
Galeazzi fractures can occur from a ballistic gunshot mechanism. These injuries can typically be treated with rigid internal fixation of the radial shaft alone.
Dr. Timothy Westbrooks, Department of Orthopaedic Surgery, Emory University School of Medicine, Atlanta, Georgia, USA. E-mail: twestb2@emory.edu
Abstract
Introduction: Galeazzi fractures, defined as fractures of the radial shaft with associated dislocation of the distal radioulnar joint (DRUJ), are uncommon injuries typically caused by high-energy blunt trauma or falls onto an outstretched hand. Ballistic mechanisms rarely produce this fracture pattern because they lack the torsional forces usually required to disrupt the DRUJ. Only isolated case reports of such injuries exist in the literature. This report presents the largest known case series of Galeazzi fractures resulting from gunshot wounds, providing new insight into their mechanism, management, and outcomes.
Case Report: Six patients, four males and two females, between 25 and 52 years of age, sustained Galeazzi fractures following low-velocity gunshot wounds. Several were polytraumatized with concomitant injuries to other extremities or the abdomen. All patients underwent operative fixation of the radial shaft using rigid internal fixation constructs. In each case, the DRUJ was evaluated intraoperatively after fixation and was found to be stable without the need for additional surgical stabilization. Post-operative immobilization consisted of short-term splinting followed by early mobilization. At follow-up, all patients demonstrated fracture healing and functional forearm rotation without pain or DRUJ instability. Despite an average of 10.9 mm of initial radial shortening relative to the ulna, no patient developed instability requiring further surgical intervention.
Conclusion: This case series expands current understanding of Galeazzi fracture patterns by demonstrating that ballistic mechanisms, though uncommon, can produce this distinctive injury without the classic torsional loading. These findings suggest that stable DRUJ alignment can often be achieved through rigid fixation of the radial shaft alone, even in the setting of significant shortening from ballistic trauma. This report adds novel evidence to the orthopedic literature by highlighting a previously underrecognized mechanism of Galeazzi injury. It supports the importance of thorough intraoperative assessment of DRUJ stability following fixation. The clinical impact extends beyond trauma surgery by reinforcing that fracture pattern, rather than mechanism alone, should guide management decisions.
Keywords: Galeazzi fracture, ballistic injury, distal radioulnar joint, radial shaft fracture, gunshot wound.
Galeazzi injuries are fractures of the radial shaft associated with dislocation of the distal radioulnar joint (DRUJ). This injury was first described in 1822 by Astley Cooper, and later further discussed in a case series of 18 patients treated by Riccardo Galeazzi [1]. These are typically the result of high-energy blunt trauma [2]. Dorsal dislocations are most common and are thought to occur from hyperpronation and wrist extension, as occurs from a fall onto an outstretched hand. These are relatively rare injuries with reports indicating an incidence of ≤3% of forearm fractures in children and ≤7% in adults [3]. Because Galeazzi fractures occur rarely in most surgeons’ practices, they can be easily missed if not appropriately evaluated by the clinician.
Galeazzi fractures typically result from a fall or blunt trauma, with torsional force through the DRUJ in combination with radial shortening, disrupting interosseous ligaments. Biomechanical studies have demonstrated that fractures of the distal one third radial shaft are more likely to disrupt the DRUJ than more proximal fractures [2]. Furthermore, wide displacement of the DRUJ and excessive radial shortening of more than 5–7 mm are risk factors for persistent DRUJ instability. Ballistic injuries are rarely reported as a cause of Galeazzi fractures. The lack of torsion across the DRUJ makes it a seemingly unlikely cause of DRUJ instability. To our knowledge, only a single case report exists describing such an injury [4].
Here we present a case series of six patients who sustained Galeazzi fractures from ballistic injuries.
Patient one
A 52-year-old male polytraumatized by multiple low-velocity gunshot wounds, including a tibia fracture and a left Galeazzi fracture (Fig. 1).
