
Early CT-based diagnosis and anatomical fixation are critical for restoring knee joint congruity in medial Hoffa’s fractures. This series highlights varied presentations and management approaches to optimize patient outcomes.
Dr. Parimal Vairagade, Department of Orthopaedic Surgery, NKP Salve Institute of Medical Sciences, Nagpur, Maharashtra, India. E-mail: pvairagade01@gmail.com
Abstract
Introduction: Medial Hoffa’s fractures are rare coronal plane fractures of the distal femur, often missed on initial radiographs. Early diagnosis and anatomical fixation are essential for good functional recovery.
Case Report: We present three cases of medial Hoffa’s fracture in adult patients following high-energy trauma. All were diagnosed using computed tomography scans. Surgical fixation was performed using headless compression screws through a subvastus approach. Post-operative rehabilitation protocols varied slightly, but all patients achieved satisfactory union and function by 6–9 months.
Conclusion: High suspicion, advanced imaging, and stable fixation are vital for optimal outcomes in medial Hoffa’s fractures. Consistent anatomical reduction across cases resulted in excellent functional recovery.
Keywords: Medial Hoffa’s fracture, distal femur, coronal fracture, internal fixation, subvastus approach.
Medial Hoffa’s fractures, first described by Albert Hoffa in 1904, are extremely rare injuries involving the coronal plane of the medial femoral condyle [1,2,3]. They typically result from high-energy trauma such as road traffic accidents and may be missed on plain radiographs [4,5,6,7]. Untreated or malreduced fractures can lead to poor outcomes due to articular incongruity and instability [5,8,9].
Case 1: A 35-year-old male sustained a high-energy road traffic accident and presented with knee swelling, medial joint line tenderness, and restricted range of motion. Initial radiographs demonstrated a subtle coronal fracture line of the medial femoral condyle (Fig. 1).
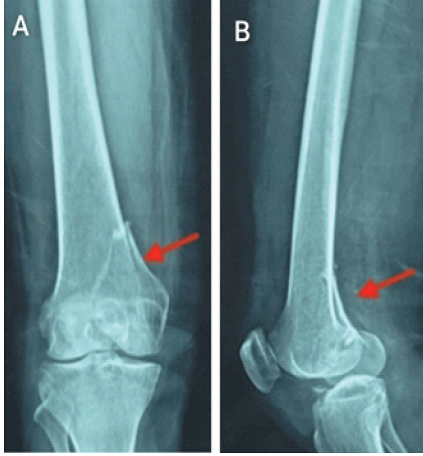
Figure 1: Pre-operative magnetic resonance imaging – Axial T1-weighted (left) and sagittal T2-weighted fat-saturated (T2w FS) (right). Left: A large, well-circumscribed lobulated cystic mass occupies the anterodorsal compartment, homogeneously hyperintense on T1-weighting, consistent with a fluid-filled ganglion of the tibialis anterior tendon sheath measuring 4.4 × 3.9 × 11.7 cm. Right: The sagittal T2w FS sequence demonstrates the full craniocaudal extent (~11.7 cm) of the lobulated hyperintense ganglion cyst, intimately associated with the tibialis anterior tendon as it courses toward its insertion on the medial cuneiform.
Computed tomography (CT) imaging confirmed an isolated medial Hoffa’s fracture without comminution (Fig. 2).
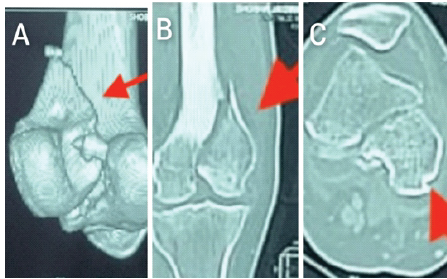
Figure 2: Intraoperative photograph – initial cyst exposure – Following anterior longitudinal elliptical incision over the left dorsal ankle, the large multilobulated ganglion cyst herniates through the wound, displaying its characteristic pearly-white, smooth, translucent, multilobulated appearance consistent with the septated morphology demonstrated on pre-operative magnetic resonance imaging. The extensor retinaculum is retracted using retractors.
