
[box type=”bio”] Learning Point of the Article: [/box]
The Importance of Graf Checklist in Graf Method.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 7-10 | Cuneyd Gunay, Hakan Atalar, Ahmet Yigit Kaptan, Erdinc Esen, Ali Turgay Cavusoglu. DOI: 10.13107/jocr.2250-0685.1344
Authors: Cuneyd Gunay[1], Hakan Atalar[2], Ahmet Yigit Kaptan[2], Erdinc Esen[2], Ali Turgay Cavusoglu[2]
[1]Department of Orthopaedics and Traumatology, Faculty of Medicine, Eskisehir Osmangazi University, Eskisehir, Turkey.
[2]Department of Orthopaedics and Traumatology, Faculty of Medicine, Gazi University, Ankara, Turkey.
Address of Correspondence:
Dr. Cuneyd Gunay,
Department of Orthopaedics and Traumatology, Faculty of Medicine, Eskisehir Osmangazi University, Buyukdere mah., Meselik Kampusu, 26480, Eskisehir, Turkey.
E-mail: cungunay@hotmail.com
Abstract
Introduction: According to the Graf method, mature Type 1 hips will not worsen overtime. However, some cases have been reported in literature of hips which were initially Graf Type 1 hips and then worsened later. Our aim is to show the mistakes of the hip sonograms, which had been diagnosed as a mature Graf Type 1 hips.
Case Report: A review of literature revealed four studies initially diagnosed as Graf Type 1 hips and which then worsened overtime. Professor Graf has previously stated that measurements from inappropriate sonograms may result in an incorrect diagnosis. In this paper, the four aforementioned studies and their sonograms reported in literature were evaluated according to the Graf technique. In the light of the findings, it was discussed whether a mature hip could worsen overtime. In the reported cases, some of the deficiencies according to the Graf checklist were determined.
Conclusion: From this examination, it can be concluded that Type 1 mature hips which worsened overtime, except for special circumstances as previously mentioned by Professor Graf, are related to an initial wrong diagnosis. As a result,if a Graf Type 1 hip was determined appropriately according to Graf checklist, it will never worsen later in normal circumstances.
Keywords: Delayed diagnosis, developmental dysplasia of the hip, hip, infant, ultrasonography.
Introduction
Since the use of ultrasound in developmental dysplasia of the hip (DDH) was reported by Professor Graf[1]from Austria, it has rapidly gained acceptance as a means of diagnosing neonatal hip instability as well as monitoring subsequent progress and management. Ultrasonography can detect hip problems that may be missed in clinical and radiographic examinations [2]. Graf’s technique of evaluation is based on a coronal image of the hip obtained from the lateral approach with the femur in anatomic position. His method emphasized angular measurements of acetabular landmarks, in addition to the assessment of hip position [1]. Graf also stated that only sonographic images in the standard plane are acceptable for measurement [3]. If well-defined anatomic sonographic examination, interpretation, and measurement techniques are carefully followed, it is easy to manage the newborn hip problem using this method. If anatomical identification cannot be visualized or the standard plane is missing in a sonographic image, it is of no value and should not be used for diagnosis. In completely dislocated hips (Graf Type 3–4), non-standard sonograms can be used for the evaluation because the displacement of the femoral head avoids the visualization of the femoral head and the center of the acetabulum in the same frontal section [4]. However, for diagnosis of Graf Type 1 mature hips, evaluation should be made from the standard section of the sonographic image [3]. According to Graf, Type 1 mature hips do not worsen overtime except in special circumstances (e.g., neuromuscular disease and septic arthritis). However, in literature, there have been reports of hips, which were Type 1 according to Graf, and which have then worsened overtime. We know that if a hip was diagnosed as Graf Type 1 accurately according to Graf checklist, it will never worsen later except abnormal situations. The aim of this study was to show the mistakes of initial diagnosis of Graf Type 1 hips mentioned in literature that worsened over time.
