
Real-time navigation can improve the safety and accuracy of endoscopic excision for spinal osteoid osteoma located close to neural structures.
Dr. Ajit Hanmant Rampure, Department of Orthopaedics, Spine Unit, Dr. Babasaheb Ambedkar Memorial Hospital, Mumbai, Maharashtra, India. E-mail: ajitrampure46@gmail.com
Abstract
Introduction: Osteoid osteoma is a benign osteogenic tumor that commonly affects young individuals and may involve the posterior elements of the spine. Surgical intervention is indicated when conservative management fails. We describe a novel technique of navigation-assisted endoscopic excision for the precise and minimally invasive management of lumbar vertebral osteoid osteoma.
Case Report: A 21-year-old male presented with nocturnal low back pain for 6 months, partially relieved with non-steroidal anti-inflammatory drugs. Computed tomography revealed a well-defined nidus involving the left lamina of the L2 vertebra in close proximity to neural structures. Navigation-assisted endoscopic excision of the lesion was performed. Using a 3D C-arm-based navigation system, precise localization and trajectory planning were achieved. Complete en bloc excision of the nidus was performed endoscopically with preservation of surrounding bony and neural structures. The patient experienced immediate post-operative pain relief and was discharged on post-operative day 1. Histopathology confirmed osteoid osteoma, and no recurrence was noted at 15-month follow-up.
Conclusion: Navigation-assisted endoscopic excision offers a safe, effective, and minimally invasive alternative for spinal osteoid osteoma, allowing precise localization, reduced morbidity, and histological confirmation.
Keywords: Osteoid osteoma, navigation, endoscopy, spine, minimally invasive surgery.
Osteoid osteoma is a benign bone-forming tumor characterized by a small vascular nidus surrounded by reactive sclerosis [1]. It accounts for approximately 10% of benign bone tumors and only 1% of spinal tumors, with the lumbar spine being the most commonly involved region. The posterior elements are affected in nearly 75% of spinal cases [2]. Patients typically present with nocturnal pain relieved by non-steroidal anti-inflammatory drugs (NSAIDs). Surgical excision is indicated in patients with persistent symptoms or lesions located near neural structures. Conventional open surgery is associated with challenges such as inaccurate localization, excessive bone removal, post-operative instability, and longer recovery [3]. Minimally invasive alternatives such as radiofrequency ablation and cryoablation reduce tissue trauma but carry the risk of neural injury and do not provide histological confirmation [4,5]. We present a novel case of navigation-assisted endoscopic excision of a lumbar vertebral osteoid osteoma, highlighting the advantages of combining real-time navigation with endoscopic visualization.
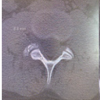
A 21-year-old previously healthy male presented with non-specific low back pain for 6 months. The pain was moderate-to-severe in intensity (Visual Analog Scale [VAS] score: 8/10), predominantly nocturnal, and partially relieved by NSAIDs. There were no radicular symptoms, neurological deficits, or constitutional symptoms. Initial radiographs and magnetic resonance imaging were inconclusive. Due to persistent symptoms and high clinical suspicion, a computed tomography (CT) scan of the spine was performed, which revealed a well-defined sclerotic lesion measuring 1 × 0.5 × 0.7 cm involving the left lamina of the L2 vertebra, with a central lucent nidus and surrounding sclerosis. Magnetic resonance imaging demonstrated hyperintense signal changes on T2-weighted images around the lesion, with adjacent neural structures located approximately 4 mm from the tumor margin. Based on clinical and radiological findings, a provisional diagnosis of osteoid osteoma was made, and the patient was planned for navigation-assisted endoscopic excision (Fig. 1 and 2).

Figure 1: Pre-operative sagittal computed tomography scan showing a well-defined nidus involving the left lamina of L2 vertebra with surrounding sclerosis.
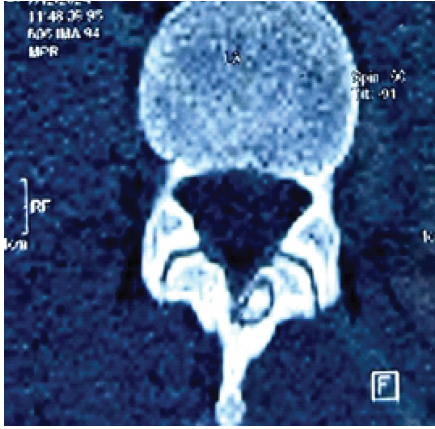
Figure 2: Pre-operative coronal computed tomography scan showing a well-defined nidus.
The procedure was performed under general anesthesia with the patient in the prone position. A 3D C-arm scan of the lumbar spine was obtained and transferred to the Brainlab navigation system. A reference array was securely fixed to the L2 spinous process, and accurate registration was confirmed (Fig. 3).