The fracture was managed surgically using a medial parapatellar approach, and fixation was achieved with two anterior-to-posterior headless compression screws. Post-operative radiographs demonstrated anatomical reduction and stable fixation (Fig. 3).

Figure 3: Intraoperative photograph – tibialis anterior tendon pathology and tubularization – Following cyst decompression and evacuation of its mucinous contents, the underlying tibialis anterior tendon is exposed, revealing multiple longitudinal degenerative tears (~4 cm in length, located 1 cm proximal to the medial cuneiform insertion) with splaying and fraying of tendon fibers. The patulous, redundant tendon sheath is clearly visible. Vicryl 4-0 sutures have been placed in preparation for tubularization to restore the cylindrical architecture of the tendon.
At 6-month follow-up, the patient achieved a painless knee range of motion from 0° to 120° with radiological evidence of union.
Case 2: A 42-year-old female sustained a fall from height and presented with swelling, medial knee pain, and inability to bear weight. Plain radiographs suggested a minimally displaced medial condylar fracture (Fig. 4).

Figure 4: Post-surgical sagittal post-contrast magnetic resonance imaging (approximately 4 weeks post-operative) – Diffuse enhancement of the anterior ankle soft tissues consistent with cellulitis. The ATT tendon sheath collection extends proximally to surround the myotendinous junction with intramuscular extension and irregularly thickened, enhancing walls consistent with an infective collection. A subcentimeter susceptibility focus is identified in the subdermal layer adjacent to the ATT, raising suspicion for a retained foreign body that is radiographically occult on plain radiographs.
CT scan confirmed a medial Hoffa’s fracture with minimal displacement (Fig. 5).
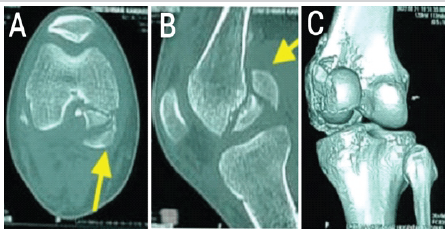
Figure 5: Computed tomography scan showing fracture pattern – case 2.
Open reduction and internal fixation were performed through a medial parapatellar approach using three cannulated screws to enhance stability. Post-operative radiographs confirmed satisfactory fixation (Fig. 6).
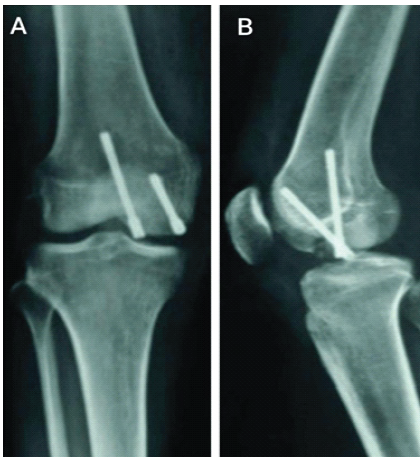
Figure 6: Post-operative radiograph – case 2.
The patient was allowed progressive weight-bearing and achieved a knee range of motion of 0°–125° at 7 months.
Case 3: A 28-year-old male sustained a motorcycle accident and presented with knee effusion and medial joint line tenderness. Radiographs demonstrated a medial condylar fracture (Fig. 7), and CT imaging revealed a comminuted medial Hoffa’s fracture (Fig. 8).
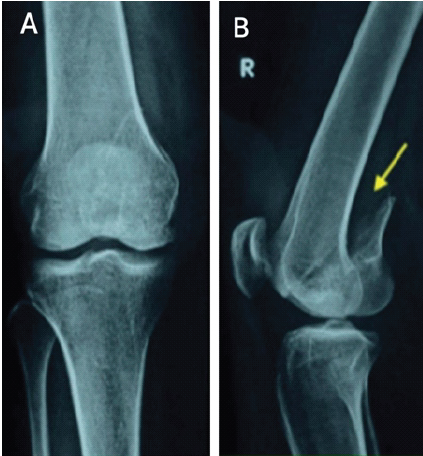
Figure 7: Pre-operative X-ray showing anteroposterior and lateral radiographs – case 3.
