
Single-staged arthroscopic management of multiple internal derangements of the knee is a feasible option that reduces patient morbidity. With carefully planned rehabilitation and meticulous surgical technique, favorable outcomes can be achieved in the majority of cases.
Dr. Vishesh Verma, Department of Orthopedics, Sarvodaya Healthcare and Research Centre, Faridabad, Haryana, India. E-mail: vishesh776@gmail.com
Abstract
Introduction: Posterior meniscal root tears affecting both menisci are rare occurrences, as their injury mechanisms differ significantly. While most root avulsions involve soft tissue, to our knowledge, bony avulsions of both posterior meniscal roots as discrete fragments have not been previously reported in the literature. Pang et al. (2025) described a unified intercondylar eminence fracture with both roots attached to a single fragment, but separate bony avulsion fractures of each root represent a distinct clinical challenge.
Case Report: We present the case of a 28-year-old male with discrete bony avulsion fractures of both posterior meniscal roots accompanied by a concomitant anterior cruciate ligament (ACL) tear. The patient was managed with a single-staged arthroscopic procedure. ACL reconstruction was performed using quadrupled hamstring autograft (semitendinosus and gracilis) with adjustable-loop cortical button fixation on the femoral side and bioabsorbable interference screw fixation on the tibial side. Two separate trans-osseous tunnels were created – one for each discrete bony root fragment – with pullout sutures from each tunnel secured independently over a single cortical button.
Conclusion: This case presented a unique surgical dilemma regarding the optimal fixation strategy for discrete dual bony root avulsions. The arthroscopic single-stage approach minimized surgical morbidity, facilitated early rehabilitation, and yielded favorable short-term outcomes. An extensive literature review of similar cases is presented in tabulated form, providing readers with a comprehensive comparison of various management strategies reported by multiple authors.
Keywords: Anterior cruciate ligament tear, posterior meniscal root, bony avulsion, dual root avulsion fracture, transosseous tunnel pullout repair, arthroscopic reconstruction.
The importance of meniscal roots has been well documented in orthopedic literature. Injury to a meniscal root leads to loss of hoop stresses in the affected compartment, causing abnormal increases in tibiofemoral contact pressures, altered knee joint kinematics, and accelerated development of degenerative joint disease [1]. Since the lateral and medial menisci differ with regard to anatomy and biomechanics, the pathologies leading to avulsion of their respective roots also differ substantially. Lateral posterior meniscal root tears are predominantly traumatic and nearly always associated with anterior cruciate ligament (ACL) injury [2]. Conversely, medial meniscus (MM) posterior root tears are typically related to chronic degenerative processes [3].
Concomitant tears of the posterior roots of both menisci are exceedingly rare and are documented in the literature through only a handful of case reports [4,5,6,7,8,9,10]. Among these, Pang et al. reported a case involving bony avulsion of both roots; however, their case featured a single large intercondylar eminence fracture fragment with both meniscal roots attached to it [10]. To our knowledge, the present case represents the first report of dual posterior meniscal root bony avulsions occurring as two anatomically discrete bony fragments in conjunction with an ACL tear.
A 28-year-old male presented to our outpatient clinic with complaints of pain and instability in his right knee of 3 weeks’ duration. He reported difficulty walking and was unable to squat or sit cross-legged, which significantly impaired his daily activities. The patient provided a history of trauma occurring 1 month prior, when his motorcycle skidded off the side of a road due to a pothole. He landed awkwardly on the affected limb, sustaining multiple contusions and abrasions. After receiving primary care at a nearby hospital, he did not seek further consultation, hoping for spontaneous recovery. As his symptoms persisted and worsened, he presented to our institution.
On physical examination, we documented a positive Lachmann test. McMurray’s test was deferred due to pain. There was tenderness along both the medial and lateral joint lines, and knee flexion was limited secondary to pain and effusion. Plain radiographs (Fig. 1) were unremarkable. Magnetic resonance imaging (MRI) revealed a full-thickness ACL tear from the femoral footprint, injury to the posterior horn of the MM extending to the root with bony avulsion, and bony avulsion fracture of the posterior root of the lateral meniscus (Fig. 2a, b, c).
