
Wide excision followed by ipsilateral ulnar transposition serves as a robust biological reconstruction for Campanacci Grade III giant cell tumors of the distal radius, providing stable wrist arthrodesis and preserving forearm rotation without the donor-site morbidity associated with distant autografts.
Dr. Ajith John K, Quarters number 12, Amala Hospital Thrissur, Kerala, India. E-mail: ajith.polutan@gmail.com
Abstract
Introduction: Giant cell tumour (GCT) of the bone is an intermediate, locally aggressive neoplasm with a high incidence in the Indian subcontinent. The distal radius is a frequent site, often presenting with extensive cortical destruction (Campanacci Grade III), necessitating en bloc resection. Reconstructing the resulting defect remains a challenge in orthopaedic oncology. This study evaluates the functional and oncological outcomes of ulnar transposition after radial resection.
Materials and Methods: A cohort of 14 patients with Grade III GCT of the distal radius underwent en bloc resection and reconstruction with ipsilateral ulnar transposition between 2015 and 2023. Functional outcomes were assessed using the Musculoskeletal Tumour Society (MSTS) score, grip strength measurements, and range of motion (supination and pronation). Radiological union times at the ulno-radial and ulno-carpal junctions were recorded.
Results: In our study, we have a total study sample of 14 cases. Both males and females have equal preponderance for GCT of bone. The mean age was calculated to be 39 ± 13.3 years. The mean of the VIII MSTS score was 26.21 ± 1.67. The majority of the patients (78%) have no pain post-operatively. The mean time taken for ulno-radial union was 6.5 months, and for ulnocarpal union was 5.7 months. There is a strong agreement of hand grip strength scores between affected and unaffected hands: Cronbach’s alpha is +0.961. The mean of supination was 83.57 ± 8.419 (range 70–90°). The mean pronation was 75 ± 9.405 (range from 60 to 90°). The mean of actual grip strength of the affected hand is 16.15 kg as compared to 31.78 kg for the opposite side. In 64% of cases, they were not having any post-operative complications associated with surgery. There were only 4 cases (28.5%) of implant failure associated with non-union. One case (7%) of recurrence was noted.
Conclusion: Ulnar transposition is an effective, technically accessible biological reconstruction that avoids the complications of fibular grafting or prosthetics. It provides a stable, painless wrist while preserving significant forearm rotation, making it a viable option for aggressive distal radius tumours.
Keywords: Giant Cell Tumour, Distal Radius, Ulnar Transposition, En-bloc Resection, Wrist Arthrodesis, Biological Reconstruction, Orthopaedic Oncology
The clinical entity known as a giant cell tumour (GCT) of the bone has long fascinated and challenged the orthopaedic community since its initial description by Sir Astley Cooper in 1818. Historically, the understanding of GCT has progressed from a poorly defined lytic lesion to a well-characterised neoplasm under the World Health Organization (WHO) classification, which identifies it as an osteoclastic giant cell-rich tumour of intermediate nature [1]. While fundamentally benign, its biological behaviour is remarkably unpredictable, characterised by local aggressiveness, significant osteolytic potential, and a documented, albeit rare, capacity for pulmonary metastasis, occurring in 1–9% of cases [2]. The epidemiological landscape of GCT reveals a striking geographic disparity. In Western populations, GCT accounts for approximately 5% of all primary bone tumours. In contrast, reports from East Asia and specifically southern India indicate a much higher prevalence, with some series suggesting it constitutes up to 20% of all primary bone neoplasms [3]. The distal end of the radius is the third most common location for GCT, following the distal femur and the proximal tibia [4]. This site is particularly significant due to the complex anatomy of the radiocarpal joint and the high functional demands placed on the wrist in young adults, who are the most frequently affected demographic [5]. The pathogenesis of GCT is rooted in a unique cellular environment. The lesion is composed of mononuclear spindle-like stromal cells, which are considered the neoplastic component, and a massive secondary population of multinucleated osteoclast-like giant cells. The recruitment and activation of these giant cells are driven by the overexpression of the receptor activator of nuclear factor kappa-B ligand (RANKL) by the stromal cells. This RANK-RANKL interaction triggers intense osteoclastic resorption, leading to the rapid destruction of the