
Adult presentation of congenital macrodactyly is rare; individualised surgical management with ray resection, debulking and carpal tunnel release can provide significant functional and cosmetic improvement.
Dr R. Subashini, Department of Hand Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai, Tamil Nadu, India. E-mail: doctor.subashini@ymail.com
Abstract
Introduction: Macrodactyly is a rare, non-hereditary congenital anomaly characterised by progressive enlargement of digits due to overgrowth of bone, fat, nerve, or soft tissue. It is typically diagnosed and treated in childhood. If left untreated, it may persist into adulthood, resulting in significant functional impairment and cosmetic deformity.
Case Report: We report a 51-year-old female with congenital macrodactyly affecting the left thumb, index, and middle fingers. She experienced progressive enlargement of these digits since birth and reduced function in her left hand. Clinical examination revealed marked hypertrophy, complete loss of function in the left index finger, and partial movement in the thumb and middle finger. Surgical management included amputation of the left index finger, debulking of the thumb and middle finger, and carpal tunnel release.
Conclusion: Postoperatively, the patient demonstrated significant improvement in hand function, reduced digit size, and satisfactory cosmetic results. Adult-onset presentation of macrodactyly is rare, but individualised surgical treatment can lead to substantial improvement.
Keywords: Finger amputation, debulking surgery, digital overgrowth, congenital hand anomaly, macrodactyly.
Macrodactyly is a congenital condition characterised by disproportionate growth of one or more fingers or toes. It is caused by hypertrophy of multiple mesenchymal tissues, including bone, adipose tissue, nerves, and skin [1]. This localised increase in size is usually visible at birth, but the disproportion typically worsens as the child grows [2], leading to functional impairment and cosmetic deformity. Macrodactyly is classified into two main types: static and progressive. In static macrodactyly, the affected digit is enlarged at birth but grows proportionally with the hand. In contrast, progressive macrodactyly is characterised by accelerated growth of the affected digit relative to the others, resulting in increasing deformity over time [3]. While the exact cause is unclear, recent research points to somatic mutations in the PI3K–AKT signalling pathway – specifically the PIK3CA gene [4]. It usually appears as an isolated anomaly, but we must screen patients for other systemic overgrowth conditions. Management of macrodactyly presents significant clinical challenges. Treatment aims to preserve function and enhance the appearance of the hand. Surgical interventions include debulking, epiphysiodesis, osteotomies, ray resection, and amputation [5]. Due to the progressive nature of the condition, patients often require staged procedures and long-term follow-up. We report this case of macrodactyly of the hand due to the limited literature on its clinical presentation and surgical management.
A 51-year-old, right-hand dominant female presented to our department with a complaint of progressive, massive enlargement of the thumb, index, and middle fingers of the left hand. The patient had experienced overgrowth since birth. Her medical history was significant only for primary hypothyroidism, managed with a daily tablet of levothyroxine. There was no history of previous hand injury or infections, and there was no family history of similar congenital anomalies. The patient has now opted for treatment primarily due to a severe decline in her ability to perform activities of daily living (Fig. 1).

Figure 1: Operative X-ray of the hand.
On clinical examination, disproportionate hypertrophy was localised to the thumb, index, and middle fingers of the left hand, corresponding to the median nerve distribution. The index finger was the most severely affected and was fixed in a rigid, non-functional position with severe induration. The thumb and middle finger, although severely enlarged, retained functional arcs of motion at the metacarpophalangeal and interphalangeal joints.
Neurovascular status:
Static two-point discrimination was intact across all affected digits. Capillary refill was adequate, and radial pulse was palpable. No clinical signs of vascular malformation, such as bruits or thrills, were noted.
Radiographic evaluation:
Standard anteroposterior and oblique radiographs of the left hand demonstrated cortical thickening and elongation of the phalanges and metacarpals of the thumb, index, and middle fingers. Massive expansion of the surrounding soft tissue was seen, with no radiographic signs of acute fracture, osteolytic lesions, or premature osteoarthritic degradation of the joint spaces. Considering the significant functional impairment and the patient’s desire to reduce hand bulk, a single-stage multiple surgical procedure was planned. She underwent an index finger ray resection. The index finger was markedly enlarged, stiff, and non-functional. Therefore, a complete ray resection of the index finger was done to decrease the transverse width of the hand and improve functional interaction between the remaining digits.