Figure 1: Pre-operative anteroposterior and lateral radiographs of the right knee showing no obvious bony abnormality.
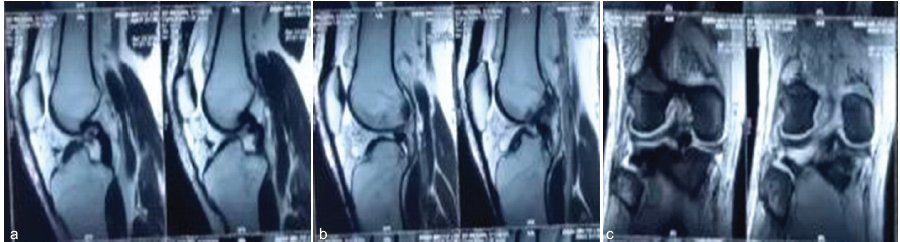
Figure 2: (a) Pre-operative sagittal T2-weighted magnetic resonance imaging (MRI) demonstrating bony avulsion of the medial meniscus posterior root. (b) Pre-operative sagittal T2-weighted MRI demonstrating bony avulsion of the lateral meniscus posterior root. (c) Pre-operative coronal T2-weighted MRI showing dual posterior meniscal root bony avulsions.
The patient was scheduled for surgical intervention. Clinical evaluation under anesthesia corroborated pre-operative findings. Diagnostic arthroscopy revealed a complete ACL tear from its femoral attachment and discrete bony avulsion fractures of the posterior roots of both the lateral and medial menisci (Fig. 3a and b). No other intra-articular pathology was detected. We elected to reconstruct the ACL using a quadrupled hamstring autograft and to address each meniscal root independently using separate transosseous pullout tunnels.
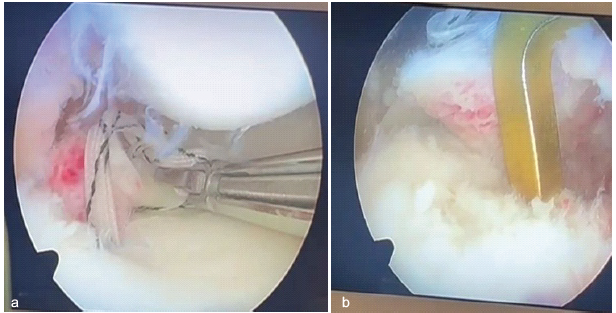
Figure 3: (a) Intraoperative arthroscopic image showing bony avulsion of the lateral meniscus posterior root. (b) Intraoperative arthroscopic image showing bony avulsion of the medial meniscus posterior root.
Surgical technique
Step 1: Femoral tunnel drilling
After adequate debridement of the ACL’s femoral footprint, an offset guide was used to mark and drill the femoral tunnel for ACL reconstruction, followed by passage of a suture loop to secure the tract.
Step 2: Securing the medial meniscal root
The avulsed medial meniscal root with its attached bony fragment was debrided of fibrous tissue and tagged using braided ultra-high molecular weight polyethylene suture tape with a MINI FIRSTPASS suture passer device. The fracture bed was debrided and curetted to promote healing. Using a transtibial ACL guide set at 45°, we drilled a 4.5-mm trans-osseous tunnel from the anatomic root attachment site, exiting anteromedially on the proximal tibial metaphysis, approximately 1–2 cm medial to the tibial tuberosity and 3 cm distal to the joint line. This positioning was deliberately selected to avoid convergence with the planned ACL tibial tunnel. The suture tape was then shuttled through this tunnel using a suture retriever.
Step 3: Securing the lateral meniscal root
The lateral meniscal root bony fragment was similarly prepared and tagged with fiber tape. The original anatomic footprint was prepared but slightly adjusted (2–3 mm posteriorly) to further minimize the risk of tunnel convergence with the ACL tibial tunnel while maintaining biomechanical function. A 4.5 mm transosseous tunnel was drilled at 45°, exiting anterolaterally on the proximal tibia. The fiber tape was shuttled through this tunnel.