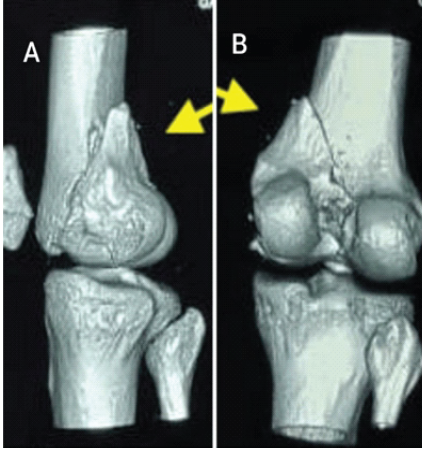
Figure 8: Computed tomography scan showing comminution – case 3.
Due to comminution, anatomical reduction was supplemented with screw fixation and plate augmentation to resist shear forces. Post-operative radiographs confirmed stable fixation (Fig. 9). Fracture union was achieved by 5 months, and the patient returned to pre-injury activity levels by 9 months.
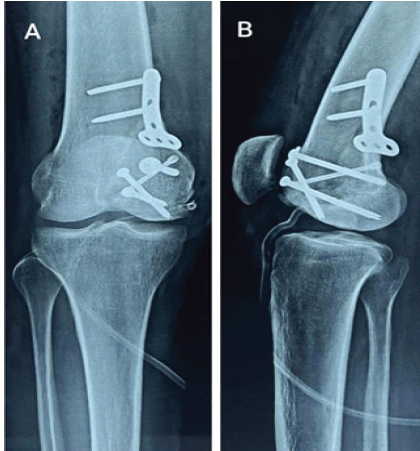
Figure 9: Post-operative radiograph with plate augmentation – case 3.
Medial Hoffa’s fractures are an uncommon subset of distal femur fractures [1,2,3], representing a coronal plane injury that can be easily missed on standard anteroposterior and lateral radiographs. Their rarity, combined with subtle presentation, often delays diagnosis [5,6]. These fractures typically occur due to high-energy mechanisms such as road traffic accidents or falls from height, where an axial load is transmitted through a flexed knee [4,6,7]. The resultant shear forces across the condyles cause intra-articular separation, which, if left untreated or inadequately fixed, may result in joint incongruity, instability, and early post-traumatic arthritis. CT imaging plays a pivotal role in identifying fracture orientation, degree of displacement, and associated comminution, allowing precise surgical planning [6,7,10]. Our case series highlights that, irrespective of patient age or fracture pattern, surgical management remains the gold standard [5,11,10]. The choice of surgical approach depends on the condyle involved: A medial parapatellar or subvastus approach provides optimal visualization for medial condyle fractures [12], while a lateral parapatellar approach is suited for lateral condyle injuries. Bicondylar variants may require combined exposures. In our series, fixation with headless or cannulated screws ensured rigid stability, while plate augmentation was valuable in the comminuted case to resist shear forces and prevent collapse [5,10]. Early mobilization was possible in all cases due to the stable constructs, which is critical in preserving knee range of motion and preventing stiffness. The outcomes reinforce that meticulous anatomical reduction, stable fixation, and a structured rehabilitation protocol are the cornerstones for achieving pain-free function and avoiding long-term degenerative changes. Several previous studies have described unicondylar femoral fractures and their management strategies [13,14,15,16].
Hoffa fractures of the distal femur are rare, high-energy injuries involving the coronal plane of one or both condyles. They are often missed during routine assessment and demand a high index of suspicion, especially in patients with axial load on a flexed knee. CT imaging should be used to confirm the diagnosis and plan surgical management [6,7,10]. Non-operative treatment is rarely indicated; the current standard is open reduction and internal fixation, using approaches tailored to the condyle involved. Appropriate fixation with screws and plate augmentation when required ensures anatomical reduction, joint stability, and favorable long-term outcomes.
