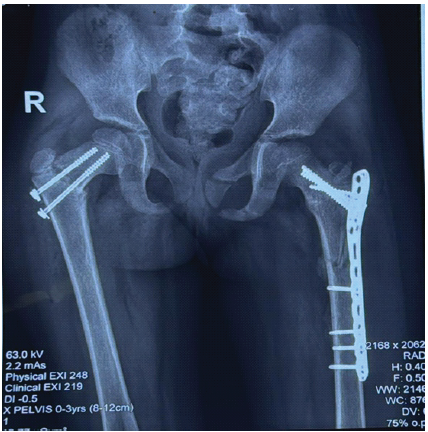
Figure 2: Post-operative radiograph at 6 weeks.
The authors attributed the development of SCFE to factors such as the precarious blood supply of the growing femoral head, non-union at the fracture site, and premature weight-bearing. Management consisted of open reduction and percutaneous cannulated screw fixation combined with a non-vascularized fibular graft [4].
Manukaran reported a case of SCFE in a 9-year-old boy occurring 14 months after internal fixation of a femoral neck fracture with cancellous screws, and suggested that implant penetration or proximity of the screw tip to the epiphyseal plate was a contributing factor in the development of the epiphyseal slip [5]. (Fig. 3).

Figure 3: Radiograph at 15 months postoperatively.
Ok et al. reported a case of a 6-year-old boy who developed SCFE, following malunion of a subtrochanteric femoral fracture. The authors attributed the development of SCFE to altered shear forces across the proximal femoral physis secondary to the deformity [6].
Ogden reported a case of SCFE occurring 15 months after a femoral neck fracture in an 11-year-old boy who was initially treated with hip spica immobilization and subsequently underwent a subtrochanteric valgus osteotomy for delayed union and coxa vara deformity. The author concluded that post-traumatic angular deformities of the proximal femur can predispose to physeal slip and emphasized the importance of restoring normal anatomic alignment during the management of proximal femoral fractures [7].
Jung and Park described a case of SCFE in an 11-year-old boy who sustained a Delbet Type III femoral neck fracture and was treated with open reduction and internal fixation using cannulated screws. Fifteen months postoperatively, epiphyseal slip was identified and managed with in situ fixation combined with a subtrochanteric valgus osteotomy [8].
Lahoti et al. reported two cases of separation of the proximal femoral epiphysis following derotation varus osteotomy of the femur, a commonly performed elective procedure for the management of developmental dysplasia of the hip. Unlike trauma-related cases, these epiphyseal separations were attributed specifically to the surgical procedure itself and likely represent a different etiology and pathophysiological mechanism [9].
In a comprehensive review, Finnegan explored the possible etiological and pathogenic mechanisms underlying this rare complication. Still, they concluded that larger, multicenter, and multinational studies would be required to draw definitive conclusions due to the limited number of reported cases [10].
Excluding the two cases reported by Lahoti et al. [9], only eight cases of SCFE following femoral neck or proximal femoral fracture treatment have been documented in the English-language literature. Notably, the majority of these cases have been reported from Asia, with the exception of the case described by Ogden et al. [8] Whether this apparent regional predominance reflects a true geographical or genetic predisposition remains unclear and warrants further investigation.
Because this complication is rare, a definite causal relationship cannot be established. The etiology is likely multifactorial, involving both mechanical and possible biological factors.
This case highlights that radiographic union alone should not be considered the endpoint of treatment in skeletally immature patients. Residual proximal femoral malalignment may continue to alter physeal loading and predispose to delayed slip.
Published literature on this complication remains sparse and consists largely of isolated case reports, limiting robust comparison and deeper etiological analysis.
Delayed SCFE is a rare but serious complication following pediatric femoral neck fracture fixation. Anatomical reduction, restoration of neck-shaft angle, stable fixation, cautious rehabilitation, and prolonged follow-up until skeletal maturity are essential for prevention and early diagnosis.
Limitations
This report is limited by its single-case design, which precludes establishing a definite causal relationship between femoral neck fracture fixation and subsequent SCFE. Long-term clinical and radiological outcomes could not be assessed because the patient was lost to follow-up after diagnosis. Functional outcome scores were unavailable. Radiographic follow-up intervals were limited, and advanced imaging such as magnetic resonance imaging or computed tomography was not performed. Implant position and residual deformity analysis were not comprehensive. Detailed implant position analysis with respect to screw trajectory, tip-to-physis distance, and possible physeal irritation was not available, limiting assessment of implant-related causation. Although routine endocrine investigations were normal, subtle metabolic abnormalities cannot be excluded. No gait or biomechanical analysis was available. In addition, the rarity of this complication and the limited published literature restrict the broader generalization of findings. Potential reporting bias must also be considered because unusual complications are more likely to be published.
Delayed SCFE can occur even after apparent union of pediatric femoral neck fractures. Residual coxa vara and altered biomechanics may predispose to slip; therefore, restoration of anatomy and long-term surveillance are essential.
References
- 1. Azouz EM, Karamitsos C, Reed MH, Baker L, Kozlowski K, Hoeffel JC. Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-20. [Google Scholar] [PubMed]
- 2. Li H, Zhao L, Huang L, Kuo KN. Delayed slipped capital femoral epiphysis after treatment of femoral neck fracture in children. Clin Orthop Relat Res 2015;473:2712-7. [Google Scholar] [PubMed]
- 3. Shrader MW, Jacofsky DJ, Stans AA, Shaughnessy WJ, Haidukewych GJ. Femoral neck fractures in pediatric patients: 30 Years experience at a level 1 trauma center. Clin Orthop Relat Res 2007;454:169-73. [Google Scholar] [PubMed]
- 4. Gopinathan NR, Chouhan D, Akkina N, Behera P. Case report: Bilateral femoral neck fractures in a child and a rare complication of slipped capital epiphysis after internal fixation. Clin Orthop Relat Res 2012;470:2941-5. [Google Scholar] [PubMed]
- 5. Manukaran MN, Abdul Hamid AK. Slipped capital femoral epiphysis caused by an implant–a case report. J Singapore Med J 1989;30:406-7. [Google Scholar] [PubMed]
- 6. Ok IY, Kim YS, Kwon YJ. A slipped capital femoral epiphysis following ipsilateral femoral subtrochanteric fracture: A case report. J Korean Soc Fract 2002;15:526-30. [Google Scholar] [PubMed]
- 7. Ogden JA, Gossling HR, Southwick WO. Slipped capital femoral epiphysis following ipsilateral femoral fracture. Clin Orthop Relat Res 1975;110:167-70. [Google Scholar] [PubMed]
- 8. Jung ST, Park GH. Slipped capital femoral epiphysis following fracture of the femoral neck: A case report. J Pediatr Orthop B 2012;21:579-82. [Google Scholar] [PubMed]
- 9. Lahoti O, Turnbull TJ, Hinves BL. Separation of the proximal femoral epiphysis after derotation varus osteotomy of the femur. J Pediatr Orthop 1998;18:662-4. [Google Scholar] [PubMed]
- 10. Finnegan MA. CORR insights®: Delayed slipped capital femoral epiphysis after treatment of femoral neck fracture in children. Clin Orthop Relat Res 2015;473:2718-20. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report June 1, 2026 A 5-Year Outcome of Closed Reduction and Screw Fixation for an Atypical Slipped Capital Femoral Epiphysis Associated with Hypogonadism: A Case Report
June 1, 2026 A 5-Year Outcome of Closed Reduction and Screw Fixation for an Atypical Slipped Capital Femoral Epiphysis Associated with Hypogonadism: A Case Report June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report