Step 4: ACL tibial tunnel drilling
The ACL guide is now set at 55° and a tunnel was drilled through the footprint of remnant ACL (anterior half of the footprint) positioned far medially over the proximal tibia medial condyle to avoid tunnel collision. The suture loop previously left in the femoral tunnel is not shuttled through this tunnel.
Step 5: Final fixation sequence
Fixation was performed in the following sequence to optimize graft and repair tension:
- The ACL graft was first secured on the femoral side using an adjustable-loop cortical suspension device
- Both fiber tapes from the medial and lateral meniscal roots were passed through a single 4-hole cortical button (OPENBUTTON, Sironix Ortho, Ahmedabad, India) positioned on the anterior tibial cortex. The meniscal roots were reduced anatomically under arthroscopic visualization. Tension was applied to each root independently at 30° of knee flexion with the knee in neutral rotation. The sutures were tied securely over the cortical button with the surgeon applying manual posterior drawer force to reduce the tibia and maintain appropriate graft tension
- Finally, the ACL graft was fixed on the tibial side at 10° of knee flexion in neutral rotation using a bioabsorbable interference screw
- Post-operative radiographs confirmed appropriate hardware positioning without fracture or tunnel convergence (Fig. 4).

Figure 4: Post-operative anteroposterior and lateral radiographs
demonstrating appropriate tunnel positioning and cortical button placement without convergence.
Post-operative rehabilitation
The patient was placed in a hinged knee brace locked in extension for the first 2 weeks. Non-weight-bearing toe-touch ambulation using a walker was permitted from post-operative day 1. Isometric quadriceps and hamstring strengthening exercises in a closed-chain manner were initiated on the 2nd post-operative day. Range of motion (ROM) was progressively increased by 30° weekly until reaching 90°, which was maintained until 6 weeks postoperatively to protect the meniscal root repairs.
At 6 weeks, partial weight-bearing (25–50% body weight) was permitted with bilateral crutches, and unrestricted ROM exercises were initiated. Progressive weight-bearing advancement continued over the subsequent 6 weeks. At 3 months postoperatively, the patient was ambulating independently with full weight-bearing using elbow crutches as a protective aid during dynamic activities such as pivoting and stair negotiation. This precautionary measure was implemented based on known healing timelines of meniscal root repairs and to minimize shear forces during the critical graft incorporation phase. Clinical examination at 3 months revealed no effusion, full active extension, flexion to 120°, negative Lachmann test, and the patient reported minimal pain (Visual Analog Scale 1/10) with activities of daily living.
Historically underappreciated as an etiology of knee pain and early-onset osteoarthritis, the meniscal root plays a vital biomechanical role in maintaining knee joint longevity [11]. Meniscal root tear is defined as a complete bony or soft tissue avulsion of the root attachment or a radial tear occurring within 1 cm of the meniscal root attachment [12,13]. Biomechanical studies have demonstrated that contact area and pressure changes across the knee joint following a meniscus root tear are comparable to those of a meniscus-deficient state [14]. A strong correlation exists between meniscal root tears and accelerated progression of knee osteoarthritis [15]. For years, the accepted treatment for these injuries was meniscectomy; however, as contemporary evidence has accumulated, the trend has shifted decisively toward meniscal preservation through repair techniques.
Fixation technique selection and rationale
Various techniques are available for meniscal root repair, including side-to-side all-inside repair, suture anchors, knotless suture anchors, and trans-osseous tunnel repair [16]. Among these options, repairs utilizing transosseous tunnels have been reported as biomechanically superior, achieving near-anatomic restoration of joint kinematics, including contact pressures and hoop stresses [17,18,19,20]. In cadaveric studies, transosseous pullout repair has been shown to restore approximately 90% of native meniscal root function, whereas suture anchor techniques typically restore only 60–70% [18]. This biomechanical advantage formed the primary rationale for our technical choice.
