
[box type=”bio”] What to Learn from this Article?[/box]
We should be aware of possible insufficiency fracture in the affected limb after total hip arthroplasty.
Case Report | Volume 7 | Issue 2 | JOCR March – April 2017 | Page 11-13| Ryu Kojima, Toshiki Miura, Eisei Fukatani. DOI: 10.13107/jocr.2250-0685.726
Authors: Ryu Kojima[1], Toshiki Miura[1], Eisei Fukatani[1]
[1] Department of Orthopaedic Surgery, JR Tokyo General Hospital, Tokyo, Japan.
Address of Correspondence
Dr. Toshiki Miura,
Department of Orthopaedic Surgery, JR Tokyo General Hospital, 2-1-3, Yoyogi, Shibuya-ku, Tokyo 151-8528, Japan.
E-mail: miuratoshiki@gmail.com
Abstract
Introduction: Although periprosthetic fractures of the femur have been well documented, insufficiency fractures following total hip arthroplasty (THA) have been rarely described. We report a case of an insufficiency fracture in the distal tibia and fibula that occurred after THA.
Case Report: A 54-year-old woman presented with severe pain in the bilateral hip joints and was diagnosed with end-stage osteoarthritis. She underwent THA on the right side. Although the postoperative course was uneventful, she suddenly experienced severe pain and swelling in the right leg without any history of trauma 22 weeks after the surgery. She was first diagnosed with cellulitis by her local doctor and was treated with oral antibiotics. Her symptoms persisted, and she returned to our hospital 1 month later. Her right distal leg and ankle were diffusely swollen and tender. Plain radiographs revealed a sclerotic linear zone in the distal tibia and fibula. She was diagnosed with insufficiency fractures in the distal tibia and fibula following THA. Local disuse osteoporosis and increased mechanical stress after THA as a result of pain relief could be the causes for her fracture. Her right leg and ankle were immobilized with a splint for another 4 weeks. Her symptoms subsided gradually, and fracture union was confirmed on the follow-up X-ray.
Conclusion: Insufficiency fractures should be suspected in patients complaining of unexplainable pain, even in the distant area of the affected limb, for at least 6 months following THA
Keywords: Insufficiency fracture, total hip arthroplasty, distal tibia.
Introduction
Fracture is one of the significant complications of total hip arthroplasty (THA). Although periprosthetic fractures of the femur have been well documented [1, 2, 3, 4], insufficiency fractures following THA have been rarely described [5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. Insufficiency fractures following THA have been reported to occur not only in the periprosthetic areas, including the pubis, acetabulum, and femur [5, 6, 7, 8, 9, 10, 11, 12, 13], but also in the distant areas such as the proximal tibia and the calcaneus, both of which can be easily overlooked unless insufficiency fractures in these areas are suspected [14, 15]. Here, we report a case of an insufficiency fracture in the distal tibia and fibula that occurred after THA.
Case Report
A 54-year-old woman presented with severe pain in the bilateral hip joints. She was limping with a T-cane, and her activities of daily living were remarkably limited. Her height, weight, and body mass index were 152 cm, 55 kg, and 23.8 kg/m2, respectively. The Japanese Orthopaedic Association hip Score was 54 on the right and 45 on the left. Plain radiographs showed bilateral loss of joint space, large osteophytes, and marked deformity of the femoral head and acetabulum (Fig. 1). The width of the cortex of her right femur shaft was thinner than that on her left side. Her right lower limb was 30 mm shorter than her left limb. She was diagnosed with end-stage osteoarthritis of the bilateral hip joints. She first underwent THA on the right side, and it was performed successfully (Fig. 1). The leg length discrepancy was improved by 4 mm after the surgery; however, the right side was still shorter than the left. Full weight bearing was initiated on the second postoperative day. Overall, the postoperative course was uneventful and her walking ability improved.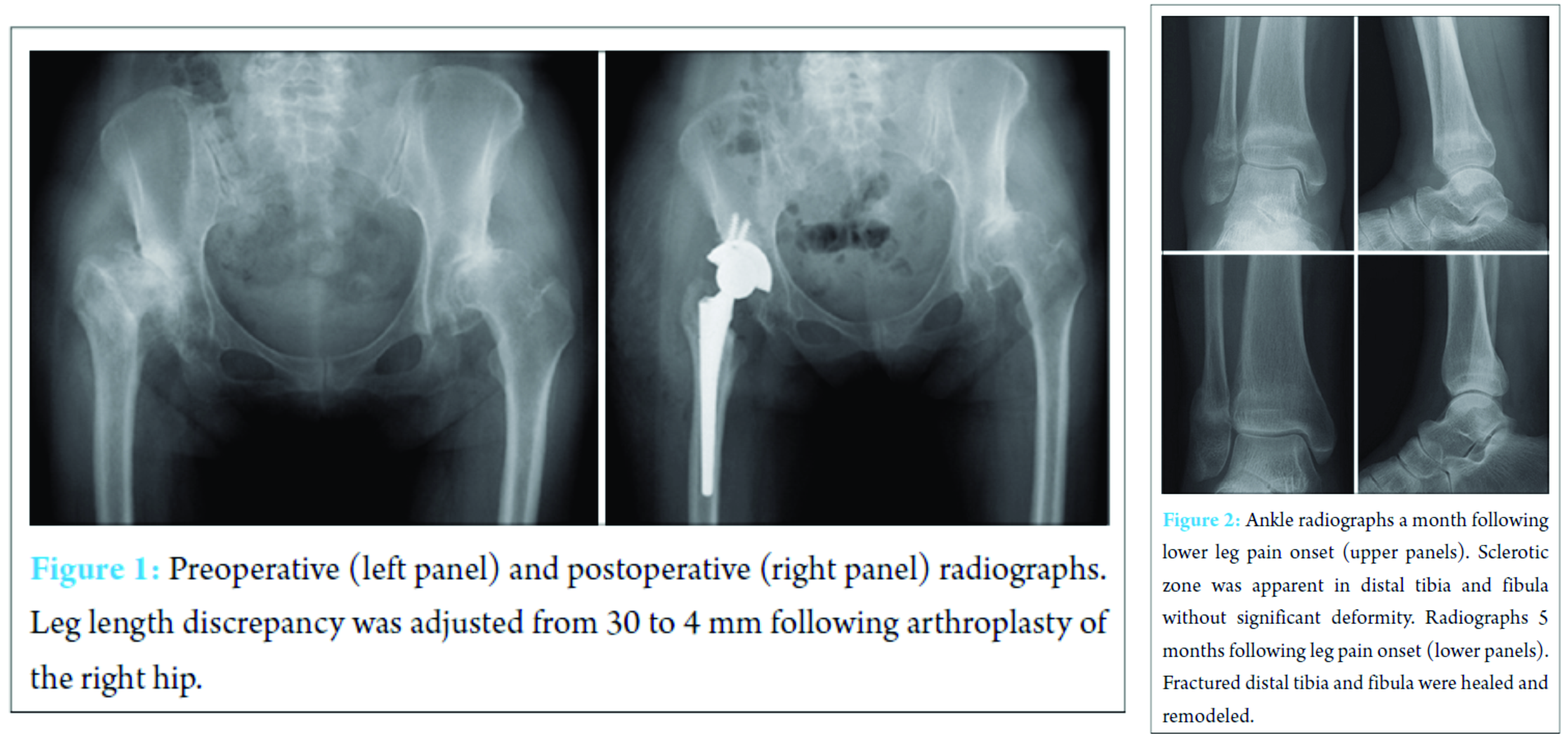
Twenty-two weeks after the surgery, she suddenly experienced severe pain and swelling in the right leg without any history of trauma. She visited her local doctor first and was diagnosed with cellulitis. Although she was treated with oral antibiotics, her symptoms persisted. One month later, she visited our hospital again in a wheelchair. Her right distal leg and ankle were diffusely swollen, red, warm, and tender. Her body temperature was 36.8°C. The following laboratory data were collected, showing normal range in parentheses: White blood cell count, 5300/μl (neutrophil 63.3%; 4000-8000/μl); erythrocyte sedimentation rate, 18 mm/h (1-15 mm/h); C-reactive protein, 1.08 mg/dl (0-0.4 mg/dl); uric acid, 4.7 mg/dl (2.0-6.0 mg/dl); tartrate-resistant acid phosphatase 5b, 478 mU/dl (premenopausal normal range, 120-420 mU/dl); bone alkaline phosphatase, 31.0 μg/l (premenopausal normal range, 2.9‑14.5; postmenopausal normal range, 3.8-22.6 μg/l); calcium, 9.1 mg/dl (8.4‑10.3 mg/dl); and inorganic phosphorus, 3.5 mg/dl (2.3-4.2 mg/dl). Plain radiographs revealed a sclerotic linear zone in the distal tibia and fibula without significant deformity (Fig. 2). There was no arthritic change in the ankle joint. Dual X-ray absorptiometry of the lumbar vertebra was performed to evaluate osteoporosis. Her bone mineral density was 0.731 g/cm2, T-score was −2.5, and Z-score was −0.9. She was diagnosed with an insufficiency fracture in the distal tibia and fibula following THA. Her right leg and ankle were immobilized with a U-slab plaster splint for another 4 weeks. She was advised to bear weight as tolerated. Her symptoms subsided gradually, and fracture union was confirmed on the follow-up X-ray. She was also instructed rehabilitation to prevent osteoporosis.