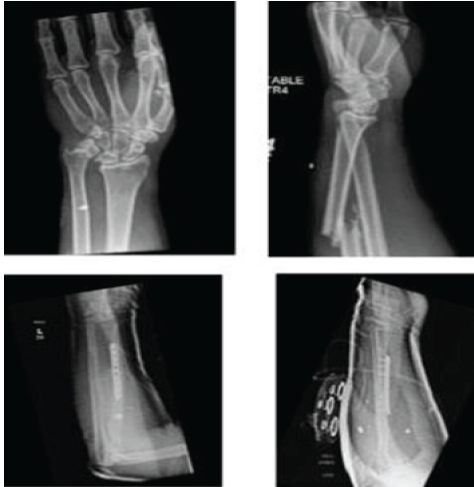
Figure 1: Pre-operative and post-operative radiographs of patient 1.
After obtaining rigid internal fixation of his radial shaft, his DRUJ was clinically stable to the shuck test. He was immobilized in a sugar-tong splint in neutral rotation to protect his DRUJ. This splint was removed at 2 weeks postoperatively, and he was allowed platform weight bearing to assist with overall mobilization. He was lost to follow-up until 16 weeks post-operative. At this time, he had 80° of pronation and supination without crepitus or pain at the wrist.
Patient two
A 27-year-old male sustained three gunshot wounds, causing a left femoral shaft fracture and a left Galeazzi fracture (Fig. 2).
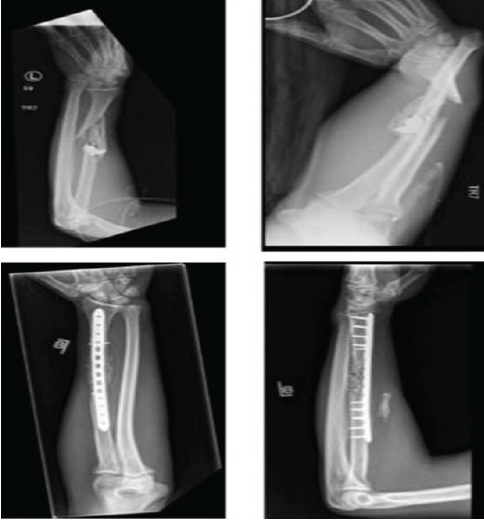
Figure 2: Pre-operative and post-operative radiographs of patient 2.
Both fractures were treated operatively during the same anesthetic event. The radial shaft had a significant amount of comminution and devitalized bone fragments that were debrided. The fracture was fixed with a bridge plate construct with cancellous bone chips and injectable demineralized bone fiber, given the bone loss. Against medical advice, he began using his arm for weight-bearing activities after the 2-week post-operative visit. At 6-weeks post-operative, he had no pain in his forearm and was functionally using his arm for activities of daily living and work. He was lost to follow-up after this visit.
Patient three
A 49-year-old male ballistic polytrauma patient with a right Galeazzi injury (Fig. 3).
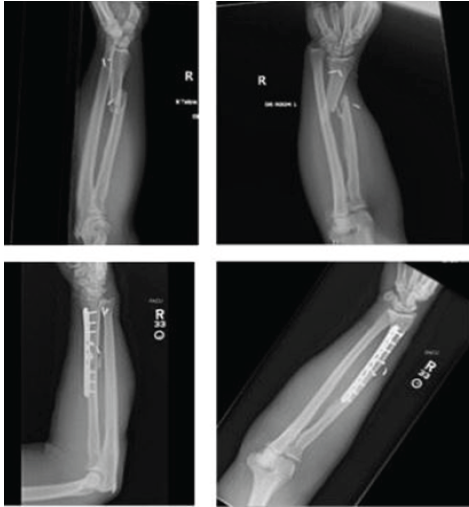
Figure 3: Pre-operative and post-operative radiographs of patient 3.
This fracture was treated on day 7 post-injury. After rigid fixation of his radial shaft, the DRUJ remained stable and was not immobilized. His hospital course was complicated due to abdominal injuries, and he was discharged on post-operative day 34. His first clinic visit was 8 months post-operative, and he had 5/5 wrist and hand strength with symmetric wrist and digit range of motion to his contralateral side. Radiographs demonstrated a healed radial shaft fracture without DRUJ instability.
Patient four
A 26-year-old female who sustained six low-velocity gunshot wounds, causing a splenic laceration, a left proximal humerus fracture, and a left Galeazzi fracture (Fig. 4) with radial, median, and ulnar neuropraxic injuries.

Figure 4: Pre-operative and post-operative radiographs of patient 4.