subchondral bone and cortical expansion [6]. In Campanacci Grade III lesions, this process leads to the complete breach of the bony cortex and extension into the surrounding soft tissues, significantly increasing the risk of local recurrence if the primary surgical management is inadequate. Surgical management remains the cornerstone of treatment for GCT. For less aggressive Grade I and II lesions, extended curettage with the use of local adjuvants such as phenol, liquid nitrogen, or bone cement has shown acceptable results in reducing recurrence [7]. However, for Grade III lesions, where the integrity of the joint surface and the cortical shell is lost, intralesional curettage carries a recurrence risk as high as 65% [8]. En bloc resection offers superior oncological control but leaves a massive segment of missing bone at the distal radius. The subsequent reconstruction must address three goals: Providing a stable support for the hand, preserving as much forearm and hand function as possible, and ensuring long-term biological durability [9]. Various reconstructive options have been described in the literature. Osteoarticular allografts provide an anatomical match but are fraught with risks of infection, non-union, and late articular collapse due to the lack of biological vitality. Vascularised fibular autografts are considered a gold standard for biological reconstruction but involve complex microvascular surgery and significant donor-site morbidity, including common peroneal nerve injury and ankle instability [10]. Custom-made prostheses offer the advantage of early mobilisation but are expensive and carry the risk of mechanical loosening and infection over the long term [11]. Ulnar translocation, originally described by Seradge in 1982, offers a pragmatic and biologically sound alternative [12]. Using the ipsilateral ulna to bridge the defect, the surgeon utilises a local source of autologous bone that maintains its vascularity through its native muscle attachments. This procedure eliminates the need for a secondary surgical site and avoids the complications associated with microvascular anastomosis. Despite its advantages, the procedure results in wrist arthrodesis, which necessitates a careful evaluation of the functional trade-offs. This study aims to provide a comprehensive analysis of the functional outcomes and associated complications of wide excision and ulnar transposition in a cohort of 14 patients treated at a tertiary care centre in South India, contributing to the limited body of evidence regarding this specific reconstructive technique.
Study design and population:
This research was structured as a cohort study conducted at the Department of Orthopaedics at Amala Institute of Medical Sciences (AIMS), a prominent tertiary care hospital in Thrissur, Kerala. The study focused on patients diagnosed with Campanacci Grade III GCT of the distal radius between the years 2015 and 2023. The inclusion criteria were stringent, requiring histological confirmation of GCT and radiological evidence of Grade III disease according to the Campanacci classification. Patients who underwent en bloc resection and ipsilateral ulnar translocation were followed longitudinally to assess functional and radiological outcomes. The study was initiated following approval from the Institutional Ethics Committee (Ref No: 17/EC/22/AIMS-68).
Preoperative staging:
Preoperative evaluation began with a detailed clinical history and physical examination, focusing on pain duration, the presence of a palpable mass, and the degree of wrist joint impairment. Standard radiographic views (AP and lateral) were obtained to assess the lytic lesion, cortical destruction, and potential pathological fractures. Advanced imaging played a crucial role in staging. Computed tomography (CT) scans were utilised to classify the tumour’s intraosseous or extraosseous extension. They were divided into the following classes based on the results of the CT scan. Intraosseous Class I tumours lacked cortical fractures. Extraosseous lesions with cortical fractures limited to a single surface and not extending beyond one-third of the circumference of the bone were classified as Class II tumours. Tumours classified as Class III consisted of extraosseous lesions that had penetrated the cortex on many surfaces or covered more than one-third of the bone’s circumference [13]. Magnetic resonance imaging (MRI) was indispensable for determining the extent of soft tissue involvement and the proximity of the tumour to critical structures such as the median nerve and the radial artery. The level of radial resection was meticulously planned on MRI, ensuring a 1 cm margin of healthy bone proximal to the lesion.