Discussion
Stress fractures are caused by repetitive stress to the bone. They can be classified into three groups based on the quality of the bone: Fatigue fractures, insufficiency fractures, and pathologic fractures, which appear in a bone with normal strength, a fragile osteoporotic bone, and a fragile bone as a result of tumor invasion, respectively [16, 17]. In our case, the patient had mild, generalized osteoporosis as well as local disuse osteoporosis in the affected limb and suffered a fracture without any history of trauma. Therefore, the case was classified as an insufficiency fracture. Early diagnosis of an insufficiency fracture is difficult because it is a rare event, and early radiographs show no obvious fracture. A bone scintigram is reported to be useful for the early diagnosis of insufficiency fractures whereas computed tomography scanning is of little value in the diagnosis of insufficiency fractures of the long bones [18]. The proper diagnosis of our case was made over 1 month. Repeated radiography is recommended when insufficiency fracture is suspected. Insufficiency fractures in the distal tibia have been reported only in patients with rheumatoid arthritis, osteomalacia, and severe osteoporosis [19]. Although insufficiency fractures in the distal tibia and fibula following THA have not been previously reported in the literature, they might have been overlooked or mistaken for other conditions such as cellulitis, arthritis, and thrombophlebitis. In our case, the patient had bilateral severe osteoarthritis of the hip, and her affected side became the main supporting limb after arthroplasty. In our case, fracture may have been caused because of decreased bone strength in the affected limb due to preoperative limitation of activities as well as postoperative increase of repetitive load owing to pain relief of the hip joint and correction of limb length discrepancy. Miki et al. reported five calcaneal insufficiency fractures following THA and total knee arthroplasty. The mean duration for the appearance of clinical symptoms of these fractures was 10 weeks (range, 6-23 weeks) [14]. In our patient, symptoms appeared 22 weeks after surgery, which was comparable to the findings of a previous report [14]. Insufficiency fractures should be suspected in patients complaining of unexplainable pain, even in the distant area of the affected limb, for at least 6 months following THA.
Conclusion
We reported a rare case of an insufficiency fractures in the distal tibia and fibula that occurred 22 weeks after THA. Insufficiency fractures should be suspected in patients complaining of unexplainable pain, even in the distant area of the affected limb following THA.
Clinical Message
We should be aware of the possible insufficiency fractures for at least 6 months following total joint arthroplasty when the patient complains unexplainable pain even in the distant area of the affected limb.
References
1. Woolson ST, Milbauer JP, Bobyn JD, Yue S, Maloney WJ. Fatigue fracture of a forged cobalt-chromium-molybdenum femoral component inserted with cement. A report of ten cases. J Bone Joint Surg Am 1997;79(12):1842-1848.
2. McElfresh EC, Coventry MB. Femoral and pelvic fractures after total hip arthroplasty. J Bone Joint Surg Am 1974;56(3):483-492.
3. Thien TM, Chatziagorou G, Garellick G, Furnes O, Havelin LI, Mäkelä K, et al. Periprosthetic femoral fracture within two years after total hip replacement: Analysis of 437,629 operations in the Nordic arthroplasty register association database. J Bone Joint Surg Am 2014;96(19):e167.
4. Meek RM, Norwood T, Smith R, Brenkel IJ, Howie CR. The risk of peri-prosthetic fracture after primary and revision total hip and knee replacement. J Bone Joint Surg Br 2011;93(1):96-101.
5. Sharkey PF, Hozack WJ, Callaghan JJ, Kim YS, Berry DJ, Hanssen AD, et al. Acetabular fracture associated with cementless acetabular component insertion: A report of 13 cases. J Arthroplasty 1999;14(4):426-431.
6. Sánchez-Sotelo J, McGrory BJ, Berry DJ. Acute periprosthetic fracture of the acetabulum associated with osteolytic pelvic lesions: A report of 3 cases. J Arthroplasty 2000;15(1):126-130.