Intraoperatively, the median and ulnar nerves were contused but intact. After rigid fixation of her radial shaft, the DRUJ was stable. Postoperatively, she was treated with a volar slab splint and transitioned to a removable splint at 2-weeks. She continued to have paresthesia in the median, radial, and ulnar nerve distributions at the 1-year mark but was lost to follow-up before further intervention or diagnostic testing.
Patient five
A 31-year-old male who sustained an isolated ballistic left Galeazzi fracture with a radial shaft fracture at the metaphyseal–diaphyseal junction (Fig. 5).
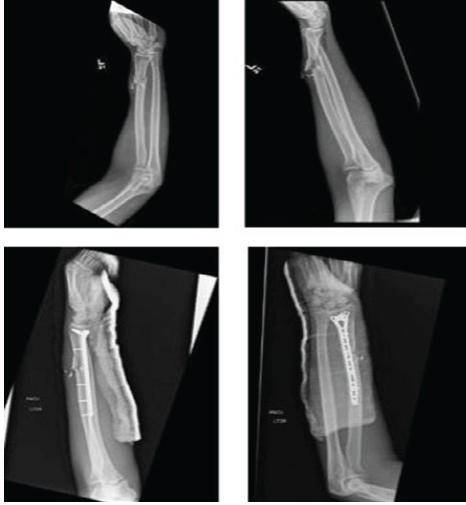
Figure 5: Pre-operative and post-operative radiographs of patient 5.
This was treated with open reduction internal fixation using a long distal radius volar locking plate. The DRUJ was stable after fixation of the radial shaft. A volar slab splint was applied for 2 weeks, at which time he was allowed passive and active wrist range of motion with continued non-weight bearing. At 6 weeks post-operative, the patient had no pain and a nearly symmetric range of motion to the contralateral side.
Patient six
A 25-year-old male who sustained an isolated ballistic left Galeazzi fracture (Fig. 6).

Figure 6: Pre-operative and post-operative radiographs of patient 6.
There was a large amount of comminution at the metaphyseal–diaphyseal junction. A long metadiaphyseal plate was applied to bridge the area of comminution after restoration of appropriate length, alignment, and rotation of the radial shaft. After rigid fixation of the radial shaft was obtained, the DRUJ was assessed clinically and determined to be stable. He was placed in a volar slab splint for 2 weeks and then transitioned to allow range of motion, but continued non-weight-bearing status. He began showing signs of interval callus formation at 3 months post-operative, and by 9 months post-operative, had healed his radial shaft fracture. His wrist flexion and extension were limited to 20° each, but his DRUJ remained stable without pain during pronation or supination (Table 1).
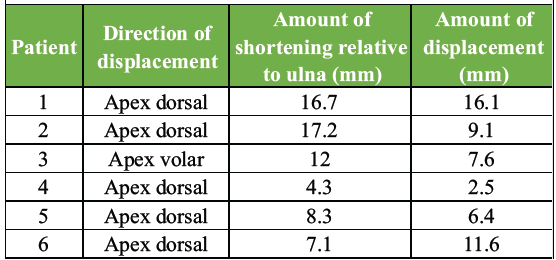
Table 1: Pre-operative fracture metrics
In an epidemiologic study on ballistic fractures, an estimated 240,555 patients sustained ballistic fractures over 20 years in the United States. In 2000, the fracture incidence rate was 15.7/1,000,000 person-years at risk (PYR), and this rose to 96.8 PYR in 2019 [5]. To our knowledge, this is the largest case series of ballistic Galeazzi fractures in the current orthopedic literature, consisting of six patients. We find these injuries interesting because they do not follow the typical injury pattern described for a Galeazzi injury. The DRUJ is primarily stabilized by the triangular fibrocartilage complex (TFCC), and disruption of the TFCC is required for a DRUJ dislocation to occur [6]. The TFCC originates from the base of the lunate fossa and attaches to the ulnar fovea and ulnar styloid. Because of this attachment at the distal ulna, shortening of the radial shaft can lead to disruption of the TFCC.
