
[box type=”bio”] Learning Point of the Article: [/box]
Transfer of the lower trapezius to the infraspinatus might provide a useful salvage procedure for patients with poor functional prognosis of a chronic suprascapular nerve injury.
Case Report | Volume 9 | Issue 2 | JOCR March – April 2019 | Page 56-59 | Shinsuke Takeda, Masahiro Tatebe, Akimasa Morita, Naoki Saka, Katsuyuki Iwatsuki, Hitoshi Hirata. DOI: 10.13107/jocr.2250-0685.1370
Authors: Shinsuke Takeda[1],[2], Masahiro Tatebe[1], Akimasa Morita[2], Naoki Saka[3], Katsuyuki Iwatsuki[1], Hitoshi Hirata[1]
[1]Department of Hand Surgery, Nagoya University Graduate School of Medicine, Japan,
[2]Department of Orthopaedics, Suzuka Kaisei Hospital, Japan,
[3]Departmentof Rehabilitation, Suzuka Kaisei Hospital, Japan.
Address of Correspondence:
Dr. Shinsuke Takeda,
Department of Hand Surgery, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya 466-8550, Japan.
E-mail: s7.takeda.jpn@gmail.com
Abstract
Introduction: Combined injuries to the suprascapular and axillary nerves can result in irreversible dysfunction of the shoulder joint, with reconstruction of shoulder external rotation being an essential component of an effective treatment. Transfer of the lower portion of the trapezius to the infraspinatus has been used, with success, to regain external rotation of the shoulder.
Case Report: We present the case of a 45-year-old man with a chronic traumatic injury of the suprascapular and axillary nerves. In addition to a surgical transfer of the lower trapezius to the infraspinatus, we included a transfer of the latissimus dorsi and teres major, with a tensor fasciaelatae graft to the supraspinatus tendon insertion, to improve the muscular strength of shoulder elevation and abduction, as well as to improve external rotation. At 24-month post-surgery, the patient had recovered 170° of shoulder elevation, 170° of abduction, and 60° of external rotation.
Conclusion: Early recovery after surgery was achieved, with excellent improvement of the range of shoulder motion. We report the transfer of the lower trapezius to the infraspinatus might provide a useful salvage procedure for patients with poor functional prognosis of a chronic suprascapular nerve injury.
Keywords: Lower trapezius transfer, shoulder functional reconstruction, suprascapular and axillary nerves injury.
Introduction
External rotation is an essential component of shoulder function. As such, patients with both suprascapular and axillary nerve injuries face significant impairment in upper limb function. Elhassan et al. have achieved clinically acceptable outcomes for these injuries for over a decade by transferring the lower portion of the trapezius to the infraspinatus muscle, even in cases of chronic rotator cuffs dysfunction, several years after brachial plexus injury, nerve reconstruction, or massive irreparable posterior-superior rotator cuff tears[1,2,3]. In this case report, we describe our surgical management for a trauma patient with combined injuries to the suprascapular and axillary nerves. In an effort to improve the patient’s shoulder elevation and abduction, in addition to the external rotation, we included a transfer of the latissimus dorsi (LD) and teres major (TM) muscles to the basic transfer of the lower portion of the trapezius.
Case Report
A 45-year-old man was injured in a motorcycle accident and transferred to the emergency department in a state of traumatic hemorrhagic shock. Radiographs indicated fractures of the left distal clavicle and scapula, associated with multiple rib fractures and a fracture of the transverse processes of spinal vertebrae. Computed tomography examination revealed a left hemopneumothorax. After resuscitation, the patient underwent osteosynthesis of the left distal clavicle fracture, using tension band wiring. 6-month post-injury, the patient presented to our hospital with severe limitation of shoulder motion, with visible atrophy of the deltoid muscle and inability to perform active shoulder abduction and external rotation. Active range of shoulder motion was as follows: 35° of forward elevation, 20°of abduction, and 0°of external rotation. The strength of all muscle groups of the shoulder, on manual muscle testing, was <M2. No impairments in elbow and wrist function were noted. Electromyography (EMG) assessment identified a complete denervation of the deltoid muscles, with the absence of voluntary potentials, and incomplete paralysis of the supraspinatus and infraspinatus muscles. Based on the EMG and physical examination, a diagnosis of suprascapular and axillary nerve injury. Considering that 6 months had passed since the time of trauma, we selected to perform a radial to axial nerve transfer, using the branch from the medial head of the triceps, while selecting to monitor the status of the suprascapular nerve injury, based on the incomplete paralysis of supraspinatus and infraspinatus. 6-month post-surgery, the contractile strength of the deltoid muscle had improved to M3, but without recovery of shoulder abduction and external rotation, with the significant restriction in shoulder motion persisting at 14-month post-injury, as follows: 80° of elevation, 30°of abduction, and 0°of external rotation (Fig. 1).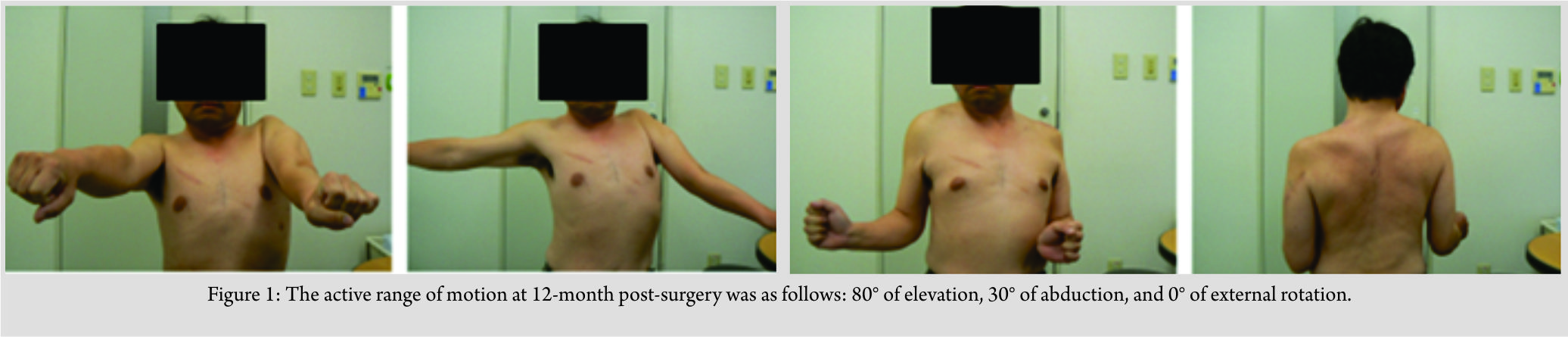 Considering the extent of limitation in shoulder movement, we planned to perform a surgical reconstruction of the functions of the rotator cuff.
Considering the extent of limitation in shoulder movement, we planned to perform a surgical reconstruction of the functions of the rotator cuff.
Surgical procedure
The surgical reconstruction was performed with the patient in a right lateral decubitus position, under general anesthesia. A zigzag incision was created along the axillary line, and the LD and TM were detached from the humerus. LD and TM were transferred to the attachment of the supraspinatus muscle, using an anchor and a 4 cm × 10 cm graft extension of the tensor fascia latae. An incision of approximately 20 cm was created along the spine of the scapula, from the acromion to the inferior angle of scapula. The lower portion of the trapezius was elevated, along with the periosteum from the lateral margin, and directly sutured to the insertion of the infraspinatus muscle using an interlacing technique, without the use of an autogenous tendon (Fig. 2).The wound was closed and an airplane splint applied with the shoulder in 90° of abduction and neutral rotation.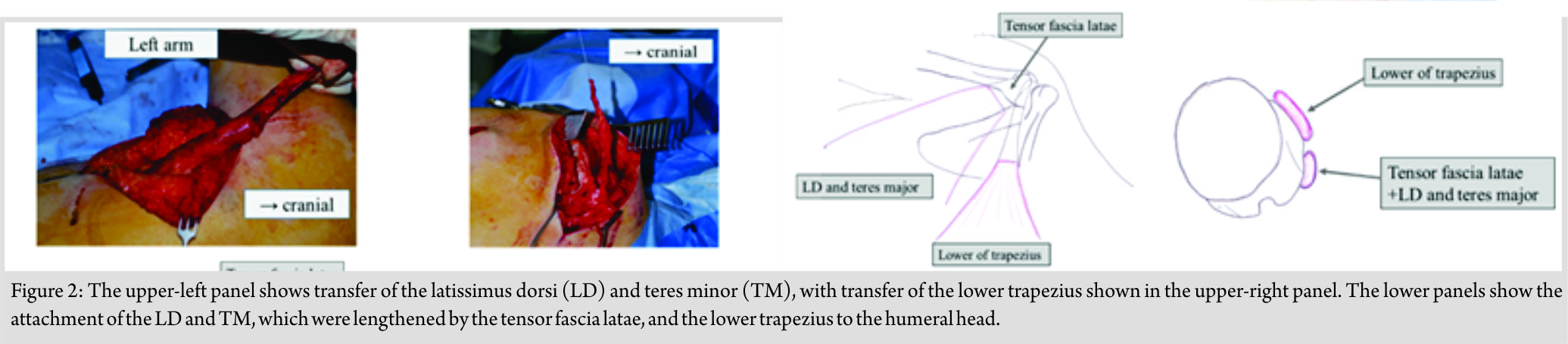
Post-operative course
The patient had begun active and passive elbow range of motion(ROM) at 2-day post-surgery, passive shoulder ROM at 2-week post-surgery, and active shoulder ROM at 4-week post-surgery. After gradual decrease of abduction angles of the airplane splint in 2 weeks, the splint was removed at 6-week post-surgery. 9-week post-surgery, an active range of 110°of the shoulder elevation, 75°of abduction, and 15°of external rotation was achieved. At 12-month post-surgery, the muscle strength of shoulder elevation and external rotation had recovered to M3/M4, and the patient had returned to his activities of swimming and water jet skiing. At 24-month post-surgery, the patient had recovered 170° of shoulder elevation, 170° of abduction, and 60° of external rotation. Moreover, muscle strength of external rotation had recovered to M4 (Fig. 3), with a Hand20 score of 13, compared to 30.5 preoperatively.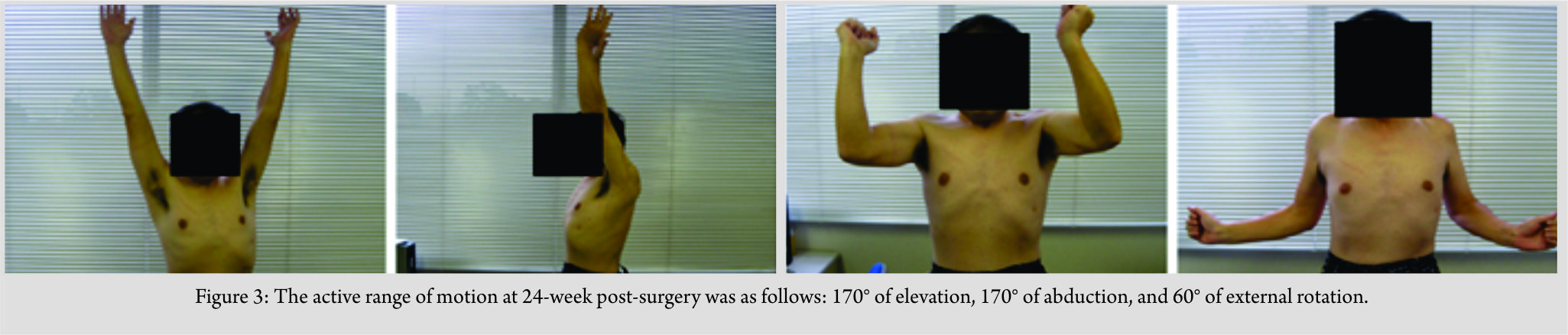
Discussion
Specific differentiation between injury to the upper trunk brachial plexus injury and combined injury to the suprascapular and axillary nerves is often difficult [4]. In patients with injury to the upper brachial plexus, the suprascapular and axially nerves are typically targeted in the reconstruction of shoulder function, especially shoulder external rotation and abduction. Improving external rotation is necessary for the recovery of shoulder function in activities of daily living for patients with a suprascapular nerve palsy [5]. The surgical treatment of chronic suprascapular nerve injury in patients having the potential for recovery of rotator cuff function has not been previously reported. Transfer of the spinal accessory nerve to the suprascapular nerve is a popular treatment in these cases. However, a primary nerve graft or transfer has been recommended to restore shoulder function in patients with a suprascapular nerve injury. Exploration of the suprascapular nerve over its entire length is essential in these cases due to the possibility of several points of the nerve damage. The nerve graft must be performed within the first 3-month post-injury to restore good shoulder function [6, 7, 8]. Baltzer et