Medial Hoffa’s fractures, though rare, must be actively ruled out in all high-energy distal femur injuries. CT imaging is crucial for diagnosis, and timely anatomical fixation – preferably with screws and plate augmentation if needed – ensures joint stability, prevents arthritis, and restores full function.
References
- 1. Smith EJ, Crichlow TP, Roberts PS. Monocondylar fractures of the femur: A review of 13 patients. Injury 1989;20:371-4. [Google Scholar] [PubMed]
- 2. Kolmert L, Wulff K. Epidemiology and treatment of distal femoral fractures in adults. Acta Orthop Scand 1982;53:957-62. [Google Scholar] [PubMed]
- 3. Nordin JY, Masquelet AC, Gavard R, Signoret F. Unicondylar fractures of the femur: reflections based on a series of 90 cases. Rev Chir Orthop Reparatrice Appar Mot. 1985;71:111–115 [Google Scholar] [PubMed]
- 4. Alam N, Siddiqui YS, Abbas M, Akshay V. Buttress plate assisted fixation for bicondylar hoffa fracture: A missed fracture-case report with review of literature. J Orthop Case Rep 2022;12:75-9. [Google Scholar] [PubMed]
- 5. Manfredini M, Gildone A, Ferrante R, Bernasconi S, Massari L. Unicondylar femoral fractures: Therapeutic strategy and long-term results. A review of 23 patients. Acta Orthop Belg 2001;67:132-8. [Google Scholar] [PubMed]
- 6. Patel PB, Tejwani NC. The Hoffa fracture: Coronal fracture of the femoral condyle a review of literature. J Orthop 2018;15:726-31. [Google Scholar] [PubMed]
- 7. Zhou Y, Pan Y, Wang Q, Hou Z, Chen W. Hoffa fracture of the femoral condyle: Injury mechanism, classification, diagnosis, and treatment. Medicine (Baltimore) 2019;98:e14633. [Google Scholar] [PubMed]
- 8. Kennedy JC, Grainger RW, McGraw RW. Osteochondral fractures of the femoral condyles. J Bone Joint Surg Br 1966;48:436-40. [Google Scholar] [PubMed]
- 9. Ostermann PA, Neumann K, Ekkernkamp A, Muhr G. Long term results of unicondylar fractures of the femur. J Orthop Trauma 1994;8:142-6. [Google Scholar] [PubMed]
- 10. Viskontas DG, Nork SE, Barei DP, Dunbar R. Technique of reduction and fixation of unicondylar medial Hoffa fracture. Am J Orthop (Belle Mead NJ) 2010;39:424-8. [Google Scholar] [PubMed]
- 11. Helfet DL. Fratture monocondiloidee di femore. In: Browner BD. editor. Traumatologia Deall’apparato Muscolo-Scheletrico. Vol. 4. Roma: Verduci Editore; 1994. p. 1721-1736 [Google Scholar] [PubMed]
- 12. Berstock JR, Murray JR, Whitehouse MR, Blom AW, Beswick AD. Medial subvastus versus the medial parapatellar approach for total knee replacement: A systematic review and meta-analysis of randomized controlled trials. EFORT Open Rev 2018;3:78-84. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series
August 1, 2026 Clinical and Functional Outcomes of Posterior Cruciate Ligament Tibial Avulsion Fractures Treated with a Mini-Open Posterior Approach and Internal Fixation: A Case Series August 1, 2026 Functional and Cosmetic Outcome in Vertical Midline versus Horizontal Curvilinear Patella-Centered Incision in Internal Fixation of Patellar Fractures
August 1, 2026 Functional and Cosmetic Outcome in Vertical Midline versus Horizontal Curvilinear Patella-Centered Incision in Internal Fixation of Patellar Fractures July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report
July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone
July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone