
[box type=”bio”] Learning Point of the Article: [/box]
Solitary peripheral neurofibroma is an infrequent condition that do usually not exhibit clinical manifestations. However, when infrapatellar pain is not alleviated and other causes of such have been discarded, imaging studies must be considered within the differential diagnosis. Afterwards, pathology and molecular biology studies are needed to confirm the histologic type and hence set a curse of treatment.
Case Report | Volume 9 | Issue 1 | JOCR January – February 2019 | Page 28-32| Romeo Tecualt-Gómez, Adriana Atencio-Chan, Gabriela Gutiérrez-Salmeán. DOI: 10.13107/jocr.2250-0685.1294
Authors: Romeo Tecualt-Gómez[1], Adriana Atencio-Chan[2], Gabriela Gutiérrez-Salmeán[3]
[1]Department of Orthopaedic Surgery,Bone and Soft Tissue Orthopedic Surgeon, Angeles Lindavista Hospital, CDMX. 07760. Mexico,
[2]Department of Orthopaedic Surgery, Private General and Orthopedic Pathologist, Bamba River 745. Lindavista. CDMX. Mexico,
[3]Center for Research in Health Sciences, Faculty of Health Sciences, Anahuac University Mexico, North Campus, Mexico.
Address of Correspondence:
Dr. Gabriela Gutiérrez-Salmeán,
Center for Research in Health Sciences, Faculty of Health Sciences, Anahuac University Mexico, North Campus., Av. Universidad Anáhuac 46. Lomas Anáhuac. Huixquilucan 52786. State of Mexico, Mexico.
E-mail: gabrielasalmean@yahoo.com
Abstract
Introduction: Infrapatellar peripheral neural tumors, particularly neurofibromas, are rather rare entities reported in the literature. They are slow-growing lesions that usually do not exhibit clinical manifestations other than interspecific swelling or pain; hence, their diagnosis can be quite challenging. Therefore, scrutiny should include not only traditional clinical assessment and imaging but also more specific molecular biology techniques, such as immunohistochemistry.
Case Report: We present the clinical, imaging, histological, and immunohistochemical features of a unique case of solitary neurofibromain a 33-year-old female presenting chronic anterior knee pain. The tumor was completely removed through a surgical approach.
Conclusions: Although cases of a solitary neurofibroma originating within Hoffa’s fat pad are extremely rare; the entity should be considered in the differential diagnosis when symptomatology is not alleviated with appropriate treatments.
Keywords: Anterior knee pain, Hoffa’s fat pad, immunohistochemistry, solitary neurofibroma.
Introduction
Neurofibromas (Nf) are relatively frequent neoplasms of the peripheral nervous system. They account for about a third of neural tumors and, from these, Nf are entitled foral most 90% of those of the nerve sheath [1]. Most Nf grow as solitary lesions, unless they are associated with neurofibromatosis Type I (i.e., von Reckling hausen disease)and are commonly found in young adults without proclivity to a particular gender [2]. Anatomically, Nf are habitually localized in head and trunk (vs. other body surfaces), although some reports include cases in kidneys, bowel, oral cavity, and spine. Clinically, they present as well-circumscribed -but not encapsulated- bland entities, not associated to other skin alterations (e.g., color and texture), and often smaller than 5–6 cm[3,4]. Nf are slow- and insidious-growing tumors, usually asymptomatic (no significant clinical signs, nonspecific swelling or/and pain may be present); thus, late diagnosis is frequent as it may be confused not only with other soft tissue tumors, either benign or malignant, but also with neuropathies or tendinopathies; hence, histologic assessment is needed. However, because Nf develop from nonmyelinating Schwann cells, the neoplasm -as a whole- can contain other neuromesenchymal cellular types including perineurial cells, fibroblast, and mast cells thus hindering histopathologic diagnosis [5]. Due to the aforementioned, molecular biology studies, particularly immunohistochemistry for which Nf are positive to S100 and negative to act in and CD34- [6,7]provide precise insights into nature, not only of these neoplasms but of the various peripheral nerve sheath tumors (PNST). Despite Nf are benign tumors, surgical approach is the treatment of election since malignant transformation -although not frequent- has been reported [8];recurrences are unusual, but the continuous mass growth may affect surrounding tissues and/orcause functional compromise or/and symptomatology [9]. Hereunder, we present clinical, magnetic resonance imaging (MRI), histopathologic, transoperatory, and immunohistochemical (IHC) features of an unusual -the second [10] to the best of our knowledge, after extensive review of the literature- case of an intra-articular solitary neurofibroma, in a patient without neurofibromatosis, presenting within the infrapatellar fat pad.
Case Report
We report the case of a 33-year-old woman, otherwise healthy, complaining of intermittent and mild anterior knee pain, which was clinically diagnosed as pb. Hoffitis/tendinitis thus managed with nonsteroidal anti-inflammatory drugs and electro-physical therapies, including local ultrasound and electric stimulation. With these, discomfort ceased up until the patient’s second trimester of pregnancy; again, physical therapy, and acetaminophen mitigated the symptoms. However, a year and a half later, the patient presented severe shooting pain and local swelling although no palpable mass could be detected. A MRI scan showed a discretely lobulated ovoid-shaped lesion, with well-defined borders, located below the patella and apparently involving the patellar tendon sheath. As seen in Fig. 1, the neoplasm showed discrete heterogeneous behavior of frank hyperintense predominance in density of protons with fatty saturation, MERGE, slightly hypotensive in T2 and hypotensive in T1; with the contrast medium, its enhancement is homogeneous, measuring approximately 22 mm × 14 mm× 28 mm in its longitudinal, anteroposterior, and transverse axes, respectively. MRI report also included minimum proximal patellar tendinosis, lateral inclination of the patella and mild edema of Hoffa’s fat pat pb. secondary to increased pressure due to the lesion. In accordance to the aforementioned imaging findings, giant cell tumor of the tendon sheath was suggested. Presurgical physical examination of the knee did not show neither positive meniscal signs nor evidence of ligament instability. The patient presented complete flexo-extension of the knee; arcs of movement were complete, although with the presence of pain at the maximum flexion. Muscular tone and strength preserved. Volume increase in the anterior region of the knee, with pain in the interlinear joint were detected after digitopression. No neurovascular involvement of the limb was found. Hence, an incisional biopsy was performed, and surgical could not be, at that time, completed, since transoperatory histopathologic findings -reported as mesenchymal fusocellular neoplasm to be further classified were not sufficient to discard malignancy. H and E staining (Fig. 2) yielded the following description: Lesion consisting of vacuolated and hyperchromatic large nucleus spindle cells, which are arranged in bundles that interlace with each other with densely cellular and collagenized areas; no abnormal mitotic activity is observed. The diagnosis was then proposed as ancient schwannoma.
To confirm the later, IHC markers were used for final staining, as seen in Fig. 3: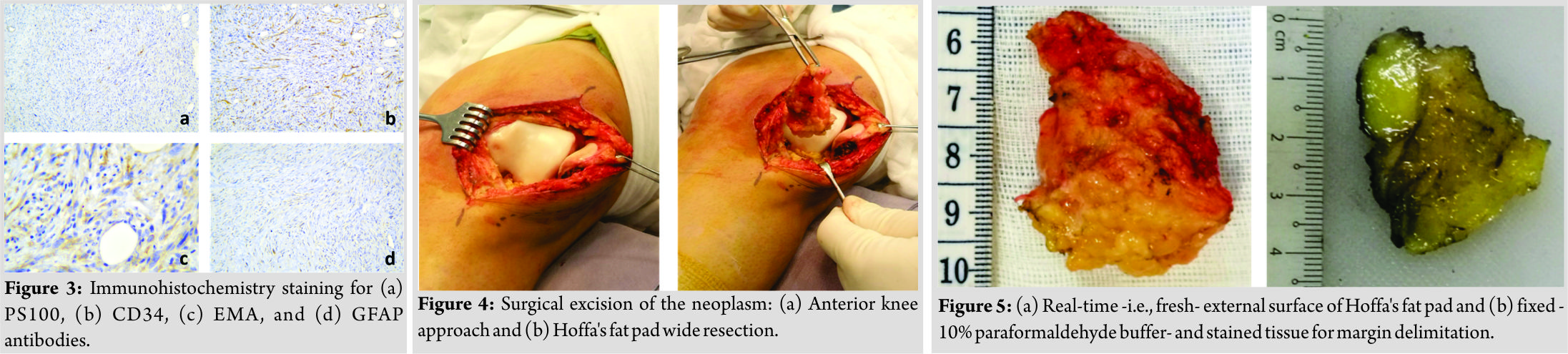
• PS100 ++ (moderate, in patches)
• CD34 ++(besides vascular wall, some cells are positive)
• EMA +(focally weak on cytoplasmatic membrane)
• GFAP +(weak, scarce cells in cytoplasm).