Surgical technique:
The procedures were performed by experienced orthopaedic surgeons under general anaesthesia. A pneumatic tourniquet was used for all cases to ensure a bloodless field, which is essential for identifying the thin, expanded cortex and the margins of the tumour. The approach utilised a dorsal longitudinal incision. The superficial branch of the radial nerve was identified and carefully protected. The forearm musculature was dissected to reveal the tumour, with the second and third extensor compartments being the primary access points. The en bloc resection involved the removal of the distal radius with a margin of 2 cm (based on the T1W MRI image), the tumour, and a cuff of healthy soft tissue. Proximal to the tumour, a transverse osteotomy was performed based on the pre-operative MRI planning. Following the excision of the radius, the focus shifted to the ulna. The distal third of the ulna was exposed, taking care to preserve the muscular attachments of the pronator quadratus and the extensor carpi ulnaris to maintain the blood supply to the bone. An ulnar osteotomy was performed at a level corresponding to the length of the radial defect. The ulnar segment was then translocated laterally into the position previously occupied by the distal radius. Arthrodesis of the wrist was performed by removing the articular surface of the carpal bones (primarily the lunate and radius). The translocated ulna was then stabilised to the proximal radius and the distal carpal bones using a dynamic compression plate (DCP). The plate was carefully contoured to accommodate the shift from the radial to the ulnar axis. The forearm was fixed in a mid-prone position to maximise its functional utility for daily activities. Before closure, the range of forearm rotation was assessed to ensure that the hardware did not mechanically interfere with pronation and supination (Fig. 1).
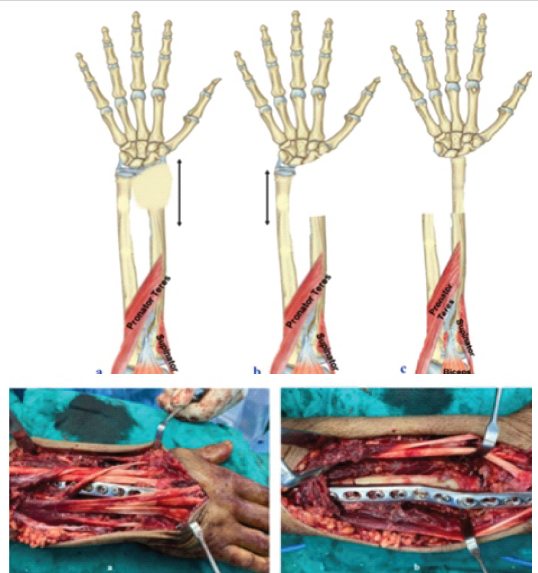
Figure 1: Surgical steps of ulnar transposition.
Post-operative protocol:
The post-operative regimen involved initial immobilisation in a volar splint until wound healing and suture removal. This was followed by a below-elbow cast for a period of approximately 2 months. Early finger movements and elbow exercises were encouraged from the 1st postoperative day. Graded forearm rotation exercises were initiated once early radiological signs of union were observed at the ulno-radial junction. Denosumab, chemotherapy, and radiation are not used pre- or post-operatively. Denosumab is usually reserved for soft tissue recurrence.
Outcome measures:
The primary outcome was the functional assessment using the Musculoskeletal Tumour Society (MSTS) score. This scoring system evaluates six parameters: pain, function, emotional acceptance, hand positioning, manual dexterity, and lifting ability. Each parameter is assigned a score from 0 to 5, providing a maximum possible score of 30.
Secondary outcomes included:
- Grip strength: Measured using a Jamar hand dynamometer at the final follow-up and compared to the contralateral unaffected hand
- Range of motion: Pronation and supination were measured in degrees using a standard goniometer.
- Radiological union: The time to union at both the ulno-carpal and ulno-radial junctions was determined by serial radiographs.
- Complications: Surveillance for implant failure, non-union, local recurrence, and wound-related issues.
Statistical analysis was conducted using the Statistical Package for the Social Sciences version 23. Results for continuous measurements are presented as mean ± standard deviation, while categorical data are presented as frequencies and percentages.
The study cohort consisted of 14 patients, with an equal gender distribution of 7 males (50%) and 7 females (50%). This finding differs slightly from some international series that suggest a female preponderance for GCT, yet it reflects the diverse clinical presentation in the South Indian population. The mean age of the patients was 39.0 ± 13.3 years, with the youngest patient being 20 and the oldest 64. The most common age group affected was 31–40 years, accounting for 35.7% of the cases (Table 1).