Soft-tissue debulking:
Extensive debulking of the hypertrophied fibrofatty tissue was done through standard mid-axial incisions along the thumb and middle finger. Careful dissection was undertaken to preserve the digital neurovascular bundles while adequate reduction in soft-tissue volume was achieved.
Prophylactic carpal tunnel release:
Given that macrodactyly is frequently associated with enlargement of the median nerve and its branches, an open carpal tunnel release was performed to decompress the median nerve and reduce the risk of compressive neuropathy.
Macrodactyly of the hand is an uncommon congenital disorder characterised by progressive enlargement of all mesenchymal components of the digit, including bone, subcutaneous tissue, nerves, and skin. It accounts for <1% of congenital anomalies of the upper extremity and frequently presents with significant cosmetic deformity and functional impairment [2]. The condition may manifest as either static or progressive forms, with the latter demonstrating disproportionate growth of the affected digit compared to the remaining digits. The exact pathogenesis of macrodactyly remains incompletely understood. Several theories have been proposed, including abnormal neural influence and fibrofatty proliferation within the digital nerves. Tsuge suggested that hypertrophy of the peripheral nerves may play an important role in stimulating excessive growth of the surrounding tissues [6]. Histological studies frequently demonstrate fibrofatty infiltration of the nerve, often described as lipofibromatous hamartoma, which is commonly associated with enlargement of the median nerve in cases affecting the radial side of the hand [7]. Management of macrodactyly is challenging due to the progressive nature of the deformity and involvement of multiple tissue components. Surgical intervention is typically indicated for significant functional limitation, difficulty with grasp, or cosmetic concerns. Procedures described in the literature include soft-tissue debulking, epiphysiodesis, osteotomy, ray resection, and amputation, depending on the severity of the deformity and patient age [5]. Soft-tissue debulking remains one of the most commonly performed procedures, particularly when the deformity is mainly due to excessive fibrofatty tissue. Debulking procedures aim to reduce the bulk of the digit while preserving neurovascular structures and maintaining hand function. However, recurrence of soft-tissue overgrowth has been reported, and multiple procedures may sometimes be required during the course of treatment [8]. Ray resection is a valuable option when the affected digit is severely enlarged, stiff, and functionally non-contributory. Removal of the involved ray can significantly reduce hand width and improve overall function by facilitating better interaction among the remaining digits. Previous studies have demonstrated satisfactory functional and cosmetic outcomes following ray resection in patients with severe progressive macrodactyly [9]. Another important consideration for this type of presentation during surgical treatment is the involvement of the median nerve. Enlargement of the median nerve and associated fibrofatty infiltration may lead to compressive neuropathy at the level of the carpal tunnel. Therefore, several authors recommend performing carpal tunnel release during surgical reconstruction to prevent or treat median nerve compression [7,9]. Gluck et al. [10] have emphasised that complete nerve excision is necessary due to the nerve-driven overgrowth of the digit, which is thought to be mediated by diffusible growth factors. In the present case, the patient had severe enlargement of the index finger with significant functional limitation. A combined surgical approach consisting of index finger ray resection, soft-tissue debulking of the adjacent digits, and prophylactic carpal tunnel release was performed. This approach allowed reduction in hand bulk, improved functional alignment of the remaining digits, and prevented potential median nerve compression (Figs. 1, 2, 3).
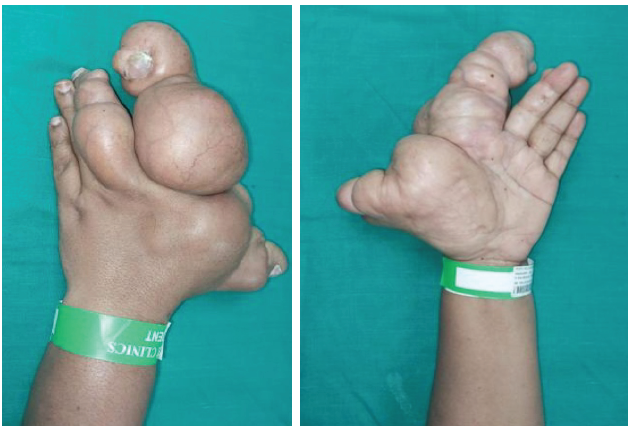
Figure 2: Pre-operative clinical images.