Case Report
Literature review was applied using the key words“hip dysplasia,” “screening,” “ultrasound,” “late diagnosis,” and “Graf method.”Four papers were found which reported late-diagnosed DDH following a normal ultrasound examination according to the Graf method. The sonograms of those cases were examined in detail to ascertain whether or not they were appropriate according to the Graf checklist [3]. 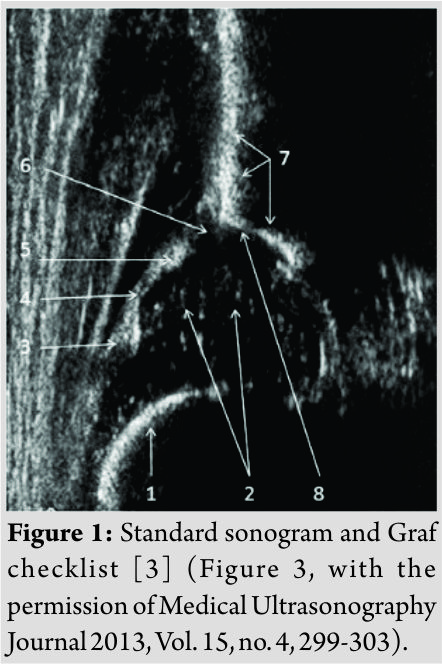 Jones et al. presented “Late presenting dislocation of sonographically stable hips” in 2006 [5]. Rafique et al. presented “Late presentation of developmental DDH following normal ultrasound examination” [6], Jaiswal et al. presented “Late dislocation of the hip following normal neonatal clinical and ultrasound examination” [7], and recently, in 2014, Brinsmead et al. reported “A case of late presentation of developmental DDH with normal screening ultrasound scan” [8]. The demographic information of the patients, and also the congruence of the sonograms to the Graf checklist, is presented in [Table 1].
Jones et al. presented “Late presenting dislocation of sonographically stable hips” in 2006 [5]. Rafique et al. presented “Late presentation of developmental DDH following normal ultrasound examination” [6], Jaiswal et al. presented “Late dislocation of the hip following normal neonatal clinical and ultrasound examination” [7], and recently, in 2014, Brinsmead et al. reported “A case of late presentation of developmental DDH with normal screening ultrasound scan” [8]. The demographic information of the patients, and also the congruence of the sonograms to the Graf checklist, is presented in [Table 1].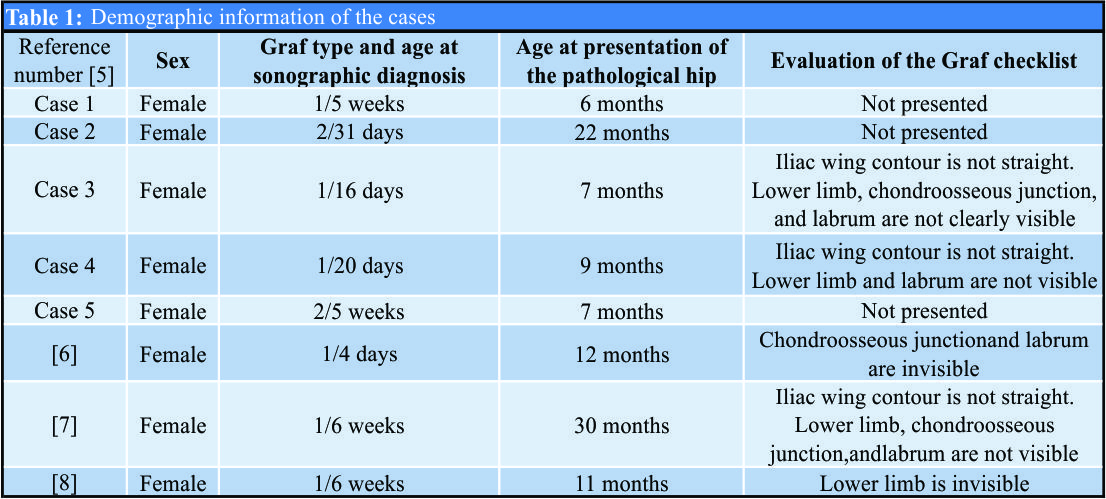
Discussion
Graf technique and hip sonography have spread worldwide over the past 30 years in diagnosing DDH. However, conflicting hip sonography techniques used in various centers are the main cause of discussions regarding sonography and its safety. It remains controversial in respect of whether dislocations are missed on neonatal screening or whether the hip can dislocate at a later date. Typical mistakes can be avoided if the checklists, which were described by Graf [3], are used correctly. Graf checklist, which was showed in Fig. 1, should be checked during performing the hip ultrasonography. Graf checklist contains the following anatomical structures as number 1: Chondroosseous border, number 2: Femoral head, number 3: Synovial fold, number 4: Joint capsule, number 5: Labrum, number 6: Cartilaginous roof, number 7: Bony roof, and number 8: Bony rim (concavity-convexity). If hip sonography is applied using these checklists, wrong diagnosis can be prevented. In the Graf method, the coronal view in the standard plane in the lateral decubitus position can be obtained with the hip in the physiological neutral position (15°–20° flexion). The standard plane is defined by identifying a straight iliac line, the tip of the acetabular labrum, and the transition from the os ilium to the triradiate cartilage [4]. On the sonographic images, the alpha (α) and beta (β) angles were measured, and then, the hip joint was classified according to the Graf method [4]; Type I: Mature hips, Type IIa: Physiologically immature hips; Type IIb and IIc: Dysplastic hips; Type D: Decentric hips; and Type III and IV: Dislocated hips. Obtaining the hip sonography according to the Graf technique by experienced doctors is important[9,10]. In addition, to be able to evaluate the image as a standard section or not, the sonographic picture should be evaluated step by step according to the checklist which was defined by Graf (Fig. 1). You do not need to be experienced and are not dependent on the operator. As shown in [Table 1], the studies presented in literature [5, 6, 7, 8] show deficiencies according to the Graf checklist. The evaluation of sonograms as stated in Table 1 may cause wrong interpretation of the hip joint rather than using the technique developed by Graf [3]. Rosendahl et al. reported that the total number of late cases, and subluxation plus dislocation, was highest in the group not offered ultrasound screening, intermediate in the group receiving selective screening, and lowest in the group subjected