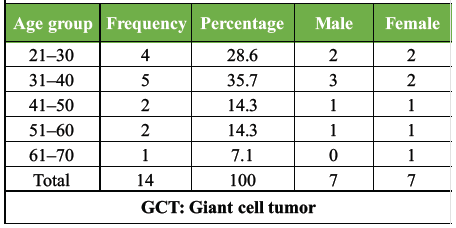
Table 1: Age and gender distribution of the GCT cohort
Clinical presentation and staging:
The majority of patients (78.6%) presented with the classic combination of pain and swelling at the distal end of the radius. One patient (7.1%) presented with a pathological fracture following minor trauma, which is a documented indicator of the aggressive nature of Grade III tumours. Pre-operative physical examination revealed palpable masses and tenderness in 85.7% of cases, with a significant reduction in wrist range of motion due to pain in 100% of the cohort. X-ray findings consistently demonstrated eccentric lytic lesions with cortical destruction, typical of Campanacci Grade III lesions. Regarding co-morbidities, 64.3% of the patients were healthy. The remaining 35.7% presented with controlled type 2 diabetes mellitus, hypertension, or hypothyroidism. These systemic conditions did not preclude surgical intervention but were considered in the postoperative healing phase.
Functional outcome: MSTS score:
The functional evaluation performed at the final follow-up yielded highly encouraging results. The mean MSTS score for the cohort was 26.21 ± 1.67, with individual scores ranging from 23 to 28. A majority of the patients (71.4%) achieved scores of 26 or higher, which signifies an excellent functional outcome according to the Enneking criteria (Table 2).
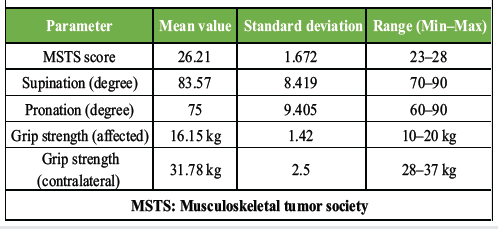
Table 2: Functional assessment summary (range of motion and MSTS)
The individual parameters of the MSTS score provided deeper insight into the patient’s quality of life. Pain assessment revealed that 78.6% of patients had no pain post-operatively, while 21.4% experienced only mild, intermittent pain. Emotional acceptance was high, as the procedure allowed patients to return to their baseline activities and occupations. Manual dexterity and hand positioning scores indicated that despite the loss of wrist mobility, patients effectively compensated using their finger and forearm mobility.
Forearm rotation and range of motion:
One of the primary advantages of ulnar translocation is the preservation of forearm rotation, which is often sacrificed in other types of wrist fusion. In this study, the mean supination achieved was 83.57 ± 8.42, and the mean pronation was 75.00 ± 9.41. Over 57% of the patients regained full supination of 90°, and 64.2% achieved pronation of 80° or more. This preservation of rotation is critical for tasks such as using a keyboard, turning a doorknob, or holding a plate, which significantly impact the patient’s functional independence.
Grip strength comparison:
The handgrip strength of the affected side was compared with that of the contralateral normal hand using a dynamometer. The mean actual grip strength of the affected hand was 16.15 kg, whereas the unaffected side measured 31.78 kg. Thus, the affected hand retained approximately 51% of its normal strength. While this reduction is statistically significant, it was clinically tolerated by all patients. A strong correlation between the strength of the affected and unaffected hands was observed (Cronbach’s alpha: +0.961), suggesting that the surgical reconstruction provided a consistent and predictable functional result.
Radiological union:
The time to achieve biological union is a critical metric for any reconstructive procedure. In our study, the mean time for radiological union at the ulno-carpal junction was 5.7 months (ranging from 4 to 8 months). The ulno-radial junction, which represents the more proximal bone-to-bone interface, took slightly longer to unite, with a mean time of 6.5 months (ranging from 5 to 8 months for those that united) (Table 3).
