
Intraoperative 3D fluoroscopy enhances the detection of dorsal screw prominence during volar plating of distal radius fractures compared with standard 2D imaging, enabling timely intraoperative correction and potentially reducing post-operative complications and revision procedures.
Dr. Zakir Ali Shah, Department of Trauma and Orthopedic, Rashid Hospital, Muhammad Bin Rashid Medical University, Dubai, United Arab Emirates. E-mail: drzakiralishah@gmail.com
Abstract
Introduction: Functional outcomes in distal radius fractures rely on effective surgical fixation and anatomical joint restoration. Volar locking plating is essential for stabilizing intra-articular distal radius fractures. Intraoperative standard 2D fluoroscopic images are typically utilized during the surgical fixation to evaluate the reduction and malposition; however, there has been a recent shift toward the intraoperative 3D fluoroscopy for this purpose, because of the limited role of 2D imaging, which might not give a promising surgical outcome.
Objectives: To evaluate the progressive diagnostic accuracy and performance of intraoperative 3D fluoroscopy compared with intraoperative standard 2D fluoroscopy for detecting screw prominence or malposition during volar plating of distal radius fractures, using post-operative computed tomography (CT) as the reference standard, and to quantify intraoperative screw revisions prompted by imaging.
Design: Retrospective single-cohort diagnostic accuracy study.
Materials and Methods: A total of 52 adult patients with distal radius fractures were selected who underwent surgical fixation within a year with a locking compression plate. All patients had intraoperative 2D fluoroscopy, followed by intraoperative 3D fluoroscopy performed on the affected wrist during the surgery, and subsequently underwent post-operative CT scan in the ward. Prominent screws were defined as ≥1 mm dorsal cortical protrusion. Intraoperative revisions prompted by imaging were recorded. The diagnostic performance of 3D fluoroscopy results was calculated in comparison with Post-operative CT scan results.
Results: Sixty fractures (350 screws) were evaluated. Intraoperative standard 2D fluoroscopy identified 6/350 screws (1.71%) requiring intraoperative exchange. Intraoperative 3D fluoroscopy identified additional screw-related findings not evident on 2D imaging in 32/60 constructs (53.4%), including 20 screws with dorsal cortical extension; 18 were exchanged intraoperatively. Post-operative CT scan identified 10 additional screws with >1 mm dorsal prominence (1.20–2.24 mm) missed by both intraoperative 2D/3D fluoroscopy; 8/10 (80%) were located in dorsal compartments, and none were intra-articular. For dorsal/intra-articular screw detection, intraoperative 3D fluoroscopy demonstrated 71.4% sensitivity and a negative predictive value >97.0%.
Conclusion: Intraoperative 3D fluoroscopy successfully identified dorsal screw prominence compared with intraoperative standard 2D imaging and helped in the correct positioning of the screws. However, post-operative CT scan still identified additional prominent screws missed intraoperatively. We highly recommend utilizing intraoperative 3D fluoroscopy imaging to prevent the need for revision surgeries.
Keywords: 3D fluoroscopy, wrist fractures, distal radius fracture, computed tomography scan, screw prominence.
A distal radius fracture is the standard type of wrist fracture in adults. Volar locking plate fixation is widely accepted for unstable and intra-articular distal radius fractures for stable fixation and early mobilization. Despite recent advances in implant design, the size of the plate and screws used in distal radius surgery frequently increases the risk of flexor and extensor tendon damage [1]. Extensor tendon injuries occur in approximately 8.6% of cases. Extensor tendon rupture is believed to be a result of drilling and the use of lengthy screws, which have been observed during tendon transfer procedures [2]. Routinely, 2D fluoroscopy is used during surgery, but conventional posteroanterior and lateral views may not reliably detect dorsal screw prominence or subtle malposition. (Fig. 1).
 Figure 1: Intraoperative setup for standard 2D fluoroscopy during volar plating of a distal radius fracture.
Figure 1: Intraoperative setup for standard 2D fluoroscopy during volar plating of a distal radius fracture.