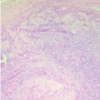
Given the afore, the conclusive histopathologic diagnosis was neurofibroma. Hence, the patient underwent to surgical resection of the mass (measuring 2.3 cm, in its longest axis) -illustrated in Figs. 4 and 5-; in brief, the neuroma was resected by an anterior approach of the knee, performing a dissection in planes, until Hoffa’s fat was localized. A wide resection of the lesion was performed with partial resection of the Hoffa, maintaining the tumoral content within the tissue of the fat pad, to achieve tumor-free surgical margins. There was no clinical or histological evidence that the Nf came from any large or important neurological structure, so it is assumed that it developed from the termination of a terminal sensory branch of the own fat pad. 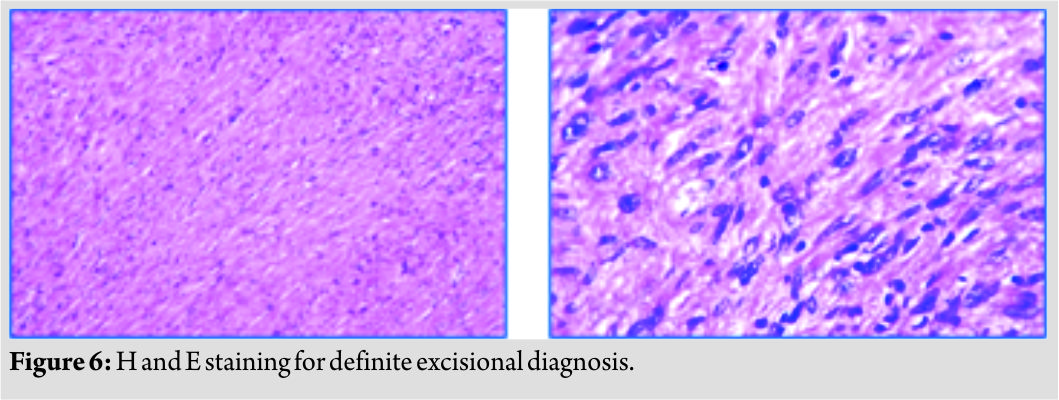 Prior diagnosis was confirmed by histopathological examination(Fig. 6)altogether with clear margins from adjacent tissues: dermis, deep dermis, tendinous and rotula -both superior and inferior- fragments with no sign of lesion. Thus further antineoplastic interventions, for example, radiotherapy, were not needed. At the moment (i.e., 6 months after surgery), the patient has recovered as expected, regained almost full function of the knee and quadriceps (Fig. 7) and has no alterations in the biomechanics of the knee nor pain. Moreover, there is no evidence of recurrence. Regular follow-ups were suggested.
Prior diagnosis was confirmed by histopathological examination(Fig. 6)altogether with clear margins from adjacent tissues: dermis, deep dermis, tendinous and rotula -both superior and inferior- fragments with no sign of lesion. Thus further antineoplastic interventions, for example, radiotherapy, were not needed. At the moment (i.e., 6 months after surgery), the patient has recovered as expected, regained almost full function of the knee and quadriceps (Fig. 7) and has no alterations in the biomechanics of the knee nor pain. Moreover, there is no evidence of recurrence. Regular follow-ups were suggested.