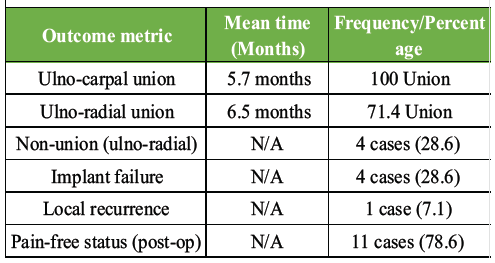
Table 3: Radiological union times and complications
Complications and recurrence:
Despite the high functional scores, the procedure was not without complications. We observed non-union at the ulno-radial junction in 4 cases (28.6%). In all four instances, the persistent lack of union led to fatigue failure of the implant, necessitating revision surgery with bone grafting and replacement of the DCP. One case (7.1%) of local soft tissue recurrence was noted during the follow-up period. This recurrence was managed with the administration of Debusumab, a monoclonal antibody against RANKL, which successfully downstaged the lesion to allow for a second excision with clear margins. There were no reports of surgical site infections, skin necrosis, or major neurovascular complications.
GCT is a benign tumour but locally aggressive in nature. GCTs represent 4–10% of all primary bone tumours and 15–20% of benign bone tumours [14]. However, the report shows a higher incidence of GCT in the Indian and Chinese populations, as high as 20% in the Asian population [15]. In our study, the sample size was 14 patients, which was comparable to Puri et al. In their study, the sample size was 14, and all patients were selected belonging to Campanacci grade III and underwent en bloc excision of the distal radius and ulnar transposition [16]. The problem of reconstructing following distal radius excision for GCT is due to multiple factors, including the high functional demands on the hand, restricted soft tissue around the area, close proximity to nearby nerves and tendons, young age, and the comparatively long life expectancy of these patients. With advantages involving better functional outcomes, preserved vascularity, and the removal of donor site morbidity, en bloc excision with ulna translocation has established itself as a routine treatment option for GCT of the lower end of the radius. Microvascular expertise is not necessary for ipsilateral ulnar transfer following radial resection in comparison to free vascularised fibular grafting. GCT is a benign tumour but locally aggressive in nature. GCTs represent 4–10% of all primary bone tumours and 15–20% of benign bone tumours [14]. However, the report shows a higher incidence of GCT in Indian and Chinese populations, as high as 20% in the Asian population [15]. In our study, the sample size was 14 patients, which was comparable to Puri et al. in their study; also, the sample size was 14, and all patients selected belonged to Campanacci grade III and underwent en bloc excision of the distal radius and ulnar transposition [16]. The problem of reconstructing following distal radius excision for GCT is due to multiple factors, including the high functional demands on the hand, restricted soft tissue around the area, close proximity to nearby nerves and tendons, young age, and the comparatively long life expectancy of these patients. With advantages involving better functional outcomes, preserved vascularity, and the removal of donor site morbidity, en bloc excision with ulna translocation has established itself as a routine treatment option for GCT of the lower end of the radius. Microvascular expertise is not necessary for ipsilateral ulnar transfer following radial resection in comparison to free vascularised fibular grafting. The chief presenting symptoms include dull aching pain and localised swelling at the distal end of the radius lasting for a few months. All the selected patients were healthy, and none of them had any metastasis. One of the patients presented to us initially with a pathological fracture, Campanacci grade III GCT, in the distal end of the radius. In our study, both males and females have equal preponderance with 50%. On the contrary, Campanacci et al. noted a higher predilection for the female gender [4]. The age group of patients with GCT presented to us was commonly in their 2nd and 3rd decades, and as the age progressed, the incidence of GCT was declining. This was comparable to that of Puri et al., in which the common age group GCT presented was between 20 and 40 years, and as the age advances, the incidence of GCT of bone decreases [16]. The mean age of GCT in our study group was 39 years ± 13.3. The predominant age group was between 20 and 40 years (64% of cases, i.e., 9 patients). The mean time taken for ulno-carpal union was 5.7 months, and the mean time taken for ulnoradial union was 6.5 months. Puri et al. [16], in their study, show that at the ulno-carpal junction, the mean time to radiological union was 4.4 months (3.0–7.0), while at the ulno-radial junction, it was 4.9 months (3.0–8.0). Salunke et al. in their study showed that the mean bone union time at the ulna to carpal junction was 4.5 (4–6) months and at the ulna to radius junction was 6.5 (5–8) months, which was comparable to our study [17]. There is a strong agreement of hand grip strength scores between affected and unaffected hands: Cronbach’s alpha is +0.961. The mean hand grip strength is 51.28% compared to the opposite side (range from 34% to 75%). The mean of the actual grip strength of the affected hand is 16.15 kg as compared to 31.78 kg for the normal side in our study. 