A legitimate concern with transosseous techniques is the potential for tunnel convergence, particularly when concurrent ligament reconstruction is required. We addressed this concern through meticulous pre-operative planning and intraoperative modification of tunnel positioning. We drilled the meniscal root tunnels first at 45°, deliberately positioning their tibial exit points approx. 2 cm from the tibial tuberosity to create adequate spacing. The ACL tibial tunnel was drilled at 55° with a more anterior and medial positioning, ensuring a good bone bridge between all tunnels, under fluoroscopic guidance. We also accepted a slight posterior adjustment (2–3 mm) of the lateral meniscal root footprint to optimize tunnel divergence while maintaining biomechanical function based on finite element analysis, suggesting preserved hoop stresses within 3 mm of anatomic positioning [19]. Fig. 5 highlights our tunnel placements compared to others in the literature [7,10] to avoid such a complication.
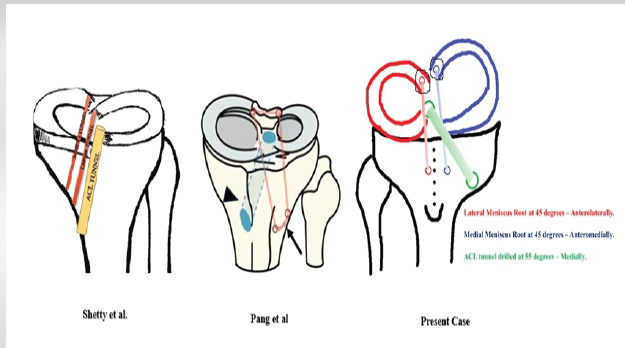
Figure 5: Schematic comparison of transosseous tunnel positioning strategies. (a) Shetty et al., (b) Pang et al. for unified fragment (c) Present case showing divergent tunnel arrangement with anterior cruciate ligament tibial tunnel at 55° and meniscal root tunnels at 45°. Note the deliberate spacing maintained between tunnels
to prevent tunnel convergence.
In comparison, alternative fixation strategies had significant limitations in our case. Suture Anchors, while avoiding tunnel convergence risk, provide inferior biomechanical stability for bony avulsion fragments. Load-to-failure testing demonstrates that transosseous repair offers approximately 30–40% greater fixation strength than anchor-based techniques [20]. Given the young age and anticipated activity level of our patient, we prioritized biomechanical strength. The approach of using a single unified tunnel [6] risks differential tensioning of the two roots, potentially under-tensioning one while over-tensioning the other. With discrete bony fragments, independent control of each root was deemed essential to restore hoop stresses symmetrically across both compartments. Bony Bridge Tie-Over as highlighted by a case report [10] is well-suited for unified intercondylar eminence fractures but cannot be applied to anatomically discrete bony fragments separated by an intact tibial plateau.
Simultaneous injuries involving both meniscal root avulsions are rare and present significant challenges in knee surgery. Available literature on these complex injury patterns is limited to case reports and technical notes, with most describing combinations of ACL or posterior cruciate ligament tears with dual meniscal root injuries [4,5,6,7,8,9,10]. As shown in Table 1, most reported cases involve soft tissue avulsions or radial tears; only one case report [10] previously described bony involvement, though as a unified fragment rather than discrete avulsions.
The biomechanical explanation for dual bony root avulsions in our case likely relates to the specific injury mechanism – a high-energy motorcycle accident with combined axial loading, rotation, and valgus stress. This differs from the injury patterns in degenerative cases (typically medial root alone) [3] or isolated sports trauma (typically lateral root with ACL) [2]. These injuries are notoriously difficult to diagnose on pre-operative imaging and may be missed on MRI, particularly when there is substantial joint effusion [12]. Our case reinforces the critical importance of systematic arthroscopic evaluation of all meniscal roots in acute knee injuries, as failure to identify and repair these lesions results in functional outcomes equivalent to total meniscectomy [14].