These results are commonly identified on post-operative computed tomography (CT) scans. Recent developments enable intraoperative 3D fluoroscopy imaging, providing CT scan-like multidirectional imaging to assess distal screw length, dorsal cortical penetration, joint congruency, and screw malposition during surgery (Fig. 2)[3,4].
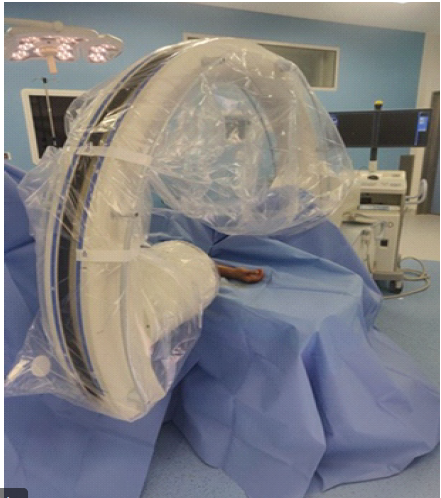 Figure 2: Intraoperative 3D fluoroscopy acquisition setup during distal radius fixation.
Figure 2: Intraoperative 3D fluoroscopy acquisition setup during distal radius fixation.
As a result of a rise in the number of revision surgeries caused by improperly placed or excessively long screws, our hospital has established a protocol to utilize 3D fluoroscopy for every patient. This aims to decrease the rate of revision surgeries.
Study design and setting
This was a retrospective single cohort diagnostic accuracy study conducted at Rashid Hospital, Dubai. All surgeries were performed by fellowship trained orthopedic trauma surgeons following a standardized institutional protocol mandating sequential intraoperative 2D and 3D fluoroscopy for every case. Although post-operative CT is not routinely performed in most centers, our institution follows a standardized protocol for post-operative CT in all distal radius fracture fixations, allowing retrospective analysis of complete imaging data. All patients underwent intraoperative 2D fluoroscopy followed by intraoperative 3D fluoroscopy and post-operative CT scan.
Patient selection criteria
We retrospectively reviewed adult patients treated surgically for distal radius fractures at our institution from January 01, 2024, to December 31, 2024.
We included patients with age ≥18 years; distal radius fracture treated with volar locked plating; intraoperative 2D fluoroscopy and intraoperative 3D fluoroscopy performed; and post-operative CT scan performed. Patients having multiple surgeries for the same fracture and incomplete imaging data were excluded from the study.
Standard surgical technique
Fractures were operated on using a standard volar approach and fixed with a locking compression plate. Screw number and length were selected intraoperatively based on fracture pattern and imaging assessment.
Fluoroscopy imaging protocol
Intraoperative 2D fluoroscopy
2D fluoroscopy was performed using standard posteroanterior and lateral wrist views. Prominent or malpositioned screws identified on 2D were documented and revised intraoperatively when indicated.
Intra operative 3D fluoroscopy
3D fluoroscopy was acquired using an ISO-C-3D system with multiplanar reconstructions (axial, sagittal, and coronal) reviewed intraoperatively. Any long or malpositioned screws identified on 3D imaging were exchanged or repositioned as necessary.
Post-operative CT (reference standard)
A post-operative CT scan was performed in all cases to identify residual discrepancies and screw malposition missed on intraoperative imaging. Post-operative CT was performed as part of our institutional quality assurance protocol to validate intraoperative imaging accuracy and minimize revision risk. Radiation exposure was limited to the wrist region, and the cost was covered under the standard post-operative imaging package. We recorded intraoperative revisions prompted by 2D and/or 3D imaging and compared intraoperative findings with post-operative CT scan.
Definition criteria
Prominent screws were defined as dorsal cortical protrusions≥1 mm on CT scan. Malpositioned screws were defined as intra-articular placement (radiocarpal joint) or involvement of the distal radioulnar joint (DRUJ).