al. reported that a clinically meaningful recovery of shoulder function following a nerve transfer performed at 1-year post-surgery was achieved in only 33% of cases of the traumatic brachial plexus injury [9]. In our case, the patient presented with an incomplete paralysis, with the possibility of spontaneous neural recovery. As such, we chose to monitor recovery of neural function over a period, which delayed the timing of the salvage procedure; the salvage procedure was ultimately performed in the late phase postoperatively. Elhassan et al. were the first in 2009 to report a surgical transfer of the middle and lower portions of the trapezius to restore shoulder external rotation in a patient who had sustained a brachial plexus injury with complete paralysis of the deltoid, infraspinatus, and teres minor. The transferred tendon was lengthened using an Achilles tendon allograft for fixation at the infraspinatus insertion [2]. In a subsequent report, Elhassan et al. recommended the transfer of only the lower portion of the trapezius, using a tibialis posterior tendon allograft or hamstring autograft, as an alternative option to an Achilles tendon allograft, to prolong the tendon [10]. Although the transfer of the lower portion of the trapezius to the infraspinatus provides functional recovery of shoulder external rotation, it is insufficient to improve shoulder flexion and abduction. Therefore, additional tendon transfers are required[1]. In our case, due to the poor recovery of contractile strength of the deltoid muscle, we included transfer of the LD and TM, using tensor fasciaelatae graft to the insertion of the supraspinatus tendon, which improved the muscle strength of shoulder elevation and abduction. Bonnard et al. stated that the final strength of the deltoid was better when grafting of the axillary nerve was carried out within 5–6 months of injury to the axillary nerve. They also noted a decrease in success rate of the procedure with increasing age, which might be related to a decreased capacity for nerve regeneration with aging. [8] Post-operative recovery was unremarkable, with excellent improvement of the ROM. Although our procedure is useful to improve function, it would be impractical in cases in which the terminal branch of spinal accessory nerve must be used as a nerve transfer. Nevertheless, the transfer of the lower trapezius for the suprascapular nerve palsy in an early stage without the trial of the nerve transfer may be adapted as one choice. Considering the favorable recovery of shoulder function post-surgery, multiple muscle transfers might provide an appropriate treatment option for both chronic rotator cuffs dysfunction and suprascapular nerve injury in patients in whom early functional recovery is anticipated.
Conclusion
We describe a surgical multi-tendon transfer procedure which was successful for the recovery of shoulder elevation, abduction, and external rotation, although performed at 6-month post-injury. Therefore, our method might provide a useful salvage procedure for patients with poor functional prognosis of a chronic suprascapular nerve injury.