The interosseous membrane (IOM) is another critical structure to understand when discussing Galeazzi fractures because its disruption leads to shortening of the radial shaft. It consists of a central band, a proximal band, a membranous portion, and accessory bands. The central band originates from the proximal one-third of the radius and inserts at the distal quarter of the ulna. The distal one-third of the radial shaft is devoid of IOM attachment, which may be one reason why this fracture location has a higher risk of shortening and subsequent DRUJ dislocation. Schneiderman et al. performed a cadaveric study evaluating the impact that radial shaft shortening had on the IOM and TFCC [7]. After performing a radial osteotomy alone, there was 5 mm of shortening. Radial shortening of 5–10 mm was seen after radial osteotomy, and either TFCC or IOM transection, and shortening of >10 mm was seen after radial osteotomy, TFCC transection, and IOM transection. This study demonstrates the importance of DRUJ evaluation after radial shaft fractures, especially when associated with shortening of >5 mm. However, our case series of radial shaft fractures with DRUJ dislocation seems to refute this, as there was no obvious mechanism of injury to the IOM.
A recent systematic review of irreducible Galeazzi injuries provides important insight into predictors of DRUJ instability following radial shaft. The review identified 17 cases: Most fractures involved the distal third of the radius and were associated with an ulnar styloid base fracture in 94% of cases. Dorsal dislocation of the DRUJ was the most common pattern, present in 82% of cases, and was frequently blocked by interposition of the extensor carpi ulnaris. Volar dislocations were blocked by the volar capsule. More than half of the irreducible DRUJ dislocations were not recognized intraoperatively and were only identified postoperatively when persistent instability or incongruity became evident [8].
Anatomic reduction and rigid fixation of the radius alone is often sufficient to restore and maintain DRUJ stability in Galeazzi injuries. In a retrospective study of 14 adults treated with internal fixation of the radius and closed reduction of the DRUJ, the authors found excellent long-term clinical and radiographic results. Although six patients demonstrated mild DRUJ laxity on comparative ballottement testing, none reported pain during the maneuver, all exhibited near-symmetric forearm rotation, and there was no significant difference in range of motion between injured and uninjured sides. Grip strength averaged 77% of the contralateral wrist, mean pain on the Visual Analog Scale was 0.6, and mean disabilities of the Arm, Shoulder, and Hand score was 3. Dynamic computed tomography evaluation confirmed the absence of subluxation in all patients, and no cases of severe DRUJ osteoarthritis were identified [9]. In our case series, we similarly found that rigid internal fixation of the radial shaft alone was sufficient to maintain stability of the DRUJ. None of our patients required pinning, TFCC repair, or other surgical treatments acutely or in a delayed manner for the DRUJ, and they all had appropriate clinical and radiographic stability at final follow-up.
Traditionally proposed radiographic parameters to predict DRUJ instability in association with radial shaft fractures, including fracture location within 7.5 cm of the lunate facet or radial shortening >5 mm, have not been clinically validated. A retrospective review of 66 patients with Galeazzi injuries evaluated these parameters against intraoperative findings of DRUJ instability following radial fixation. Persistent DRUJ instability after radial shaft fixation was identified in 7 patients (11%). Neither fracture proximity to the wrist nor the degree of radial shortening reliably predicted instability: Only three of seven patients with more than 10 mm of shortening had a true DRUJ injury, and 26 fractures (39%) within 7.5 cm of the wrist were stable after fixation. However, the presence of an ulnar styloid fracture was significantly associated with instability (P = 0.02), occurring in four of seven unstable cases. These findings demonstrate that previously reported radiographic thresholds are only moderately accurate and should not be used in isolation to guide management. Instead, definitive assessment of DRUJ stability should be performed intraoperatively after anatomic reduction and fixation of the radial shaft, with consideration for stabilization or exploration only when persistent instability is demonstrated [10].
While Galeazzi fractures are relatively rare, ballistic injuries are continuing to rise in our country. Ballistics cause complex injuries due to multiple variables. The energy delivered by a ballistic to its target is dependent on the kinetic energy of the ballistic on impact, the energy of the ballistic while exiting the target, as well as the behavior of the ballistic while traveling through the target. Ballistic velocity, caliber, mass, composition, and design are all variables, and these variables can cause differences in the injury created to the target tissue [11].
Our series of patients sustained Galeazzi fractures after gunshot wounds to the forearm, which is an uncommon mechanism of injury for this fracture pattern. However, none of our patients, despite an average shortening of 10.9 mm, required further stabilization of the DRUJ after bony fixation.
