
The main learning point of this article is to illustrate interesting and effective management by the orthopedic trauma team to manage a rare injury.
Guillermo Rodriguez, Department of Orthopaedic Surgery and Sports Medicine, Detroit Medical Center, Detroit, Michigan, USA; Wayne State University School of Medicine, Detroit, Michigan, USA. E-mail: guillermo0390@gmail.com
Abstract
Introduction: Occipital condyle fractures (OCFs) are rare injuries presenting with neurologic sequelae that may be debilitating or even fatal. Treatment options for unstable OCFs include fusion or halo placement. Fusion of the occipitocervical junction is associated with a significant loss of motion.
Case Report: This study presents a case of bilateral occipital condylar fractures with C1-C2 rotatory subluxation treated with temporary fusionless occipitocervical fixation.
Conclusion: This is a rare case of bilateral OCFs with atlantoaxial instability that underwent fusionless instrumentation and subsequent hardware removal. Treatment resulted in excellent radiographic and clinical outcomes regarding pain and motion at the most recent follow-up.
Keywords: Occipital condylar fracture, occipitocervical junction, fusion, unstable cervical spine, atlantoaxial instability, open reduction, temporary fixation.
Occipital condyle fractures (OCFs) are uncommon, comprising about 1–3% of high-energy trauma to the head and neck and affecting the integrity of the craniocervical junction (CCJ) [1,2,3,4,5,6]. Ligamentous attachments to the occipital condyles support craniocervical stability. The alar ligaments originate from the dens and insert onto the occipital condyles. They act in tandem to limit lateral rotation and tilt, leading to instability of the CCJ if disrupted. It is critical to stratify the stability of these injuries as they are at risk for spinal cord injury with resulting neurologic deficits [5,6,7,8].
This injury resulted in bilateral occipital condyle avulsion fractures. Anderson and Montesano classified this as a type III injury [6,7]. In most unilateral OCFs, conservative management is indicated because the occipitocervical junction remains relatively stable; however, in cases of bilateral avulsion, the increased potential for atlantoaxial stability requires more extensive management [6,9,10].
This study describes a rare presentation of bilateral OCFs managed with occipitocervical instrumentation without fusion for the goal of motion presentation versus the gold standard of arthrodesis or fusion. Once the fractures healed, the construct was removed. The patient ultimately regained a full painless range of motion of the cervical spine. This case was documented with consent by the patient that it would be submitted for publication.
Patient is an 18-year-old male who presented to the emergency department through ambulance following a high-speed motorcycle crash. On arrival, the Glasgow Coma Scale was 14. A rigid cervical collar had been placed by emergency medical services. There were deformities of his left thigh and left forearm, and he reported cervical spine tenderness. Neurological examination revealed intact motor strength and sensation of his bilateral upper and left lower extremities. Examination of the right lower extremity revealed motor weakness with grade 1 out of 5 strength for ankle dorsiflexion, great toe extension, and ankle plantarflexion. Sensation was decreased over the L4, L5, and S1 compared to the contralateral extremity.
A computed tomography (CT) scan of the cervical spine demonstrated bilateral occipital condyle avulsion fractures with atlantoaxial rotatory subluxation (Fig. 1a, b, c, d).
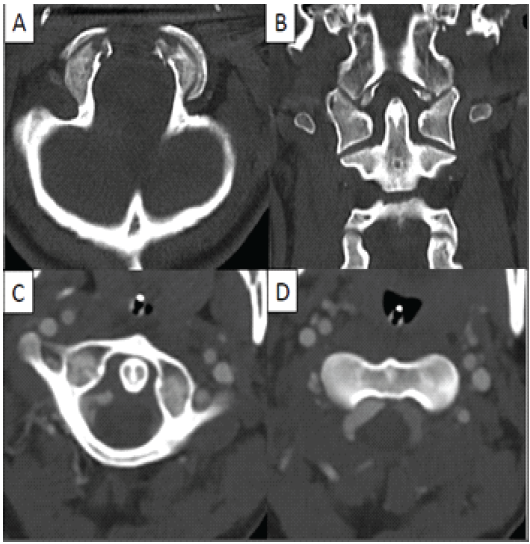
Figure 1: Computed tomography scan of the cervical spine showing bilateral occipital condyle avulsion fractures on the axial (a) and coronal cuts (b) with associated atlantoaxial (C1-C2) rotatory subluxation (c and d).