Discussion
Hoffa’s fat pad of the knee is frequently considered among the differential diagnosis of anterior knee pain. However, not so often infrapatellar neoplasms are contemplated within; even less, tumors of nervous etiology. In this sense, Nfs’ incidence has been difficult to establish, but they are considered not so frequent tumors. Moreover, their presentation in lower extremities has not been never but seldom reported [11,12]. As in our case, they are usually found in patients between the third and fifth decade of life and, although most of the literature suggests no gender proclivity [13],some studies have reported higher frequency among women [3].Nfare slow-growing neoplasms that do not usually cause any symptoms. However, swelling may be present and compression of adjacent tissues, including nerves may cause neuropathy and pain [9]. In the case herein presented, we speculate that pregnancy may have contributed to a faster development, thus, explaining the progressive increase in both soft-mass lump identification and pain. Anterior knee pain is a fairly common complaint within the orthopedic practice. However, in certain conditions, clinical exploration may be insufficient and prone to misdiagnosis or confusion with other conditions (e.g., Hoffitis and patellar tendonitis) rather than a tumor. Thus, imaging studies are the next technique of choice for diagnostic purposes. Although radiographs may help to exclude osseous abnormalities, MRI is certainly a more precise approach as it allows the assessment of soft tissue, hence, may, therefore, improve treatment, and contributes to surgical planning [14]. Given the MRI findings, the next step is histopathology classification as most common soft tissue tumors near the knee can range from synovial cysts to high-grade sarcomas. Although Nf’s growth pattern is usually well-circumscribed, its identification can be certainly challenging as they tend to recruit a mixture of cell types yielding an overall form of a spindle. Moreover, as they are slow-growing tumors, some Nf exhibit degenerative features (i.e., ancient change) such as nuclear atypia -enlarged, hyperchromatic nucleus, “smudgy” chromatin-so they may be mistaken for a cancerousneoplasm. However, in contrast to such, Nf do not show mitotic activity. Ergo, once the findings of surgical pathology allow the pinpointing of a PNST, IHC essays are needed for final differential diagnosis. In our case, SD100 positivity decreased the probability of malignancy, CD34 discriminated from schwannoma and, furthermore, EMA positivity allow the distinction from both schwannoma and a malignant PNST [15, 16, 17]. Once the diagnosis is established, surgical excision is the treatment of choice as malignant transformation, although very rare, is an actual possibility. This change has been associated with mutations both in the NF1 gene -whose expression, neurofibromin, acts as a tumor-suppressing protein on the RAS-dependent pathway- [18,19], and in the CDKN2A gene -yet another tumor suppressor, which regulates cell cycle by participating in the control of phase switching (G1 to S) [20,21], among others. The prognosis after effective resection of benign PNST is fairly good as full recovery of the function and alleviation of the symptoms is expected, together with the low rate of recurrence [22].
Conclusion
The development of solitary neurofibroma within Hoffa’s fat pad is a scarcephenomenon which, due to its clinical presentation, can be mistaken with several conditions (e.g., Hoffitis and tendinitis) or a wide variety of other soft tissue tumors -both benign and malignant. Hence, when symptomatologic treatment fails to succeed, differential diagnosis should include not only physical examination but also medical imaging and, when pertinent, both pathologic and IHC techniques. The present case contributes to the current literature on the broad spectrum of clinical presentations of Nf and, moreover, validates surgical resection as the first treatment of choice to minimize the potential of malignant transformation, reduce tumor burden, alleviate symptomatology, restore function, and, in sum, improve quality of life in such extraordinary circumstances.
Clinical Message
Diagnosing the cause of infrapatellar anterior knee pain can be quite challenging and may ultimately be due to certain tumors that present in rather rare fashion. Hence, not only a detailed clinical assessment but also imaging and molecular biology techniques are essential.
References
1. Pradilla-Gordillo MP. Solitary neurofibroma in cervical nerve root C7. Rev Iberoam Cir Mano 2016;44:35-8.
2. Argenyi ZB. Neural and neuroendocrine neoplasm (other than neurofibromatosis). In: Bolognia J, Jorizzo J, Rapini R, editors. Dermatology. 2nd ed. Madrid: Mosby; 2008. p. 1795-811.
3. Reyes-Martínez G, Plascencia-Gómez JA, de Anda-Juárez MC, Gómez-Villa R, Sáenz-Corral C, Carreón AA, et al. Solitary neurofibroma: Its frequency in a general hospital in Mexico City. Dermatol CQM 2012;10:8-12.
4. McDonald JS. Tumors of the oral soft tissues and cysts and tumors of the bones. In: Dean JA, editor. McDonald and Avery’s Dentistry for the Child and Adolescent. 10th ed. USA: Elsevier; 2016. p. 603-26.
5. Zheng H, Chang L, Patel N, Yang J, Lowe L, Burns DK, et al. Induction of abnormal proliferation by nonmyelinating Schwann cells triggers neurofibroma formation. Cancer Cell 2008;13:117-28.
6. Al-Daraji W, Husain E, Zelger BG, Zelger B. A practical and comprehensive immunohistochemical approach to the diagnosis of superficial soft tissue tumors. Int J Clin Exp Pathol 2009;2:119-31.
7. Fisher C. Immunohistochemistry in diagnosis of soft tissue tumours. Histopathology 2011;58:1001-12.
8. Krol EM, El-Fanek H, Borruso J. Solitary neurofibroma with malignant transformation: Case report and review of literature. Conn Med 2015;79:217-9.
9. Barajas-Gamboa JS, Flórez-Salamanca L. Solitary neurofibroma in the abdominal wall of a patient without neurofibromatosis: Case report. Biomedica 2009;29:501-5.