Statistical analysis
Descriptive statistics were used for patient demographics, injury mechanisms, and fracture classification. Screw level proportions were calculated for screws revised based on 2D and 3D imaging results, and screws were identified on the post-operative CT scan. Diagnostic performance measures (sensitivity and negative predictive value) for intraoperative 3D fluoroscopy were reported using post-operative CT scan as the reference standard. Sample size was determined by the total number of eligible cases treated within the study period; no formal power calculation was performed due to the retrospective nature of the study.
Fracture characteristics and patients
A total of sixty (60) distal radius fractures were included from 52 patients, with 8 patients experiencing fractures in both wrists. A total of 350 screws were examined. Among the included patients, there were 28 males and 24 females, with a mean age of 50 years (range 20–80 years). The age distribution and injury characteristics are summarized in Table 1. A total of 18 fractures occurred due to low-energy falls, 14 were caused by high-energy falls, two resulted from pedestrian vehicle collisions, and 18 were caused by motorcycle or motor vehicle collisions. Using the AO Trauma classification system, fractures were type A (0), type B (14), and type C (38) (Table 1).
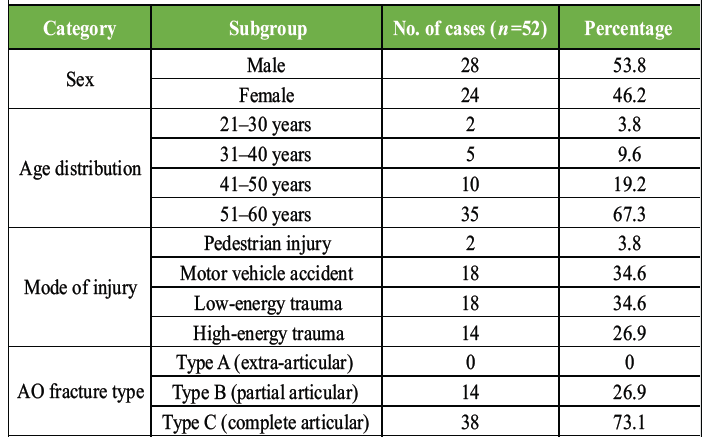
Table 1: Patient demographics, injury mechanisms, and fracture classification (n=52)
Intraoperative 2D fluoroscopy findings
Standard intraoperative 2D fluoroscopy identified prominent screws in 6 of 350 screws (1.71%) used for the 60 fractures, and these screws were replaced with shorter screws during the procedure.
Findings with intraoperative 3D fluoroscopy
Intraoperative 3D fluoroscopy identified additional screw-related findings not evident on routine 2D imaging in 32 of 60 constructs (53.4%). Specifically, 20 screws demonstrated dorsal cortical extension on 3D imaging; 18 screws were exchanged intraoperatively for shorter screws (Fig. 3a and b).
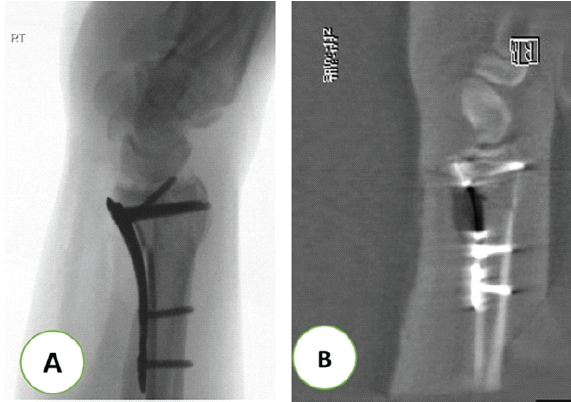
Figure 3: Example of screw assessment using 2D versus 3D imaging. (a) Standard intraoperative 2D fluoroscopic image following volar plate fixation. (b) Intraoperative 3D fluoroscopic reconstruction demonstrating screw assessment relative to the dorsal cortex.
Two screws were not revised because the estimated dorsal extension was <1 mm (below our ≥1 mm definition of screw prominence) and was judged clinically insignificant.