69% of cases had a good hand grip on the affected side, showing a good functional outcome. This result was comparable to that of Johan et al. in their study, which shows that the hand grip strength mean was 55% compared to the opposite side [18]. Vyas et al., in their study, a retrospective analysis of GCT lower end of the radius treated with en bloc resection and translocation of ulna, showed that the mean of affected side hand grip strength was 29 kg compared to 41 kg for the unaffected side [19]. In our study, the mean of the MSTS score is 26 and ranges from 23 to 28. This was comparable to Johan et al. Their study also showed a mean MSTS score of 25, and Puri et al. showed a mean MSTS score of 26 [18]. This MSTS score shows that there is a good functional upper extremity. Pain assessment was done with the MSTS score, which shows 11 patients out of 14 (>78.3%) with no pain post-operatively and 3 patients (21.7%) with mild pain. The mean value of supination is 83.57, and the standard deviation is 8.419. The mean of pronation is 75, and the standard deviation is 9.405. The majority of patients have supination of 90° (57.1%), which indicates complete regain of supination. Post-operatively, 64.2% of patients have regained pronation of more than or equal to 80°, which indicates a good functional outcome. This value was comparable to Johan et al.’s mean of forearm movement, 82.66° of supination and 81.54° of pronation [18]. McLean et al., in their study, used the ulnar translocation and reconstruction technique for Campanacci grade III GCT of the distal radius, showing an average range of motion of the forearm – 80° of pronation and 70° of supination [20]. We had 4 non-unions at the ulno-radial junction, resulting in all 4 implant failures as a major post-operative complication. Those patients were operated on again, and the previous implant was removed. Then, bone grafting was done at the ulno-radial junction, followed by DCP, which was used to fix the ulno-radial junction. Bhan and Biyani, in their study, also show that there are delayed unions at the ulno-radial junction and require further procedures involving bone grafting at the non-union site. One of the cases presented with soft tissue recurrence at the surgical site postoperatively [21]. This patient was managed with denosumab. As the tumour size shrank with the denuzumab, the tumour was excised with the surrounding soft tissue. Puri et al., in their study, also found 3 soft tissue recurrences of GCT without any bony involvement [16]. There was no surgical site infection, skin necrosis, or wound dehiscence. After the reconstruction, the majority of patients, including those who experienced issues, were able to return to their regular activities and previous jobs. Case showing patient underwent en bloc resection and ulnar translocation with a good functional outcome. This patient has good forearm movements of 90° of pronation and 80° of supination and a hand grip strength of the affected side of 75% of the opposite side. The patient has an MSTS score of 28, suggestive that the patient is having good functional upper extremity in terms of function, hand position, manual dexterity, emotional acceptance, and lifting abilities (Fig. 2).
 Figure 2: Patient underwent en bloc resection and ulnar translocation with a good functional outcome. This patient has good forearm movements of 90° of pronation and 80° of supination and hand grip strength of the affected side of 75% of the opposite side. Patient has a musculoskeletal tumor society score of 28, suggestive patient is having good functional upper extremity in terms of function, hand position, manual dexterity, emotional acceptance, and lifting abilities.
Figure 2: Patient underwent en bloc resection and ulnar translocation with a good functional outcome. This patient has good forearm movements of 90° of pronation and 80° of supination and hand grip strength of the affected side of 75% of the opposite side. Patient has a musculoskeletal tumor society score of 28, suggestive patient is having good functional upper extremity in terms of function, hand position, manual dexterity, emotional acceptance, and lifting abilities.