To the best of our knowledge, this is the largest case series of patients who sustained Galeazzi injuries after a gunshot wounds. This is different from the typical mechanism of injury involving an axially loaded forearm with the wrist held in extension and either pronation or supination. While a ballistic Galeazzi fracture may not be extremely common, it can occur if there is disruption of the TFCC and/or the IOM. Our study suggests that these can often be managed with internal fixation of the radial shaft alone. A high index of suspicion for DRUJ injury is required during evaluation of all radial shaft fractures, including those from a ballistic mechanism.
Galeazzi fractures can occur after ballistic radial shaft fractures due to the relationship between the radius, ulna, IOM, and TFCC. A high index of suspicion is required when evaluating all radial shaft fractures, including those from a ballistic mechanism.
References
- 1. Sebastin SJ, Chung KC. A historical report on Riccardo Galeazzi and the management of Galeazzi fractures. J Hand Surg Am 2010;35:1870-7. [Google Scholar] [PubMed]
- 2. Rettig ME, Raskin KB. Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-35. [Google Scholar] [PubMed]
- 3. Atesok KI, Jupiter JB, Weiss AP. Galeazzi fracture. J Am Acad Orthop Surg 2011;19:623-33. [Google Scholar] [PubMed]
- 4. Fillingham Y, Hellman M, Haughom B, Erickson B, Szatkowski J. Report of Galeazzi fracture resulting from a ballistic injury. Pol Orthop Traumatol 2014;79:5-9. [Google Scholar] [PubMed]
- 5. Lyons JG. Epidemiology of ballistic fractures in the United States: A 20-year analysis of the firearm injury surveillance study. Injury 2022;53:3663-72. [Google Scholar] [PubMed]
- 6. Tsai PC, Paksima N. The distal radioulnar joint. Bull NYU Hosp Jt Dis 2009;67:90-6. [Google Scholar] [PubMed]
- 7. Schneiderman G, Meldrum RD, Bloebaum RD, Tarr R, Sarmiento A. The interosseous membrane of the forearm: Structure and its role in Galeazzi fractures. J Trauma 1993;35:879-85. [Google Scholar] [PubMed]
- 8. Yohe NJ, De Tolla J, Kaye MB, Edelstein DM, Choueka J. Irreducible galeazzi fracture-dislocations. Hand (N Y) 2019;14:249-52. [Google Scholar] [PubMed]
- 9. Donndorff AG, Petrucelli EM, Gallucci GL, Boretto JG, Zaidenberg EE, Rellán I, et al. Galeazzi fracture-dislocations: Long-term prognosis of the distal radioulnar joint. Hand Surg Rehabil 2021;40:572-8. [Google Scholar] [PubMed]
- 10. Tsismenakis T, Tornetta P 3rd. Galeazzi fractures: Is DRUJ instability predicted by current guidelines? Injury 2016;47:1472-7. [Google Scholar] [PubMed]
- 11. Egol KA, Koval KJ, Zuckerman JD. Handbook of Fractures. Ch. 4. Gunshot Wounds. Lippincott Williams and Wilkins; 2009. Available from: https://orthopaedics.lwwhealthlibrary.com/book.aspx?bookid=898§ionid=0 [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Escherichia hermannii: A Rare Pathogen in Implant-Associated Infection Following a Type III C Open Distal Radius Fracture – A Case Report
April 1, 2026 Escherichia hermannii: A Rare Pathogen in Implant-Associated Infection Following a Type III C Open Distal Radius Fracture – A Case Report July 10, 2024 Migration of Bullet Fragment 11 Years after Initial Gunshot Wound leads to Cervical Prevertebral Abscess: A Case Report
July 10, 2024 Migration of Bullet Fragment 11 Years after Initial Gunshot Wound leads to Cervical Prevertebral Abscess: A Case Report January 6, 2019 Hoffa’s Fat Pad-associated Solitary Neurofibroma as the Cause of Anterior Knee Pain: A Case Report
January 6, 2019 Hoffa’s Fat Pad-associated Solitary Neurofibroma as the Cause of Anterior Knee Pain: A Case Report April 1, 2025 Traumatic Knee Joint Dislocation in a Total Knee Arthroplasty with Rupture of the Popliteal Artery and a Subsequent Prosthesis Change: A Case Report
April 1, 2025 Traumatic Knee Joint Dislocation in a Total Knee Arthroplasty with Rupture of the Popliteal Artery and a Subsequent Prosthesis Change: A Case Report