Post-operative CT scan findings
Post-operative CT scan identified 10 additional screws (10/350) with >1 mm dorsal prominence (range 1.20–2.24 mm) that were missed by both intraoperative 2D and 3D fluoroscopy imaging. Of these, 8 (80%) were located in dorsal compartments, with none intra-articular (Table 2).
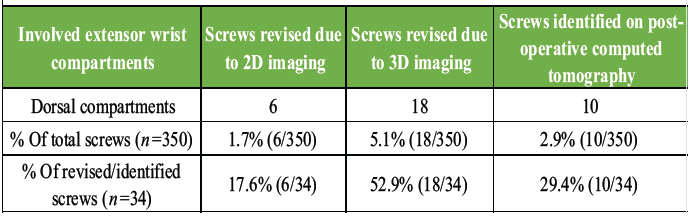
Table 2: Screws revised or identified by imaging modality
Intra-articular/DRUJ penetration and diagnostic performance
No intra-articular (radiocarpal) or DRUJ screw penetrations were identified on intraoperative 2D fluoroscopy, intraoperative 3D fluoroscopy, or post-operative CT scan in our study. For the detection of dorsal/intra-articular screws, intraoperative 3D fluoroscopy showed a sensitivity of 71.4% and a negative predictive value of >97.0% compared with post-operative CT scan.
The structure of the distal radius is intricate and challenging to visualize during surgery. The joint surface of the radius has a biconcave shape and is inclined in various directions [5]. In addition, the frequently employed volar plating method does not provide direct joint visualization; therefore, reduction of intra-articular fractures can only be managed through fluoroscopy. A comprehensive understanding of anatomy and considerable surgical experience are essential for achieving proper anatomical alignment, free from articular steps or gaps, while also ensuring that screw length is adequate, which results in dependable retention of the individual fragments [6]. Conventional intraoperative (posteroanterior and true lateral views) fluoroscopic images do not sufficiently capture the appropriate position and length of the extra-articular subchondral screws [7].
In this study, intraoperative 3D fluoroscopy provided accurate information about screws length and malposition beyond standard 2D fluoroscopy in routine practice. Without 3D imaging, more than 25% of the surgical constructs in our study could have left the operating room with protruding hardware, potentially resulting in irritation and rupture of the extensor tendons. Notably, the 3D imaging was found to be most sensitive in identifying screw length across all extensor compartments. Our findings align with the conclusion provided by Schnetzke et al. [3], who concluded that 3D fluoroscopy images give extra information compared to 2D images in the surgical treatment of distal radius fractures.
Similarly, Wung et al. [8] reported near-perfect agreement between intraoperative 3D fluoroscopy and post-operative CT scan, identifying 62 shorter screws and 22 screw penetrations. The sensitivity and specificity of intraoperative 3D fluoroscopy in detecting dorsal screw protrusion were 81.8% and 98.4%, respectively, while the skyline view’s sensitivity and specificity were 72.2% and 90.9%. Another study by Tonetti et al. [9] showed that the 3D fluoroscopic images are beneficial in assessing the reduction of fractures and implants intraoperatively. Studies conducted on different anatomical regions consistently demonstrate the superiority of 3D imaging and results [10,11,12,13]. A study conducted by Keil et al. [14] resembles our study in detecting malposition of screws and supports, which 3D helps in getting a good surgical outcome and decreases revision rates. In a comparative study by Mehling et al. [15] on 51 patients comparing 2D fluoroscopy and 3D fluoroscopy in distal radius fractures, it was revealed that screws placed during surgery in 31.3% of patients were not detected using standard 2D fluoroscopy but were detected using intraoperative 3D imaging. In addition, Ganesh et al. [16] found that post-operative CT identified prominent screws (≥1 mm) in 17% of cases that were undetected by intraoperative 2D fluoroscopy. They concluded that intraoperative 2D is not enough to identify prominent dorsal screws in distal radius fractures.