This is another case that has undergone en bloc resection of the distal end of the radius and ulnar transposition. The post-operative period was uneventful. She was followed up, and serial X-rays showed union of the ulno-radial and ulno-carpal junctions at the 4th month and 6th month, respectively. Her MSTS score was 26, suggesting she was able to do daily activities without much limitation. A year later, when she came in for follow-up, an X-ray was taken which showed a broken implant (Fig. 3).

Figure 3: Case that has underwent en bloc resection of the distal end of the radius and ulnar transposition. The post-operative period was uneventful. She was followed up and serial X-rays showed union of ulno-radial and ulno-carpal junction at the 4th month and 6th month, respectively. Her musculoskeletal tumor society score was 26, suggesting she was able to do daily activities without much limitations. A year later, when she came in for follow-up, an X-ray was taken which showed a broken implant.
However, the patient was apparently normal and was able to perform daily activities without any pain or difficulties. The range of movements of the forearm was assessed for this patient, which showed pronation of 90 degrees and supination of 90 degrees. This shows that almost the full range of pronation and supination was preserved in the forearm. Hand grip strength was assessed and showed 61% (20 kg) compared to the opposite side (34 kg). As a result of a broken implant, she can have reduced dorsiflexion and palmar flexion at her wrist. A limitation of our study is that it is a single institutional study, has no comparison group, and the sample size is limited.
This study confirms that wide excision and ulnar translocation are an effective surgical strategy for Campanacci Grade III GCTs of the distal radius. The procedure provides excellent oncological control with a low recurrence rate compared to intralesional surgery. Functionally, it allows for a painless, stable wrist while preserving a functional range of forearm rotation, resulting in high MSTS scores. Although grip strength is reduced, it remains sufficient for daily activities. The primary complication of non-union at the ulno-radial junction underscores the need for technical precision and robust internal fixation. For patients in resource-limited settings or those requiring biological durability, ulnar translocation remains a superior alternative to allografts, prosthetics, or distant autografts.
In cases of aggressive distal radius giant cell tumours (Grade III), en bloc resection is the preferred oncological approach. Ipsilateral ulnar translocation is a reliable, biological reconstructive technique that preserves forearm rotation and achieves high functional outcomes. Surgeons should consider prophylactic bone grafting at the ulno-radial junction to prevent non-union and implant failure.
References
- 1. Mavrogenis AF, Igoumenou VG, Megaloikonomos PD, Panagopoulos GN, Papagelopoulos PJ, Soucacos PN. Giant cell tumor of bone revisited. SICOT-J 2017;3:54. [Google Scholar] [PubMed]
- 2. Basu Mallick A, Chawla SP. Giant cell tumor of bone: An update. Curr Oncol Rep 2021;23:51. [Google Scholar] [PubMed]
- 3. Saikia KC, Bhuyan SK, Borgohain M, Saikia SP, Bora A, Ahmed F. Giant cell tumour of bone: An analysis of 139 Indian patients. J Orthop Sci 2011;16:581-8. [Google Scholar] [PubMed]
- 4. Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am 1987;69:106-14. [Google Scholar] [PubMed]
- 5. Errani C, Ruggieri P, Asenzio MA, Toscano A, Colangeli S, Rimondi E, et al. Giant cell tumor of the extremity: A review of 209 cases. Skeletal Radiol 2010;39:1201-7. [Google Scholar] [PubMed]
- 6. Morgan T, Atkins GJ, Trivett MK, Johnson SA, Kansara M, Slavin JL, et al. Molecular profiling of giant cell tumor of bone and the osteoclastic localization of ligand for receptor activator of nuclear factor κB. Am J Pathol 2005;167:117-28. [Google Scholar] [PubMed]