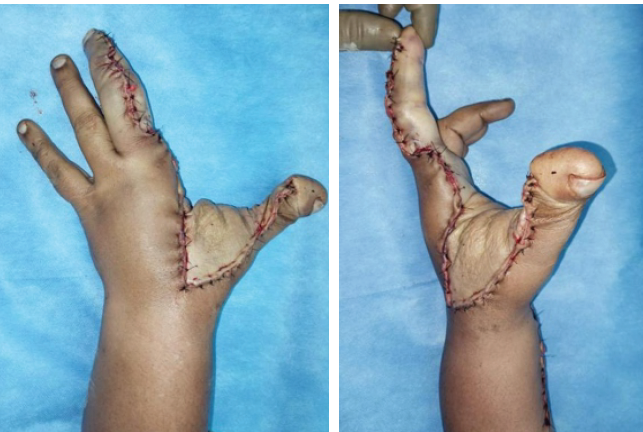
Figure 3: Post-operative clinical images.
Overall, management of macrodactyly should be individualised based on the extent of involvement, functional impairment, and patient expectations. A combination of procedures is often required to achieve satisfactory functional and cosmetic outcomes.
Adult macrodactyly of the hand is a rare congenital anomaly that can cause significant functional and cosmetic impairment. Individualised surgical management, including debulking procedures and selective digit amputation in severe cases, can achieve satisfactory functional outcomes and improve hand appearance.
References
- 1. Barsky AJ. Macrodactyly. J Bone Joint Surg Am 1967;49:1255-66. [Google Scholar] [PubMed]
- 2. Kotwal PP, Farooque M. Macrodactyly. J Bone Joint Surg Br 1998;80:651-3. [Google Scholar] [PubMed]
- 3. Ezaki M, Carter PR. Macrodactyly. J Hand Surg Am. 2004;29:131-8. [Google Scholar] [PubMed]
- 4. Rios JJ, Paria N, Burns DK, Israel BA, Cornelia R, Wise CA, et al. Somatic gain-of-function mutations in PIK3CA in patients with macrodactyly. Hum Mol Genet 2013;22:444-51. [Google Scholar] [PubMed]
- 5. Gluck JS, Ezaki M. Surgical treatment of macrodactyly. J Hand Surg Am 2015;40:1461-8. [Google Scholar] [PubMed]
- 6. Tsuge K. Treatment of macrodactyly. Plast Reconstr Surg 1967;39:590-9. [Google Scholar] [PubMed]
- 7. Spinner RJ, Scheithauer BW, Amrami KK, Wenger DE, Hébert-Blouin MN. Adipose lesions of nerve: The need for a modified classification. J Neurosurg 2012;116:418-31. [Google Scholar] [PubMed]
- 8. Pang CJ, Huo XY, Liu Y, Yang ZY, Liu L, Fan XB, et al. Surgical management of adult hand macrodactyly in a 49-year-old patient: A case report. World J Clin Cases 2024;12:5236-44. [Google Scholar] [PubMed]
- 9. Waters PM, Gillespie BT. Ray resection for progressive macrodactyly of the hand: Surgical technique and illustrative cases. J Hand Surg Am 2016;41:e251-6. [Google Scholar] [PubMed]
- 10. Gluck JS, Ezaki M. Surgical Treatment of Macrodactyly. J Hand Surg Am. 2015;40:1461–1468. doi: 10.1016/j.jhsa.2015.04.017. [Google Scholar] [PubMed] [CrossRef]



Related Articles in Journal of Orthopaedic Case Reports
 April 7, 2014 Fracture of the Anterior Locking Flange of a Total Knee Arthroplasty Polyethylene Liner Presenting with Pain following Knee Replacement
April 7, 2014 Fracture of the Anterior Locking Flange of a Total Knee Arthroplasty Polyethylene Liner Presenting with Pain following Knee Replacement January 28, 2015 A Rare Cause of Postoperative Bleeding from A Lytic Lesion of Calcaneum
January 28, 2015 A Rare Cause of Postoperative Bleeding from A Lytic Lesion of Calcaneum August 1, 2025 Bilateral Chronic Anterior Cruciate Ligament Tear or Congenital Absence of Anterior Cruciate Ligament? – A Case Report
August 1, 2025 Bilateral Chronic Anterior Cruciate Ligament Tear or Congenital Absence of Anterior Cruciate Ligament? – A Case Report May 1, 2026 Surgical Management of Painful Os Vesalianum: A Case Report and Literature Review
May 1, 2026 Surgical Management of Painful Os Vesalianum: A Case Report and Literature Review