In our study, post-operative CT scan identified additional screws with >1 mm dorsal prominence that were missed by both intraoperative 2D/3D imaging. Possible explanations include borderline prominence near the detection threshold, differences in spatial resolution and reconstruction parameters between intraoperative 3D systems and diagnostic CT scan, metal artifact, wrist positioning during acquisition, and interpretive variability. This suggests that 3D fluoroscopy improves intraoperative detection compared with standard 2D views but does not eliminate false negatives.
We used ≥1 mm criteria as the threshold for screw prominence, consistent with imaging-based literature; however, the clinical relevance of minimal dorsal prominence varies depending on dorsal compartment anatomy, tendon proximity, implant design, and patient factors. As standardized clinical follow up and patient reported outcomes were not evaluated in this study, we cannot determine whether the detected prominences were associated with dorsal wrist pain, extensor tendon irritation, tenosynovitis, rupture, or later reoperation.
Limitations
This study has several limitations. First, the retrospective design is subject to documentation variability and unmeasured confounding. Second, there was no control group treated without intraoperative 3D fluoroscopy; therefore, we cannot determine whether 3D fluoroscopy reduces revision rates or improves clinical outcomes compared to 2D alone. Third, imaging technique and interpretation may vary across surgeons. Fourth, screw-level analysis may be affected by clustering of screws within constructs and patients. Finally, operative time, radiation exposure, and cost metrics were not systematically recorded, limiting assessment of workflow and cost-benefit considerations.
Intraoperative 3D fluoroscopy increased the detection of dorsal screw prominence compared with standard 2D fluoroscopy and enabled intraoperative correction in many cases of volar plating for distal radius fractures. However, the post-operative CT scan still identified additional prominent screws. Based on these findings, it is suggested that intraoperative 3D fluoroscopy improves assessment of malposition of screws but does not fully replace post-operative CT scan as the reference standard. Routine use of intraoperative 3D fluoroscopy in distal radius fracture fixation may minimize the risk of post-operative complications, although prospective studies evaluating clinical outcomes, radiation exposure, operative time, and cost-effectiveness are required to further define its clinical importance.
Intraoperative 3D fluoroscopy enhances the detection of dorsal screw prominence during volar plating of distal radius fractures, allowing timely screw correction and reducing the likelihood of post-operative complications. Although post-operative CT may still reveal subtle prominences, incorporating 3D imaging intraoperatively can improve fixation accuracy and help avoid revision procedures.
References
- 1. Kunes JA, Hong DY, Hellwinkel JE, Tedesco LJ, Strauch RJ. Extensor tendon injury after volar locking plating for distal radius fractures: A systematic review. Hand (N Y) 2022;17 1 Suppl:87S-94. [Google Scholar] [PubMed]
- 2. Arora R, Lutz M, Hennerbichler A, Krappinger D, Espen D, Gabl M. Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate. J Orthop Trauma 2007;21:316-22. [Google Scholar] [PubMed]
- 3. Schnetzke M, Fuchs J, Vetter SY, Swartman B, Keil H, Grützner PA, et al. Intraoperative three-dimensional imaging in the treatment of distal radius fractures. Arch Orthop Trauma Surg 2018;138:487-93. [Google Scholar] [PubMed]
- 4. Atesok K, Finkelstein J, Khoury A, Peyser A, Weil Y, Liebergall M, Mosheiff R. The use of intraoperative three-dimensional imaging (ISO-C-3D) in fixation of intraarticular fractures. Injury 2007;38:1163-9. [Google Scholar] [PubMed]