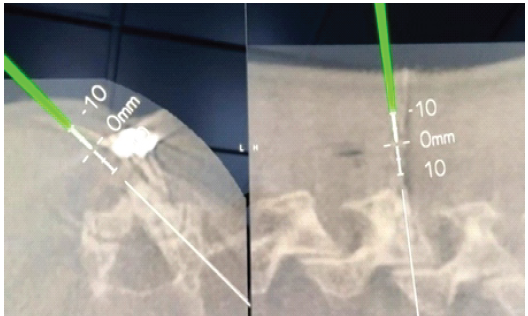
Figure 3: Intraoperative navigation screenshot showing planned trajectory toward the lesion using a 3D navigation system.
Using a navigated probe, a precise trajectory was planned to approach the left lamina of L2 from the contralateral (right) side to minimize the risk to neural structures. A 1-cm skin incision was made, followed by serial dilation and placement of the endoscopic working cannula. Under endoscopic visualization, soft tissues were cleared to expose the base of the spinous process. A navigation-guided burr was used to drill along the preplanned trajectory through the spinous process and lamina. Granulation tissue and the nidus were identified and excised en bloc. Radiofrequency ablation of the margins was performed to minimize the risk of recurrence. Complete excision was confirmed endoscopically (Fig. 4 and 5). The wound was closed in layers, and the patient was mobilized on the same day.
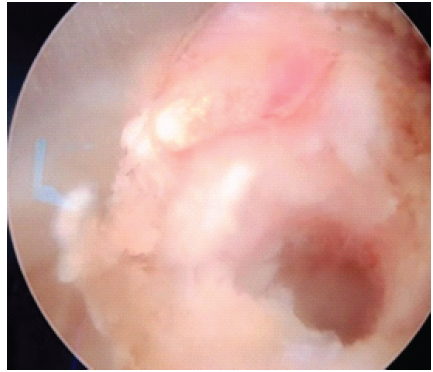
Figure 4: Endoscopic intraoperative view showing exposure of the nidus after bony drilling.
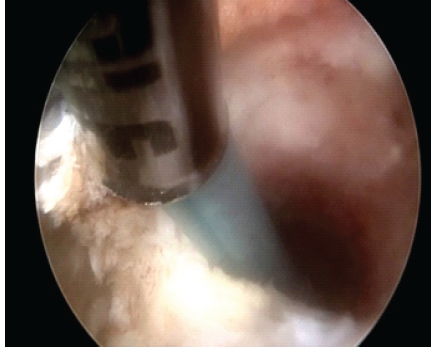
Figure 5: Endoscopic view after complete excision of the nidus.
The patient experienced immediate post-operative pain relief, with a VAS score improvement from 8/10 to 3/10. He was discharged on post-operative day 1 without complications. Post-operative CT scan confirmed complete excision of the nidus. At 6- and 12-month follow-up, the patient remained symptom-free with no recurrence (Fig. 6 and 7).

Figure 6: Post-operative sagittal scan confirming complete excision of the lesion.

Figure 7: Post-operative sagittal and axial computed tomography scan.
At the latest follow-up of 15 months, he continued to be asymptomatic with no radiological evidence of recurrence. Histopathological examination confirmed the diagnosis of osteoid osteoma with no evidence of malignancy (Fig. 8).
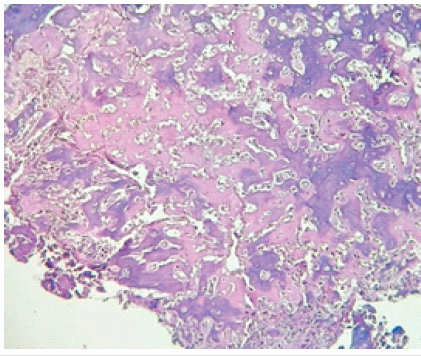
Figure 8: Histopathology showing interlacing trabeculae of woven bone with osteoblastic rimming, confirming osteoid osteoma (Hematoxylin and Eosin stain).
Surgical management of spinal osteoid osteoma aims to achieve complete excision of the nidus while preserving spinal stability and protecting neural structures [6]. Traditional open approaches often require extensive bone removal and are associated with increased morbidity [7]. Minimally invasive modalities such as radiofrequency ablation and cryoablation offer reduced tissue damage but lack histological confirmation and carry a risk of thermal injury to adjacent neural structures [8]. Navigation-assisted endoscopic excision combines the advantages of real-time three-dimensional navigation with direct endoscopic visualization [9]. This technique allows precise localization of the lesion, accurate trajectory planning, minimal bony resection, and preservation of spinal stability [9,10]. In addition, it provides histopathological confirmation, which is not possible with ablative techniques [11]. Previous reports have demonstrated the feasibility of navigation-assisted and endoscopic techniques for spinal osteoid osteoma [11,12]. Our case further supports the safety and efficacy of this combined approach, particularly for lesions located close to neural structures.