Other injuries included an unstable pelvic ring injury, bilateral acetabular fractures, open left midshaft femur fracture, closed left clavicle fracture, closed left upper extremity and hand fractures.
The patient was admitted to the surgical intensive care unit (ICU) with strict spine pre-cautions and instructions to maintain his cervical collar at all times. Three days after the initial injury, the patient was taken to the operating room to address his cervical spine injury. Once in the operating room, general anesthesia was induced, and then biotronic monitoring was placed for electromyography (EMG), somatosensory evoked potential (SSEP), and motor evoked potential (MEP). Gardner-Wells tongs were placed, and the patient was subsequently positioned prone on the Orthopedic Systems Inc. spine frame. The bookwalter retractor system and radiolucent Hohmann retractors were then used during exposure. After obtaining posterior exposure of the occiput to C3, lateral mass screws were placed in C3 and pedicle screws in C2 using fluoroscopic imaging. An occipital plate was then placed with three screws. The construct was connected to the cervical screws with two curved rods and tightened. Final fluoroscopic images were obtained to confirm appropriate hardware placement. Post-operative radiographs are shown in Fig. 2.
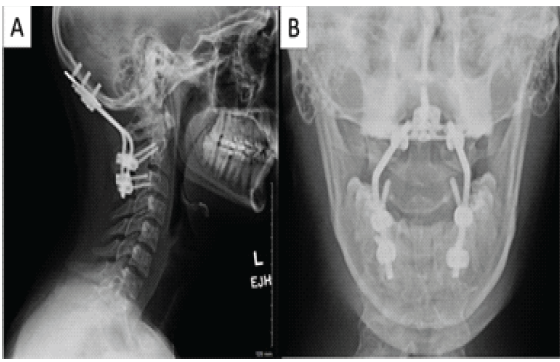
Figure 2: Post-operative lateral c-spine (a) and open-mouth odontoid (b) radiographs showing the occipital to C2-3 fixation.
The incision was subsequently closed, and sterile dressings were applied. MEPs and SSEPs were normal throughout the case. The patient was placed in a cervical collar and returned to the surgical ICU in stable condition.
Post-operative course was unremarkable, and the patient underwent rehabilitation for his other orthopedic injuries while remaining in a cervical collar. Post-operative visits demonstrated intact occipitocervical hardware with interval fracture healing. Neurologic examination remained unchanged, with motor and sensory deficits of his right lower extremity due to a peripheral sciatic nerve injury confirmed on EMG. Examination of the cervical spine showed a limited range of motion in all planes.
A CT scan of the cervical spine performed 10 months post-operatively demonstrated well-healed OCFs and maintained reduction of the atlanto-occipital and atlantoaxial articulations (Fig. 3).
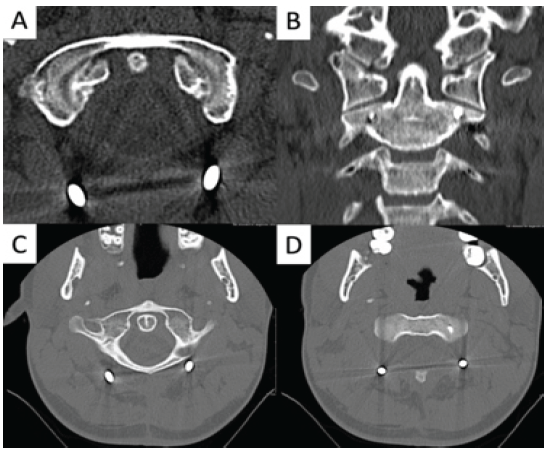
Figure 3: Computed tomography of the cervical spine, 10 months from the initial surgery, showing healed bilateral occipital condyle avulsion fractures (a and b) without atlantoaxial rotatory subluxation (c and d).