- 5. Ilyas AM. Surgical approaches to the distal radius. Hand (N Y) 2011;6:8-17. [Google Scholar] [PubMed]
- 6. Obert L, Loisel F, Gasse N, Lepage D. Distal radius anatomy applied to the treatment of wrist fractures by plate: A review of recent literature. SICOT J 2015;1:14. [Google Scholar] [PubMed]
- 7. Rausch S, Marintschev I, Graul I, Wilharm A, Klos K, Hofmann GO, et al. Tangential view and intraoperative three-dimensional fluoroscopy for the detection of screw-misplacements in volar plating of distal radius fractures. Arch Trauma Res 2015;4:e24622. [Google Scholar] [PubMed]
- 8. Wung CH, Liu WC, Chiquiar L, Jupiter JB, Regazzoni P, Dell’oca AA. Skyline view versus intraoperative 3D fluoroscopy for dorsal screw protrusion identification following volar plating in the treatment of distal radial fracture. J Orthop Surg Res 2025;20:190. [Google Scholar] [PubMed]
- 9. Tonetti J, Boudissa M, Kerschbaumer G, Seurat O. Role of 3D intraoperative imaging in orthopedic and trauma surgery. Orthop Traumatol Surg Res 2020;106 1 Suppl:S19-25. [Google Scholar] [PubMed]
- 10. Moon SW, Kim JW. Usefulness of intraoperative three-dimensional imaging in fracture surgery: A prospective study. J Orthop Sci 2014;19:125-31. [Google Scholar] [PubMed]
- 11. Carelsen B, Haverlag R, Ubbink DT, Luitse JS, Goslings JC. Does intraoperative fluoroscopic 3D imaging provide extra information for fracture surgery? Arch Orthop Trauma Surg 2008;128:1419-24. [Google Scholar] [PubMed]
- 12. Garber ST, Bisson EF, Schmidt MH. Comparison of three-dimensional fluoroscopy versus postoperative computed tomography for the assessment of accurate screw placement after instrumented spine surgery. Global Spine J 2012;2:95-8. [Google Scholar] [PubMed]
- 13. Beerekamp MS, Sulkers GS, Ubbink DT, Maas M, Schep NW, Goslings JC. Accuracy and consequences of 3D-fluoroscopy in upper and lower extremity fracture treatment: A systematic review. Eur J Radiol 2012;81:4019-28. [Google Scholar] [PubMed]
- 14. Keil H, Beisemann N, Swartman B, Schnetzke M, Vetter SY, Grützner PA, et al. Intraoperative revision rates due to three-dimensional imaging in orthopedic trauma surgery: Results of a case series of 4721 patients. Eur J Trauma Emerg Surg 2023;49:373-81. [Google Scholar] [PubMed]
- 15. Mehling I, Rittstieg P, Mehling AP, Küchle R, Müller LP, Rommens PM. Intraoperative C-arm CT imaging in angular stable plate osteosynthesis of distal radius fractures. J Hand Surg Eur Vol 2013;38:751-7. [Google Scholar] [PubMed]
- 16. Ganesh D, Service B, Zirgibel B, Koval K. The detection of prominent hardware in volar locked plating of distal radius fractures: Intraoperative fluoroscopy versus computed tomography. J Orthop Trauma 2016;30:618-2. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Addressing Bilateral Post-traumatic Distal Radius Growth Arrest with Positive Ulnar Variance with Acute Ulnar Shortening Osteotomy and Distal Radioulnar Joint Fixation in a 13-Year-Old Child: A Case Report
February 1, 2026 Addressing Bilateral Post-traumatic Distal Radius Growth Arrest with Positive Ulnar Variance with Acute Ulnar Shortening Osteotomy and Distal Radioulnar Joint Fixation in a 13-Year-Old Child: A Case Report April 1, 2025 Clinicoradiological Outcome of Variable Angle Volar Locking Plate in the Management of Distal Radius Fractures
April 1, 2025 Clinicoradiological Outcome of Variable Angle Volar Locking Plate in the Management of Distal Radius Fractures June 10, 2024 Comparison of Conventional Incision and 10 mm Approach for Volar Locking Plates in Dorsal Displaced Distal Radius Fractures
June 10, 2024 Comparison of Conventional Incision and 10 mm Approach for Volar Locking Plates in Dorsal Displaced Distal Radius Fractures October 10, 2023 Outcome Analysis of Adult Distal Radius Fractures Managed During COVID-19 Pandemic
October 10, 2023 Outcome Analysis of Adult Distal Radius Fractures Managed During COVID-19 Pandemic