The literature demonstrates a trend toward single-stage arthroscopic surgery with independent transtibial tunnels for both meniscal roots [4,5,6,7,8,9,10].
However, rehabilitation protocols must be carefully tailored based on fixation strength, concomitant injuries, and individual patient factors. Meniscal root repairs require 12–16 weeks for fibrovascular healing and biological incorporation at the bone-soft tissue interface [15]. Early aggressive loading risks repair failure or plastic deformation of the healing tissue. Premature unrestricted activity has been associated with repair failure rates of 15–25% [20]. With two independent root repairs and concurrent ACL reconstruction, the cumulative stress on the knee during dynamic activities (pivoting, squatting, and stairs) is substantially higher than with isolated injuries. We hence employed a careful rehab protocol wherein the patient was even advised to use crutches after 12-week post-operative during dynamic activities. Successful cases with long-term follow-up [5,10] employed similar cautious progressive loading protocols.
Early mobilization is indeed vital for cartilage nutrition, proprioceptive recovery, and muscle function; however, this must be balanced against biological healing constraints. Our protocol achieved this balance by allowing unrestricted ROM from 6 weeks while continuing protected loading to 12–16 weeks.
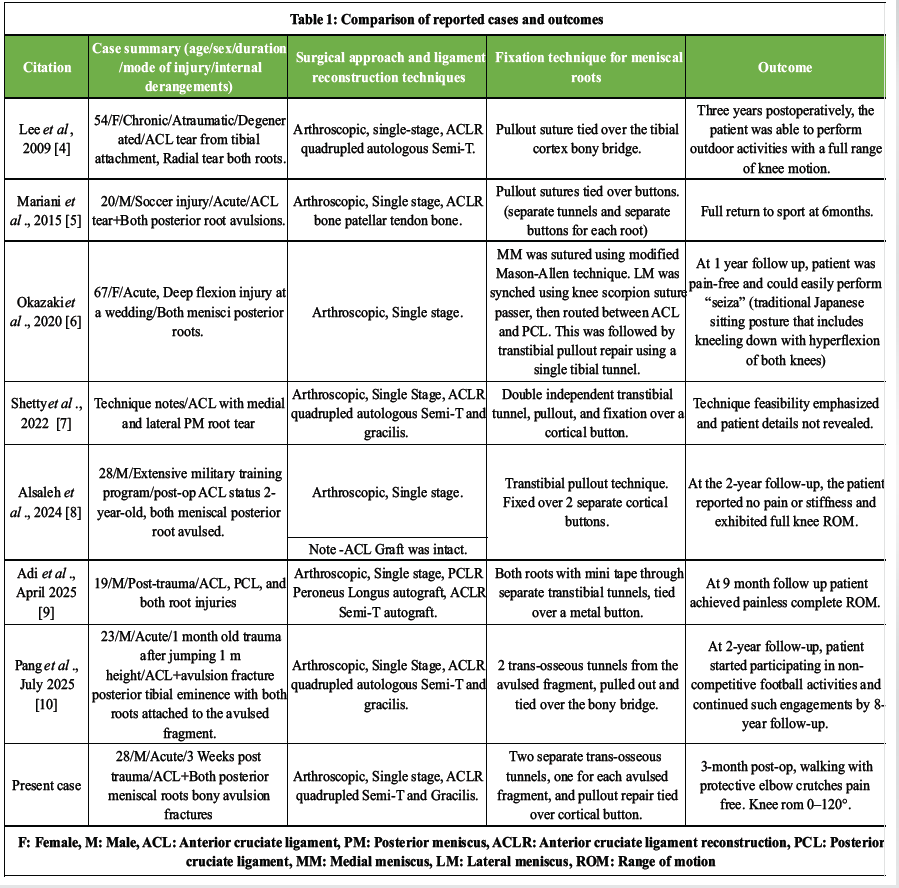
Table 1: Comparison of reported cases and outcomes
Table 1 compares available literature to our case, highlighting similarities and differences in patient presentation, surgical approach, fixation techniques, and outcome measures.