Due to complaints of limited cervical motion, the decision was made to remove the occipitocervical hardware to improve his mobility. One year after his initial surgery, the patient underwent removal of the occipital plate, cervical screws, and connecting rods (Fig. 4).
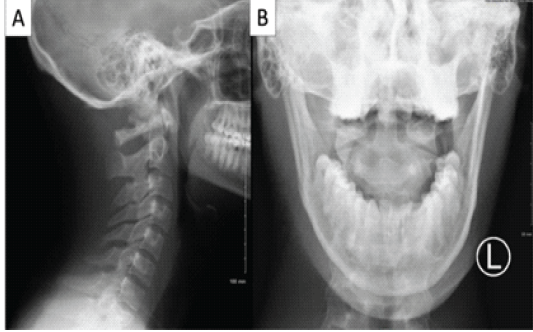
Figure 4: Post-operative lateral c-spine (a) and open-mouth odontoid views (b) radiographs following hardware removal.
Post-operatively, the patient remained stable without changes in his neurologic status and was discharged to home. At 4 weeks following removal of hardware, and approximately 13 months from the original trauma, the patient had regained full pain-free range of motion of the cervical spine (Fig. 5). He was pleased with the outcome, with plans to return to work.
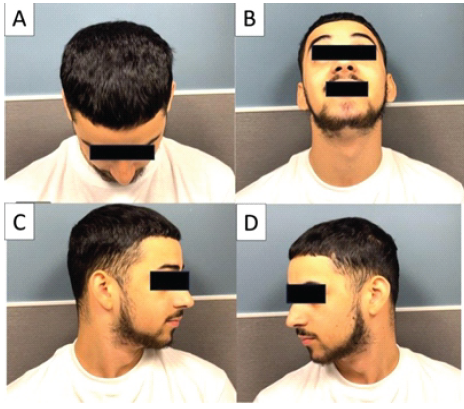
Figure 5: Patient 13 months out from initial injury, and 4 weeks from removal of occipitocervical instrumentation. Clinical pictures demonstrating full cervical range of motion in both flexion (a), extension (b), and axial rotation (c and d).
The CCJ is stabilized by the alar ligaments, the occipital condyle joint capsules, and the tectorial membrane. Fractures of the occipital condyles can result in severe instability, leading to neurologic deficits in over a third of affected patients [2,4,8]. Established recommendations to guide treatment of OCFs are limited [2,3,5,7,8,9].
Accepted classification systems consider the biomechanics, anatomy, and fracture morphology of the CCJ and define stable versus unstable injuries [5,6,7]. Anderson and Montesano stratify OCFs as Types 1 and 2, being stable with intact alar ligaments and tectorial membrane. Conversely, Type 3 OCFs, according to the above classification, include avulsion of the occipital condyle and thus injury to the alar ligament, suggesting fracture instability [7]. Tuli et al. established treatment stratification based on the structural integrity of OCFs that provides recommendations for management. They postulate that the need for open instrumentation of OCFs is dictated by the presence of craniocervical misalignment or occipitoatlantoaxial instability [5].
Bilateral OCFs are not addressed in existing classification systems. This is an uncommon presentation, which in cases of avulsion fractures, atlanto-occipital dissociation is likely to be present and must be evaluated carefully [8,10]. Notably, authors discussing treatment of bilateral avulsion of the occipital condyles have described that the concomitant disruption of the alar ligaments due to this fracture pattern results in CCJ instability [6,8,11,12,13,14]. It follows that rigid cervical immobilization is recommended for bilateral OCFs in the form of internal or external fixation; although, there is insufficient evidence in the literature to determine which type of intervention is more appropriate [2 3 5,8].
Isolated case reports report successful closed treatment of CCJ fracture patterns that include the bilateral occipital condyles, among other structures. Patients were subject to 12–18 weeks of rigid external stabilization with a halo vest [15,16,17]. Open treatment for these injuries has also been successful, consisting of O-C1 or O-C2 posterior occipitocervical fusion in a few cases [14,18,19,20,21].