10. Kelly DW, Ovanessoff SA, Rubin JP. Intra-articular neurofibroma: An unusual source of anterior knee pain. Am J Orthop (Belle Mead NJ) 2012;41:492-5.
11. Lee YB, Lee JI, Park HJ, Cho BK. Solitary neurofibromas: Does an uncommon site exist? Ann Dermatol 2012;24:101-2.
12. Tahririan MA, Hekmatnia A, Ahrar H, Heidarpour M, Hekmatnia F. Solitary giant neurofibroma of thigh. Adv Biomed Res 2014;3:158.
13. Atallah I, Gervasoni J, Gay E, Righini CA. Neurofibrome rétropharyngé: À propos d’un cas clinique rare et revue de la littérature. Ann Fr Otorhinolaryngol Pathol Cervicofac 2016;133:44-7.
14. Samim M, Smitaman E, Lawrence D, Moukaddam H. MRI of anterior knee pain. Skeletal Radiol 2014;43:875-93.
15. Rodriguez FJ, Folpe AL, Giannini C, Perry A. Pathology of peripheral nerve sheath tumors: Diagnostic overview and update on selected diagnostic problems. Acta Neuropathol 2012;123:295-319.
16. Schaberg K, Born D, Rouse RV. Neurofibroma; 2018. Available from: http://www.surgpathcriteria.stanford.edu/peripheral-nerve/neurofibroma/. [Last cited on 2018 Jul 12].
17. Miller RT. Immunohistochemistry in the Differential Diagnosis of Schwannoma and Neurofibroma; 2004. Available from: http://www.Propath.Org/Companies/Press-Clippings/26-Newsletters/260-Immunohistochemistry-In-The-Differential-Diagnosis-Of-Schwannoma-And-Neurofibroma-October-2004. [Last cited on 2018 Jul 12].
18. Rosenbaum T, Wimmer K. Neurofibromatosis Type 1 (NF1) and associated tumors. Klin Padiatr2014;226:309-15.
19. Anastasaki C, Gutmann DH. Neuronal NF1/RAS regulation of cyclic AMP requires atypical PKC activation. Hum Mol Genet 2014;23:6712-21.
20. Nielsen GP, Stemmer-Rachamimov AO, Ino Y, Moller MB, Rosenberg AE, Louis DN, et al. Malignant transformation of neurofibromas in neurofibromatosis 1is associated with CDKN2A/p16 inactivation. Am J Pathol 1999;155:1879-84.
21. Sohier P, Luscan A, Lloyd A, Ashelford K, Laurendeau I, Briand-Suleau A, et al. Confirmation of mutation landscape of NF1-associated malignant peripheral nerve sheath tumors. Genes Chromosomes Cancer 2017;56:421-6.
22. Gosk J, Gutkowska O, Urban M, Martynkiewicz J, Bąk M, Ziółkowski P, et al. Benign nerve tumours of the hand (excluding wrist). Arch Orthop Trauma Surg 2015;135:1763-9.
 |
 |
 |
| Dr. Romeo Tecualt-Gómez | Dr. Adriana Atencio-Chan | Dr. Gabriela Gutiérrez-Salmeán |
| How to Cite This Article: Tecualt-Gómez R, Atencio-Chan A, Gutiérrez-Salmeán G. Hoffa’s Fat Pad-associated Solitary Neurofibroma as the Cause of Anterior Knee Pain: A Case Report. Journal of Orthopaedic Case Reports 2019 Jan-Feb; 9(1): 28-32. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Anteromedial Knee Pain Unmasked: Schwannoma of the Infrapatellar Branch of the Saphenous Nerve – A Rare Case Report
January 1, 2026 Anteromedial Knee Pain Unmasked: Schwannoma of the Infrapatellar Branch of the Saphenous Nerve – A Rare Case Report November 1, 2025 Cavernous Hemangioma of Hoffa’s Fat Pad: A Rare Case Presentation
November 1, 2025 Cavernous Hemangioma of Hoffa’s Fat Pad: A Rare Case Presentation November 1, 2025 Giant Cell Tumor with Chondroid Differentiation: A Case Report on This Rare Morphological Variant and a Diagnostic Challenge
November 1, 2025 Giant Cell Tumor with Chondroid Differentiation: A Case Report on This Rare Morphological Variant and a Diagnostic Challenge May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain
May 1, 2025 Patellar Osteoid Osteoma: A Rare Cause for Anterior Knee Pain