Navigation-assisted endoscopic excision is a safe, effective, and minimally invasive technique for the treatment of lumbar vertebral osteoid osteoma. It enables precise localization, complete excision, minimal morbidity, and rapid recovery, making it a valuable alternative to conventional open surgery and percutaneous ablative techniques.
Navigation-assisted endoscopic excision offers a safe and precise minimally invasive option for spinal osteoid osteoma adjacent to neural structures, preserving stability and enabling histological confirmation.
References
- 1. Zhang Y, Rosenberg AE. Bone-forming tumors. Surg Pathol Clin 2017;10:513-35. [Google Scholar] [PubMed]
- 2. Cové JA, Taminiau AH, Obermann WR, Vanderschueren GM. Osteoid osteoma of the spine treated with percutaneous computed tomography-guided thermocoagulation. Spine (Phila Pa 1976) 2000;25:1283-6. [Google Scholar] [PubMed]
- 3. Motamedi D, Learch TJ, Ishimitsu DN, Motamedi K, Katz MD, Brien EW, et al. Thermal ablation of osteoid osteoma: Overview and step-by-step guide. Radiographics 2009;29:2127-41. [Google Scholar] [PubMed]
- 4. Parmeggiani A, Martella C, Ceccarelli L, Miceli M, Spinnato P, Facchini G. Osteoid osteoma: Which is the best mininvasive treatment option? Eur J Orthop Surg Traumatol 2021;31:1611-24. [Google Scholar] [PubMed]
- 5. Amendola L, Cappuccio M, Boriani L, Gasbarrini A. Endoscopic excision of C2 Osteoid Osteoma: A technical case report. Eur Spine J 2012;22 Suppl 3:S357-62. [Google Scholar] [PubMed]
- 6. Mallepally AR, Mahajan R, Pacha S, Rustagi T, Marathe N, Chhabra HS. Spinal osteoid osteoma: Surgical resection and review of literature. Surg Neurol Int 2020;11:308. [Google Scholar] [PubMed]
- 7. Migiel M, Brynczka I, Siuta N, Rypel-Bośka J, Miaśnikiewicz J, Goleniewska K, et al. Osteoid osteoma – a literature review. Qual Sport 2025;47:66808. [Google Scholar] [PubMed]
- 8. Cerny J, Soukup J, Cerna S, Novotny T. Current approaches to osteoid osteoma and minimally invasive surgery-a minireview and a case report. J Clin Med 2022;11:5806. [Google Scholar] [PubMed]
- 9. Liu R, Tian J, Yuan J, Zhao B, Xu C, Wang Y. Computer‐assisted navigation full visualization spinal endoscopic surgery for lumbar vertebral osteoid osteoma. Orthop Surg 2023;15:2464-70. [Google Scholar] [PubMed]
- 10. Alyousef YM, Aleissa SI, Konbaz F, Helal F, Abaalkhail M. Navigation assisted cervical spine osteoid osteoma excision: A case report. Int J Adv Res 2023;11:953-8. [Google Scholar] [PubMed]
- 11. Liawrungrueang W, Cholamjiak W, Sunpaweravong S, Sarasombath P. Full-endoscopic pedicle-based approach for resection of osteoid osteoma in the lumbar spine: A case report and review of current literature. J Spine Surg 2023;11:1167-74. [Google Scholar] [PubMed]
- 12. Shin Y, Sunada H, Shiraishi Y, Hosokawa M, Koh Y, Tei R, et al. Navigation-assisted full-endoscopic spine surgery: A technical note. J Spine Surg 2020;6:513-20. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Unusual Presentation of Spinal Osteoid Osteoma: A Case Report
April 1, 2026 Unusual Presentation of Spinal Osteoid Osteoma: A Case Report October 1, 2025 Glomus Tumour of Sciatic Nerve – A Rare Presentation Mimicking Sciatica
October 1, 2025 Glomus Tumour of Sciatic Nerve – A Rare Presentation Mimicking Sciatica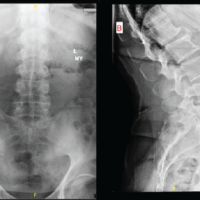 March 1, 2025 Full Endoscopic Resection of Giant Synovial Cyst in the Lumbar Spine: A Case Report
March 1, 2025 Full Endoscopic Resection of Giant Synovial Cyst in the Lumbar Spine: A Case Report August 6, 2024 Minimally Invasive Resection of a Lumbar Spine Vertebral Osteoid Osteoma: A Case Report
August 6, 2024 Minimally Invasive Resection of a Lumbar Spine Vertebral Osteoid Osteoma: A Case Report