When considering surgical intervention, CCJ instability is a primary indication for posterior occipitocervical fusion in adults – resulting in immediate post-operative stability [22,23]. However, young active adults who undergo posterior fusion typically have a significant decrease in range of motion, translating to long-term functional limitation and a decreased quality of life [22,23,24]. Furthermore, while a halo vest is effective in limiting cervical motion, common concerns include increased patient discomfort caused by the external apparatus, lack of mobility, and risk of pin site infection or loosening. In addition, contraindications to the use of a halo vest include polytrauma, chest trauma, obesity, scalp injury, and infection [25,26]. Alternatively, a rigid collar is easily placed and does not possess operative morbidity, but immobilization of the cervical spine is limited as compared with surgical stabilization or even a halo vest [25,27].
In the case presented, bilateral OCFs were successfully managed with temporary occipitocervical fixation without fusion, followed by hardware removal. Instrumentation and fixation were performed to provide stability to the fractures, allowing for bony union through callus formation. Preservation of motion upon removal of hardware is of significant benefit, as O-C2 joints are responsible for most of the flexion-extension and rotational motion of the neck when compared to subaxial levels. This is imperative as fusion of the higher cervical levels may be associated with a decreased quality of life and a significant loss of motion of the cervical spine [26,28,29]. While this technique has not been applied to bilateral OCFs in literature, temporary bridge fixation to address unstable atlas or odontoid fractures has yielded solid bone union, high levels of patient satisfaction, and resulted in preserved neck motion [30,31,32,33,34,35].
OCFs are rare injuries that may compromise the stability of the CCJ. Clinical presentation varies among patients, with up to a third resulting in neurologic deficits. Literature recommends surgical intervention in the form of occipitocervical fusion or halo vest immobilization for unstable injuries with associated atlanto-occipital instability. This case report demonstrates a motion-preserving technique for unstable bilateral OCFs. Fracture healing was accomplished using a temporary occipitocervical construct, with return of full cervical motion upon hardware removal. Further investigation is warranted to determine the most optimal protocol to address bilateral OCFs, as recommendations are not yet provided in present clinical guidelines.
This article describes the decision-making that resulted in the successful novel treatment to address an otherwise debilitating injury of unstable bilateral occipital condylar fractures with temporary fixation.
References
- 1. 1 Mueller FJ, Fuechtmeier B, Kinner B, Rosskopf M, Neumann C, Nerlich M, et al. Occipital condyle fractures. Prospective follow-up of 31 cases within 5 years at a level 1 trauma centre. Eur Spine J 2012;21:289-94. [Google Scholar] [PubMed]
- 2. 2 Hanson JA, Deliganis AV, Baxter AB, Cohen WA, Linnau KF, Wilson AJ, et al. Radiologic and clinical spectrum of occipital condyle fractures: Retrospective review of 107 consecutive fractures in 95 patients. AJR Am J Roentgenol 2002;178:1261-8. [Google Scholar] [PubMed]
- 3. 3 Vaccaro AR, Lim MR, Lee JY. Indications for surgery and stabilization techniques of the occipito-cervical junction. Injury 2005;36 Suppl 2:B44-53. [Google Scholar] [PubMed]