to general screening [11]. It has also been stated [11] that of all the infants with late discovered acetabular dysplasia, four of the five patients in the general screening group and two of the three in the selectively screened group were judged normal on ultrasound examination at birth, although the sonographic images were not presented in the paper. It cannot be confirmed, but possibly those sonographic images were not standard images according to the Graf checklist. Jones et al. reported in their study that of the seven dislocated hips, two were Type 1 and five were Type 2 according to Graf’s morphological system [5]. Initial sonographic diagnosis of both hips of the patients 3 and 4 are of Type 1 according to the Graf method. It is known that according to the Graf method, it is mandatory to obtain a sonographic image including a standard plane with a clearly visible lower limb of the bony ilium in the depth of the acetabular fossa, an apparent acetabular labrum, and a straight iliac wing contour in the sonogram [4]. If these conditions are not met in the sonographic image, taking measurements and categorizing a hip may lead to mistakes in diagnosis [12, 13]. The left hip of patient 3 has somewhat anterior section and the right hip has some what posterior section. At the same time, the right hip of patient 4 has an anterior section and the left hip has a posterior section [5]. In addition, Graf stated that a hip, initially considered to be Type 1, could only worsen overtime in cases with a primarily false diagnosis or when neuromuscular disorders, secondary dysplasia, and septic arthritis develop [12]. From reviewing this information, both of these patients can be considered to have had sonographically false diagnoses due to technical mistakes when applying the Graf method. Another point of that paper is that the sonograms of other patients were not presented, but only the angle values were given in the text. When the α and β angles were evaluated, they were found not to be in concordance in each other [5]. Therefore, from these observations, these patients can be considered not to be late hip dislocations. It was stated that in a group of 14,050 infants screened neonatally with ultrasound, no cases of late-detected hip dysplasia were found [14]. Rosendahl et al. [11] also found no cases of late-detected dislocation in their universal ultrasound group. Kohler and Hell reported that delayed diagnosis can be the result of technical errors or misinterpretation [15]. In their study, 6 neonates (43%) had been incorrectly diagnosed. In five cases, theα and β angles had been measured and the sonography was assessed as normal even though the femoral head was poorly covered or not even situated within the acetabulum. In one case (the hip joint categorized as Graf Type 1b), sectional images that did not meet the quality standards of the Graf ultrasound method were measured and diagnosed as normal. The images do not conform to the quality criteria set by Graf in terms of image size and do not show the required landmarks. It is known that clinically stable hips with a normal ultrasound examination showing Graf Type 1 hips do not progress to dislocation and no further patient follow-up is necessary. In some studies, it is widely accepted that infants with normal ultrasound examination can be safely discharged without further radiological follow-up [16, 17]. The limitations of this study were the lack of sonographic images of case 1, 2, and 5 of the study of Jones et al. [5] (Table 1). For these cases, only α and β angles were given. Another limitation was the small number of cases (only four studies/eight cases) included in this study.
Conclusion
If a sonography is made by the Graf method, then the Graf checklist should be strictly adhered to as emphasized by Graf. If an attempt is made to measure the alpha(α) angle on inappropriate sonographic images, an incorrect diagnosis could be made. Therefore, the reported Graf Type 1 hips in literature which were then diagnosed as pathological overtime can be considered not to be due to a worsening of the hip joint but to an initial false diagnosis due to taking inappropriate sonographic images and incorrect interpretation.