- Concomitant posterior meniscal root tears of both menisci, although rare, require individualized surgical strategies. To our knowledge, discrete bony avulsion fractures of both posterior roots (medial and lateral) represent a unique injury pattern not previously reported in detail.
- Arthroscopic approaches minimize morbidity, allow comprehensive intra-articular assessment, and should be prioritized when technically feasible.
- Trans-osseous pullout repair offers biomechanical advantages for bony avulsion fragments but requires meticulous tunnel planning to prevent convergence when performed in conjunction with ligament reconstruction.
- Early, but carefully progressed rehabilitation is achievable and leads to favorable outcomes in most cases.
- More longitudinal studies and larger case series are needed to establish standardized protocols for diagnosis, surgical sequencing, fixation techniques, and rehabilitation in these exceedingly rare and complex injuries.
We advocate that in all acute ACL tears, surgeons should systematically probe meniscal roots during arthroscopy, as these injuries are difficult to diagnose radiologically and may be missed even on high-quality MRI. They warrant careful arthroscopic evaluation; if overlooked, they can have potentially devastating consequences due to loss of meniscal function, as untreated root tears are biomechanically equivalent to total meniscectomy.
References
- 1. Sgaglione NA, Lubowitz JH, Provencher MT. AANA Advanced Arthroscopic Surgical Techniques: The Knee. Thorofare, NJ: SLACK Incorporated; 2016. p. 103-4. [Google Scholar] [PubMed]
- 2. Ahn JH, Lee YS, Chang JY, Chang MJ, Eun SS, Kim SM. Arthroscopic all inside repair of the lateral meniscus root tear. Knee 2009;16:77-80. [Google Scholar] [PubMed]
- 3. Hwang BY, Kim SJ, Lee SW, Lee HE, Lee CK, Hunter DJ, et al. Risk factors for medial meniscus posterior root tear. Am J Sports Med 2012;40:1606-10. [Google Scholar] [PubMed]
- 4. Lee JH, Hwang BY, Lim YJ, Kim KH, Song JH. Radial tears in the roots of the posterior horns of both the medial and lateral menisci combined with anterior cruciate ligament tear: A case report. Knee Surg Sports Traumatol Arthrosc 2009;17:1340-3. [Google Scholar] [PubMed]
- 5. Mariani PP, Iannella G, Cerullo G, Giacobbe M. Avulsion of both posterior meniscal roots associated with acute rupture of the anterior cruciate ligament. J Orthop Traumatol 2015;16:259-62. [Google Scholar] [PubMed]
- 6. Okazaki Y, Furumatsu T, Kodama Y, Matsumoto Y, Takahashi M, Ozaki T. Medial and lateral meniscus posterior root tears with an intact anterior cruciate ligament. Case Rep Orthop 2020;2020:8842167. [Google Scholar] [PubMed]
- 7. Shetty CC, Ming W, Lee YH. Concomitant medial and lateral meniscus posterior horn root repair with ACL reconstruction using trans-tibial tunnel technique. Arthrosc Tech 2023;12:e477-82. [Google Scholar] [PubMed]
- 8. Alsaleh NS, Alnasser AA, Alqahtani AA. A case report of simultaneous tears of the medial and lateral posterior meniscal roots with an intact ACL graft. Int J Surg Case Rep 2024;121:109971. [Google Scholar] [PubMed]
- 9. Adi MM, Mohamed AM, Abdulgadir M, Meda MR, Mohamed NA, AlKhyeli J. Management of a complex multiligament knee injury: Simultaneous reconstruction of ACL, PCL, and both meniscal roots. Int J Surg Case Rep 2025;129:111150. [Google Scholar] [PubMed]