- 4. 4 Karam YR, Traynelis VC. Occipital condyle fractures. Neurosurgery 2010;66 Suppl 3:56-9. [Google Scholar] [PubMed]
- 5. 5 Tuli S, Tator CH, Fehlings MG, Mackay M. Occipital condyle fractures. Neurosurgery 1997;41:368-76; discussion 376-7. [Google Scholar] [PubMed]
- 6. 6 Maserati MB, Stephens B, Zohny Z, Lee JY, Kanter AS, Spiro RM, et al. Occipital condyle fractures: Clinical decision rule and surgical management. J Neurosurg Spine 2009;11:388-95. [Google Scholar] [PubMed]
- 7. 7 Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine (Phila Pa 1976) 1988;13:731-6. [Google Scholar] [PubMed]
- 8. 8 Kalani MY, Filippidis AS, Theodore N. Injuries to the cervical spine. In: Ellenbogen RG, Abdulrauf SI, Sekhar N, editors. Principles of Neurological Surgery. Netherlands: Elsevier; 2012. p. 397-411. [Google Scholar] [PubMed]
- 9. 9 Mead LB 2nd, Millhouse PW, Krystal J, Vaccaro AR. C1 fractures: A review of diagnoses, management options, and outcomes. Curr Rev Musculoskelet Med 2016;9:255-62. [Google Scholar] [PubMed]
- 10. 10 Batista AV, Aguiar GB, Bennett P, Umigi MR, Veiga JC. Observational study of patients with occipital condyle fracture at a Brazilian referral trauma center. Rev Col Bras Cir 2021;48:e20213024. [Google Scholar] [PubMed]
- 11. 11 Werne S. Studies in spontaneous atlas dislocation. Acta Orthop Scand Suppl 1957;28 Suppl 23:3-150. [Google Scholar] [PubMed]
- 12. 12 Aljuboori Z, Sharma M, Andaluz N. Contemporaneous avulsion fractures of the inferior clivus and bilateral occipital condyles with injury of the tectorial membrane. Surg Neurol Int 2020;11:11. [Google Scholar] [PubMed]
- 13. 13 Bellabarba C, Mirza SK, West GA, Mann FA, Dailey AT, Newell DW, et al. Diagnosis and treatment of craniocervical dislocation in a series of 17 consecutive survivors during an 8-year period. J Neurosurg Spine 2006;4:429-40. [Google Scholar] [PubMed]
- 14. 14 Persad AR, Liu E, Wu A, Fourney DR. Bilateral occipital condyle fracture with an avulsion fracture of the foramen magnum: Nonoperative care guided by a traction test. Illustrative case. J Neurosurg Case Lessons 2023;6:CASE23577. [Google Scholar] [PubMed]
- 15. 15 Dashti R, Ulu MO, Albayram S, Aydin S, Ulusoy L, Hanci M. Concomitant fracture of bilateral occipital condyle and inferior clivus: What is the mechanism of injury? Eur Spine J 2007;16:261-4. [Google Scholar] [PubMed]
- 16. 16 Chan JL, Cohen JD, Rahman SU, Perry TG, Tuchman A. Motion preserving management of unstable traumatic clivus fracture extending through bilateral occipital condyles. J Clin Neurosci 2020;80:257-60. [Google Scholar] [PubMed]
- 17. 17 Tanabe, M, Watanabe T, Matsumoto S, Okamoto H, Shirakashi K. Avulsion fracture of the anterior half of the foramen magnum involving the bilateral occipital condyles and the inferior clivus–case report. Neurol Med Chir (Tokyo) 1999;39:358-61. [Google Scholar] [PubMed]
- 18. 18 Maughan PH, Horn EM, Theodore N, Feiz-Erfan I, Sonntag VK. Avulsion fracture of the foramen magnum treated with occiput-to-c1 fusion: Technical case report. Neurosurgery 2005;57:E600. [Google Scholar] [PubMed]
- 19. 19 Fuentes S, Bouillot P, Dufour H, Grisoli F. Occipital condyle fractures and clivus epidural hematoma. Case report. Neurochirurgie 2000;46:563-7. [Google Scholar] [PubMed]
- 20. 20 Jones DN, Knox AM, Sage MR. Traumatic avulsion fracture of the occipital condyles and clivus with associated unilateral atlantooccipital distraction. AJNR Am J Neuroradiol 1990;11:1181-3. [Google Scholar] [PubMed]