Clinical Message
If a hip ultrasonography is done by the Graf method, then the Graf checklist should be examined carefully. Clinically stable hips with a normal ultrasound examination showing Graf Type 1 hips do not progress to dislocation and no further patient follow-up is necessary. Type 1 mature hips which worsened overtime, except for special circumstances as previously mentioned by Professor Graf, are related to an initial wrong diagnosis.
References
1. Graf R.The diagnosis of congenital hip-joint dislocation by the ultrasonic Combound treatment. Arch Orthop Trauma Surg 1980;97:117-33.
2. Wientroub S, Grill F. Ultrasonography in developmental dysplasia of the hip. J Bone Joint Surg Am 2000;82 A:1004-18.
3. Graf R, Mohajer M, Plattner F. Hip sonography update. Quality-management, catastrophes tips and tricks. Med Ultrason 2013;15:299-303.
4. Graf R. Hip Sonography. Diagnosis and Management of İnfant Hip Dysplasia. 2nd ed. Berlin: Springer; 2006.
5. Jones DP, Dunbar JD, Theis JC. Late presenting dislocation of sonographically stable hips. J Pediatr Orthop B 2006;15:257-61.
6. Rafique A, Set P, Berman L. Late presentation of developmental dysplasia of the hip following normal ultrasound examination. Clin Radiol 2007;62:181-4.
7. Jaiswal A, Starks I, Kiely NT. Late dislocation of the hip following normal neonatal clinical and ultrasound examination. J Bone Joint Surg Br 2010;92:1449-51.
8. Brinsmead T, Hong T, Frawley K. A case of late presentation of developmental dysplasia of the hip with normal screening ultrasound scan.J Paediatr Child Health 2014;50:494.
9. Bar-On E, Meyer S, Harari G, Porat S.Ultrasonography of the hip in developmental hip dysplasia. J Bone Joint Surg Br 1998;80:321-4.
10. Dias JJ, Thomas IH, Lamont AC, Mody BS, Thompson JR. The reliability of ultrasonographic assessment of neonatal hips. J Bone Joint Surg Br 1993;75:479-82.
11. Rosendahl K, Markestad T, Lie RT. Ultrasound screening for developmental dysplasia of the hip in the neonate: The effect on treatment rate and prevalence of late cases. Pediatrics 1994;94:47-52.
12. Omeroğlu H. Use of ultrasonography in developmental dysplasia of the hip. J Child Orthop 2014;8:105-13.
13. Graf R, Wilson B. Sonography of the İnfant Hip and its Therapeutic İmplications. London: Chapman and Hall; 1995. p. 1-81.
14. Marks DS, Clegg J, al-Chalabi AN. Routine ultrasound screening for neonatal hip instability. Can it abolish late-presenting congenital dislocation of the hip? J Bone Joint Surg Br 1994;76:534-8.
15. Kohler G, Hell AK. Experiences in diagnosis and treatment of hip dislocation and dysplasia in populations screened by the ultrasound method of graf. Swiss Med Wkly 2003;133:484-7.
16. Arumilli BR, Koneru P, Garg NK, Davies R, Saville S, Sampath J, et al. Is secondary radiological follow-up of infants with a family history of developmental dysplasia of the hip necessary?J Bone Joint Surg Br 2006;88:1224-7.
17. Jellicoe P, Aitken A, Wright K. Ultrasound screening in developmental hip dysplasia: Do all scanned hips need to be followed up? J Pediatr Orthop B 2007;16:192-5.
 |
 |
 |
 |
 |
| Dr. Cuneyd Gunay | Dr. Hakan Atalar | Dr. Ahmet Yigit Kaptan | Dr. Erdinc Esen | Dr. Ali Turgay Cavusoglu |
| How to Cite This Article: Gunay C, Atalar H, Kaptan A Y, Esen E, Cavusoglu T. Can a Hip Diagnosed as Graf Type 1 According to Graf Checklist Deteriorate Over Time? A Case Series and Evaluation of the Graf Method. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 7-10. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty
January 1, 2026 Lumbar Hyperextension Fracture after Direct Anterior Total Hip Arthroplasty December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report
December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report December 1, 2025 Novel Strategy for Incarcerated Broken Broach Retrieval in Total Hip Arthroplasty
December 1, 2025 Novel Strategy for Incarcerated Broken Broach Retrieval in Total Hip Arthroplasty October 1, 2025 Bilateral Simultaneous Anterior Obturator and Pubic Dislocation of the Hip: A Case Report and Literature Review
October 1, 2025 Bilateral Simultaneous Anterior Obturator and Pubic Dislocation of the Hip: A Case Report and Literature Review