7. Hayashi S, Nishiyama T, Fujishiro T, Hashimoto S, Kurosaka M. Bilateral insufficiency fracture of the pelvis following THA: A case report. Case Rep Med 2012;2012:170736.
8. Chitre A, Wynn Jones H, Shah N, Clayson A. Complications of total hip arthroplasty: Periprosthetic fractures of the acetabulum. Curr Rev Musculoskelet Med 2013;6(4):357-363.
9. Springer BD, Berry DJ, Cabanela ME, Hanssen AD, Lewallen DG. Early postoperative transverse pelvic fracture: A new complication related to revision arthroplasty with an uncemented cup. J Bone Joint Surg Am 2005;87(12):2626-2631.
10. Oh I, Hardacre JA. Fatigue fracture of the inferior pubic ramus following total hip replacement for congenital hip dislocation. Clin Orthop Relat Res 1980;147:154-156.
11. Kanaji A, Ando K, Nakagawa M, Fukaya E, Date H, Yamada H. Insufficiency fracture in the medial wall of the acetabulum after total hip arthroplasty. J Arthroplasty 2007;22(5):763-767.
12. Richards CJ, Giannitsios D, Huk OL, Zukor DJ, Steffen T, Antoniou J. Risk of periprosthetic femoral neck fracture after hip resurfacing arthroplasty: Valgus compared with anatomic alignment. A biomechanical and clinical analysis. J Bone Joint Surg Am 2008;90 Suppl 3:96-101.
13. Christiansen CG, Kassim RA, Callaghan JJ, Marsh JL, Schmidt AH. Pubic ramus insufficiency fractures following total hip arthroplasty. A report of six cases. J Bone Joint Surg Am 2003;85-A(9):1819-1822.
14. Miki T, Miki T, Nishiyama A. Calcaneal stress fracture: An adverse event following total hip and total knee arthroplasty: A report of five cases. J Bone Joint Surg Am 2014;96(2):e9.
15. Pierson JL, Ritter MA. Ipsilateral stress fracture of the proximal tibia after primary hybrid total hip arthroplasty. Orthopedics 2005;28(4):409-410.
16. Orhan Z, Parmaksizoglu A, Kayiran E. Calcaneal stress fractures in amateur football players. Eur J Orthop Surg Traumatol 2000;10(2):133-135.
17. Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathologic fractures. JAMA 1964;187:1001-1004.
18. Straaton KV, López-Méndez A, Alarcón GS. Insufficiency fractures of the distal tibia misdiagnosed as cellulitis in three patients with rheumatoid arthritis. Arthritis Rheum 1991;34(7):912-915.
19. Miyakoshi N, Sato K, Murai H, Tamura Y. Insufficiency fractures of the distal tibiae. J Orthop Sci 2000;5(1):71-74.
 |
 |
 |
| Dr. Ryu Kojima | Dr. Toshiki Miura | Dr. Eisei Fukatani |
| How to Cite This Article: Kojima R, Miura T, Fukatani E. Insufficiency Fractures of the Distal Tibia and Fibula Following Total Hip Arthroplasty: A Case Report. Journal of Orthopaedic Case Reports 2017 Mar-Apr;7(2):11-13 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Irreducible Periprosthetic Hip Dislocation Due to Muscular Entrapment with Concomitant Sciatic Nerve Involvement
February 1, 2026 Irreducible Periprosthetic Hip Dislocation Due to Muscular Entrapment with Concomitant Sciatic Nerve Involvement February 1, 2026 Atraumatic Subtrochanteric Stress Fracture in a 45-Year-Old Housewife: Diagnostic Challenge and Management Strategy
February 1, 2026 Atraumatic Subtrochanteric Stress Fracture in a 45-Year-Old Housewife: Diagnostic Challenge and Management Strategy January 1, 2026 A Rare Case of Metabolic Disorder of Bilateral Fracture Neck Femur Treated with Bilateral Total Hip Arthroplasty
January 1, 2026 A Rare Case of Metabolic Disorder of Bilateral Fracture Neck Femur Treated with Bilateral Total Hip Arthroplasty January 1, 2026 Candida albicans Periprosthetic Hip Infection Complicated by Recurrent Dislocations Following Revision Total Hip Arthroplasty: A Case Report
January 1, 2026 Candida albicans Periprosthetic Hip Infection Complicated by Recurrent Dislocations Following Revision Total Hip Arthroplasty: A Case Report