- 21. 21 Lam KS, Carriço G, Fernandes FM, Nanni F, De La Torre Escobar C. A rare case of bilateral occipital condyle fractures associated with inferior clivus separation fracture resulting in craniocervical dislocation: A case report and modification of the Anderson and Montesano classification is proposed. Acta Neurochir (Wien) 2021;163:2307-11. [Google Scholar] [PubMed]
- 22. 22 Lieberman IH, Webb JK. Occipito-cervical fusion using posterior titanium plates. Eur Spine J 1998;7:308-12. [Google Scholar] [PubMed]
- 23. 23 Finn MA, Bishop FS, Dailey AT. Surgical treatment of occipitocervical instability. Neurosurgery 2008;63:961-8; discussion 968-9. [Google Scholar] [PubMed]
- 24. 24 Lu DC, Roeser AC, Mummaneni VP, Mummaneni PV. Nuances of occipitocervical fixation. Neurosurgery 2010;66 3 Suppl:141-6. [Google Scholar] [PubMed]
- 25. 25 Bono CM. The halo fixator. J Am Acad Orthop Surg 2007;15:728-37. [Google Scholar] [PubMed]
- 26. 26 Garrett M, Consiglieri G, Kakarla UK, Chang SW, Dickman CA. Occipitoatlantal dislocation. Neurosurgery 2010;66 Suppl 3:48-55. [Google Scholar] [PubMed]
- 27. 27 Lee TT, Green BA, Petrin DR. Treatment of stable burst fracture of the atlas (Jefferson fracture) with rigid cervical collar. Spine (Phila Pa 1976) 1998;23:1963-7. [Google Scholar] [PubMed]
- 28. 28 Guo Q, Deng Y, Wang J, Wang L, Lu X, Guo X, Ni B. Comparison of clinical outcomes of posterior C1-C2 temporary fixation without fusion and C1-C2 fusion for fresh odontoid fractures. Neurosurgery 2016;78:77-83. [Google Scholar] [PubMed]
- 29. 29 Zhong D, Lee G, Liao Y, Wang Q. Is it feasible to treat odontoid fractures via primary posterior reduction and fixation without fusion? World Neurosurg 2017;106:693-8. [Google Scholar] [PubMed]
- 30. 30 Han B, Li F, Chen G, Li H, Chen Q. Motion preservation in type II odontoid fractures using temporary pedicle screw fixation: A preliminary study. Eur Spine J 2015;24:686-93. [Google Scholar] [PubMed]
- 31. 31 Yang JJ, Park S, Yoon JY, Mun JW. Temporary bridge occipitocervical fixation for comminuted atlantoaxial fracture. World Neurosurg 2020;139:330-6. [Google Scholar] [PubMed]
- 32. 32 Theologis AA, Deviren V, Tay B. Temporary fusionless posterior occipitocervical fixation for a proximal junctional type II odontoid fracture after previous C2-pelvis fusion: Case report, description of a new surgical technique, and review of the literature. Eur Spine J 2017;26 Suppl 1:243-8. [Google Scholar] [PubMed]
- 33. 33 Rajasekaran S, Soundararajan DC, Shetty AP, Kanna RM. Motion-preserving navigated primary internal fixation of unstable C1 fractures. Asian Spine J 2020;14:466-74. [Google Scholar] [PubMed]
- 34. 34 Hu Y, Yuan ZS, Kepler CK, Dong WX, Sun XY, Zhang J. Comparison of occipitocervical and atlantoaxial fusion in treatment of unstable Jefferson fractures. Indian J Orthop 2017;51:28-35. [Google Scholar] [PubMed]
- 35. 35 Garrido BJ, Sasso RC. Occipitocervical fusion. Orthop Clin North Am 2012;43:1-9, vii. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report
July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report
February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report February 1, 2026 Irreducible Periprosthetic Hip Dislocation Due to Muscular Entrapment with Concomitant Sciatic Nerve Involvement
February 1, 2026 Irreducible Periprosthetic Hip Dislocation Due to Muscular Entrapment with Concomitant Sciatic Nerve Involvement November 1, 2025 Irreducible Dislocation of the Great Toe Interphalangeal Joint Secondary to an Incarcerated Sesamoid: A Retrospective Case Series of Six Patients
November 1, 2025 Irreducible Dislocation of the Great Toe Interphalangeal Joint Secondary to an Incarcerated Sesamoid: A Retrospective Case Series of Six Patients