- 10. Pang Y, Xu S, Xiang G, Zhang K, Sun T. Anterior cruciate ligament reconstruction simultaneously with trans-tibial pull-out fixation of avulsion fracture of medial and lateral meniscus posterior roots: A case report and eight-year follow-up. BMC Musculoskelet Disord 2025;26:622. [Google Scholar] [PubMed]
- 11. Floyd ER, Rodriguez AN, Falaas KL, Carlson GB, Chahla J, Geeslin AG, et al. The natural history of medial meniscal root tears: A biomechanical and clinical case perspective. Front Bioeng Biotechnol 2021;9:744065. [Google Scholar] [PubMed]
- 12. Matheny LM, Ockuly AC, Steadman JR, LaPrade RF. Posterior meniscus root tears: Associated pathologies to assist as diagnostic tools. Knee Surg Sports Traumatol Arthrosc 2015;23:3127-31. [Google Scholar] [PubMed]
- 13. LaPrade RF, Padalecki JR, Jansson K, Smith S, Dornan G, Pierce C, et al. Biomechanical consequences of a complete radial tear adjacent to the medial meniscus posterior root attachment site. Orthop J Sports Med 2014;2 3 Suppl:699-707. [Google Scholar] [PubMed]
- 14. Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus. Similar to total meniscectomy. J Bone Joint Surg Am 2008;90:1922-31. [Google Scholar] [PubMed]
- 15. Banovetz MT, Roethke LC, Rodriguez AN, LaPrade RF. Meniscal root tears: A decade of research on their relevant anatomy, biomechanics, diagnosis, and treatment. Arch Bone Jt Surg 2022;10:366-80. [Google Scholar] [PubMed]
- 16. Homan MD, Braaten JA, Banovetz MT, Kennedy NI, LaPrade RF. Meniscal root tears: Repair and salvage techniques. J Cartilage Joint Preserv 2023;3:100098. [Google Scholar] [PubMed]
- 17. LaPrade CM, James EW, Cram TR, Feagin JA, Engebretsen L, LaPrade RF. Meniscal root tears: A classification system based on tear morphology. Am J Sports Med 2015;43:363-9. [Google Scholar] [PubMed]
- 18. Padalecki JR, Jansson KS, Smith SD, Dornan GJ, Pierce CM, Wijdicks CA, et al. Biomechanical consequences of a complete radial tear adjacent to the medial meniscus posterior root attachment site: In situ pull-out repair restores derangement of joint mechanics. Am J Sports Med 2014;42:699-707. [Google Scholar] [PubMed]
- 19. Aspden RM, Yarker YE, Hukins WL. Collagen orientations in the meniscus of the knee joint. J Anat 1985;140:371-80. [Google Scholar] [PubMed]
- 20. Moon HK, Koh YG, Kim YC, Park YS, Jo SB, Kwon SK. Prognostic factors of arthroscopic pull-out repair for a posterior root tear of the medial meniscus. Am J Sports Med 2012;40:1138-43. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Two Cases of Anterolateral Meniscofemoral Ligament of the Lateral Meniscus
October 1, 2025 Two Cases of Anterolateral Meniscofemoral Ligament of the Lateral Meniscus August 1, 2025 Posterior Cruciate Ligament Rupture in Klippel–Trenaunay Syndrome: Case Report and Review of Literature
August 1, 2025 Posterior Cruciate Ligament Rupture in Klippel–Trenaunay Syndrome: Case Report and Review of Literature August 1, 2025 Personalized Alignment Strategies and the Need for Customization in Total Knee Arthroplasty: The Role of MISSO Joint Robotic System
August 1, 2025 Personalized Alignment Strategies and the Need for Customization in Total Knee Arthroplasty: The Role of MISSO Joint Robotic System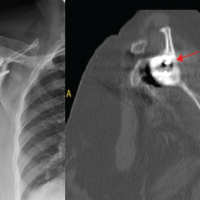 January 1, 2025 Diagnosing Mycobacterium Kansasii in Shoulder Periprosthetic Joint Infection: A Rare Case Report
January 1, 2025 Diagnosing Mycobacterium Kansasii in Shoulder Periprosthetic Joint Infection: A Rare Case Report