Clinical Message
We report the transfer of the lower trapezius to the infraspinatus, which has been used to regain shoulder external rotation, might provide a useful salvage procedure for patients with poor functional prognosis of a chronic suprascapular nerve injury.
References
1. Elhassan B, Bishop AT, Hartzler RU, Shin AY, Spinner R. Tendon transfer options about the shoulder in patients with brachial plexus injury. J Bone JoinSurg 2012;94:1391-8.
2. Elhassan B, Bishop A, Shin A. Trapezius transfer to restore external rotation in a patient with a brachial plexus injury. A case report. J Bone Join Surg Am 2009;91:939-44.
3. Elhassan BT, Wagner ER, Werthel JD. Outcome of lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tear. J Shoulder Elbow Surg 2016;25:1346-53.
4. Asada Y, Kakinoki R, Ikeguchi R. Surgical treatment by nerve transfers for combined injuries of axillary and suprascapular nerves. J Jpn SRM 2012;25:213-8.
5. Langer JS, Sueoka SS, Wang AA. The importance of shoulder external rotation in activities of daily living: Improving outcomes in traumatic brachial plexus palsy. J Hand Surg 2012;37:1430-6.
6. Ochiai N, Nagano A, Mikami Y, Yamamoto S. Full exposure of the axillary and suprascapular nerves. J Bone Join Surg Br 1997;79:532-3.
7. Mikami Y, Nagano A, Ochiai N, Yamamoto S. Results of nerve grafting for injuries of the axillary and suprascapular nerves. J Bone Join Surg Br 1997;79:527-31.
8. Bonnard C, Anastakis DJ, van Melle G, Narakas AO. Isolated and combined lesions of the axillary nerve. A review of 146 cases. J Bone Join Surg Br 1999;81:212-7.
9. Baltzer HL, Wagner ER, Kircher MF, Spinner RJ, Bishop AT, Shin AY. Evaluation of infraspinatus reinnervation and function following spinal accessory nerve to suprascapular nerve transfer in adult traumatic brachial plexus injuries. Microsurg 2017;37:365-70.
10. Elhassan B, Bishop A, Shin A, Spinner R. Shoulder tendon transfer options for adult patients with brachial plexus injury. J Hand Surg 2010;35:1211-9.
 |
| Dr. Shinsuke Takeda |
| How to Cite This Article: Takeda S, Tatebe M, Morita A, Saka N, Iwatsuki K, Hirata H. Transfer of the Lower Trapezius as a Surgical Treatment for Combined Injuries to the Suprascapular and Axillary Nerves: A Case Report. Journal of Orthopaedic Case Reports 2019 Mar-Apr; 9(2): 56-59. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Irreparable Isolated Infraspinatus Musculotendinous Lesion Treated With Lower Trapezius Tendon Transfer: Case Report
June 1, 2025 Irreparable Isolated Infraspinatus Musculotendinous Lesion Treated With Lower Trapezius Tendon Transfer: Case Report November 28, 2019 Giant Cell Tumor of Third Metacarpal: A Rare Case Report and Review of Literature
November 28, 2019 Giant Cell Tumor of Third Metacarpal: A Rare Case Report and Review of Literature January 10, 2024 Central Fracture-Dislocation of the Hip with Ipsilateral Femoral Neck Fracture in an Elderly Patient with Parkinsonism Managed with Dual Mobility Total Hip Arthroplasty: A Case Report and Review of Literature
January 10, 2024 Central Fracture-Dislocation of the Hip with Ipsilateral Femoral Neck Fracture in an Elderly Patient with Parkinsonism Managed with Dual Mobility Total Hip Arthroplasty: A Case Report and Review of Literature July 11, 2014 Anterior Dislocation of Elbow Joint-Case Report of A Rare Injury
July 11, 2014 Anterior Dislocation of Elbow Joint-Case Report of A Rare Injury