- 7. Liu YP, Li KH, Sun BH. Which treatment is the best for giant cell tumors of the distal radius? A meta-analysis. Clin Orthop Relat Res 2009;467:2739-45. [Google Scholar] [PubMed]
- 8. Turcotte RE. Giant cell tumor of bone. Orthop Clin North Am 2006;37:35-51. [Google Scholar] [PubMed]
- 9. Saikia KC, Borgohain M, Bhuyan SK, Goswami S, Bora A, Ahmed F. Resection-reconstruction arthroplasty for giant cell tumor of distal radius. Indian J Orthop 2010;44:327-32. [Google Scholar] [PubMed]
- 10. Scoccianti G, Totti G, Scoccianti M, Mundi S, Campanacci D, Capanna R. Distal radius reconstruction with vascularized fibular graft after bone tumor resection. J Hand Surg Eur Vol 2016;41:982-9. [Google Scholar] [PubMed]
- 11. Liu W, Wang B, Zhang S, Li Y, et al. Wrist reconstruction after en bloc resection of bone tumors of the distal radius. Orthopaedic Surgery. 2021;13(2):376–383. doi:10.1111/os.12737 [Google Scholar] [PubMed] [CrossRef]
- 12. Seradge H. Distal ulnar translocation in the treatment of giant-cell tumors of the distal end of the radius. J Bone Joint Surg Am 1982;64:67-73. [Google Scholar] [PubMed]
- 13. Puthoor D, Iype W. Giant cell tumor: Curettage and bone grafting. Indian J Orthop 2007;41:121-3. [Google Scholar] [PubMed]
- 14. Hosseinzadeh S, Tiwari V, De Jesus O. Giant cell tumor (osteoclastoma). In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024 Available from: https://www.ncbi.nlm.nih.gov/books/nbk559229 [Last accessed on 2024 Jun 28]. [Google Scholar] [PubMed]
- 15. Sung HW, Kuo DP, Shu WP, Chai YB, Liu CC, Li SM. Giant-cell tumor of bone: Analysis of two hundred and eight cases in Chinese patients. J Bone Joint Surg Am 1982;64:755-61. [Google Scholar] [PubMed]
- 16. Puri A, Gulia A, Agarwal MG. Ulnar translocation for reconstruction of the distal radius after tumor resection. J Bone Joint Surg Br Vol 2010;92-B:1684-9. [Google Scholar] [PubMed]
- 17. Salunke AA, Shah J, Warikoo V, Vikram SJ, Meena DK. Ulnar translocation for reconstruction of distal radius after excision of giant cell tumor: A study of 12 cases. J Clin Orthop Trauma 2015;6:223-7. [Google Scholar] [PubMed]
- 18. Johan RK, Saini R, Saini N. Ulnar translocation for reconstruction of the distal radius after tumor resection. Strategies Trauma Limb Reconstr 2015;10:21-7. [Google Scholar] [PubMed]
- 19. Vyas A, Patni P, Saini N, Sharma R, Arora V, Gupta SP. Retrospective analysis of giant cell tumor lower end radius treated with en bloc excision and translocation of ulna. Indian J Orthop 2018;52:10-4. [Google Scholar] [PubMed]
- 20. McLean JM, Clayer M, Stevenson AW, Samson AJ. A modified ulnar translocation reconstruction technique for Campanacci grade 3 giant cell tumors of the distal radius using a clover leaf plate. Tech Hand Up Extrem Surg 2014;18:135-42. [Google Scholar] [PubMed]
- 21. Bhan S, Biyani A. Ulnar translocation after excision of giant cell tumour of distal radius. J Hand Surg Br 1990;15:496-500. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Optimizing Functional Recovery in Multi-Site Giant Cell Tumors
September 1, 2025 Optimizing Functional Recovery in Multi-Site Giant Cell Tumors August 1, 2026 Successful Management of Midshaft Ulna Non-union Using Vascularized Fibula Grafting Following Failed Internal Fixation: A Case Report
August 1, 2026 Successful Management of Midshaft Ulna Non-union Using Vascularized Fibula Grafting Following Failed Internal Fixation: A Case Report August 1, 2025 Solitary Langerhans Cell Histiocytosis of the Distal Radius in an 11-Month-Old Infant: A Case Report
August 1, 2025 Solitary Langerhans Cell Histiocytosis of the Distal Radius in an 11-Month-Old Infant: A Case Report December 1, 2024 Osteochondroma of Distal End Radius Presenting as Carpal Tunnel Syndrome: A Case Report
December 1, 2024 Osteochondroma of Distal End Radius Presenting as Carpal Tunnel Syndrome: A Case Report