
[box type=”bio”] Learning Point of the Article: [/box]
Complex Kyhoscoliosis with severe Kyphosis component can be managed with an all posterior approach without need of anterior release or pre-operative traction.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 8-12 | Munjal S Shah, Kutbuddin Akbary, Priyank M Patel, Abhay M Nene. DOI: 10.13107/jocr.2020.v10.i04.1778
Authors: Munjal S Shah[1], Kutbuddin Akbary[2], Priyank M Patel[1], Abhay M Nene[1]
[1]Department of Orthopaedic Spine Surgery, Lilavati Hospital and Research Centre, Mumbai, Maharashtra, India,
[2]Department of Orthopaedic Spine Surgery, Wockhardt Hospital (South Mumbai), Mumbai, Maharashtra, India.
Address of Correspondence:
Dr. Kutbuddin Akbary,
Consultant Spine Surgeon, Department of Orthopaedic Spine Surgery, Wockhardt Hospital (South Mumbai). Mumbai. Maharashtra. India.
E-mail: kutubakbary@gmail.com
Abstract
Introduction: Neurofibromatosis (NF) 1 is associated with skeletal deformities. Scoliosis is seen in about 10–64% of NF-1 patients. NF-1 may be associated with dystrophic or non-dystrophic type of curve. There are technical difficulties in treating large dystrophic curve with proximal thoracic kyphoscoliosis in NF-1. This case report and subsequent review of literature attempts to provide a line of management for such difficult lesions.
Materials and Methods: We present a case of 22-year-old male with NF-1 who came to us with gradually progressive upper back deformity and signs of early myelopathy for 2–3 months. The patient had a 100° proximal thoracic kyphosis and 100° scoliosis with no neurological deficit and brisk reflexes. A single stage posterior fixation with three column osteotomy at the apex of the curve was performed.
Results: The kyphosis was corrected to 65° from 100, the scoliosis was corrected to 60° from 100. Clinically, the hump in the upper back was visibly reduced. At 1-year follow-up, the patient remained asymptomatic with no loss of correction and implant breakage on X-ray.
Conclusion: Large dystrophic proximal thoracic kyphoscoliosis is a difficult lesion to treat and can be managed with an all posterior approach, achieving good cosmetic and neurological outcomes, as demonstrated by this case.
Keywords: Neurofibromatosis type 1, kyphoscoliosis, dystrophic scoliosis.
Introduction
Neurofibromatosis (NF) is autosomal dominant genetic disorder. NF-1 or von Recklinghausen is peripheral type of NF. Scoliosis is the most common orthopedic manifestation in NF-1 [1, 2]. The prevalence of scoliosis in NF-1 is between 10% and 64% [1, 3]. There are two types of scoliotic curves in NF-1; dystrophic and non-dystrophic. NF-1 patients with dystrophic kyphoscoliosis are accompanied by multiple vertebral abnormalities such as rotatory subluxation, dysplastic pedicles, vertebral scalloping, and spinal tumors [4, 5]. These curves are difficult to correct and are frequently associated with pseudoarthrosis. It has previously been reported that in all cases of severe dystrophic curves with rotatory subluxation, applying halo traction preoperatively would help to improve pulmonary function, increase flexibility of the curves, and minimize neurological risk by gradual traction on a chronically stretched cord [6, 7]. We present a case report of dystrophic proximal thoracic kyphoscoliosis in a known case of NF-1 managed by single stage all posterior fixation with three column osteotomy, without anterior release or pre-operative traction with acceptable cosmetic correction and good neurological outcomes with maintenance of good correction at 1-year follow-up.
Case Report
A 22-year-old male, a previously known case of NF-1, presented with gradually progressive upper back deformity and gait imbalance for the past 2–3 months and was walking without support. His bowel and bladder control were normal. On examination, a prominent hump was noted in the upper back region. On neurological examination, power and sensation were normal. Bilateral knee and ankle reflexes were brisk. Babinski reflex was positive. Radiological investigations such as X-ray whole spine with bending films, computed tomography (CT) scan (Fig. 1), and magnetic resonance imaging (MRI) (Fig. 2) were performed. 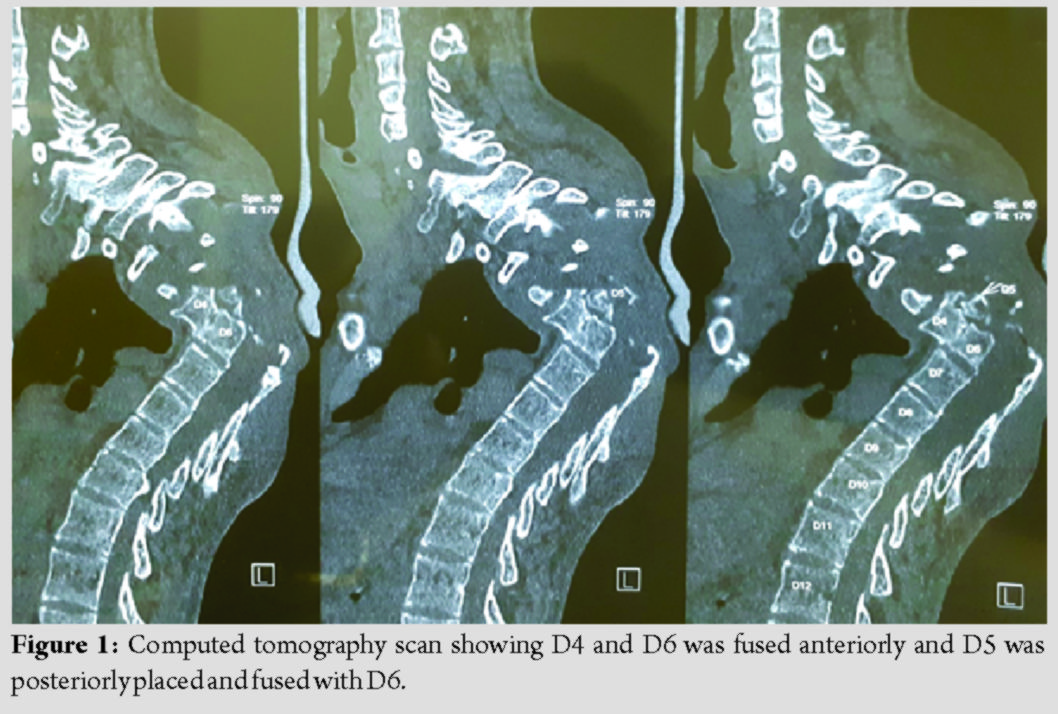 Measurements of the deformity were C2-T1: 40° correcting to 35°, T1-T10: 100° correcting to 70°, T10-L5: 25 degree correcting to 15°, and thoracic kyphosis: 100°. MRI revealed ectasia of thecal sac with a pseudomeningocele on the right side at D3 level. There was a focal hyperintensity at the D5 level. CT scan showed D4-D6 vertebral bodies with the left sided lateral wedging with dysplasia. D2 and D3 posterior elements show dysplasia. D4 and D6 were fused anteriorly and D5 was posteriorly placed and fused with D6.
Measurements of the deformity were C2-T1: 40° correcting to 35°, T1-T10: 100° correcting to 70°, T10-L5: 25 degree correcting to 15°, and thoracic kyphosis: 100°. MRI revealed ectasia of thecal sac with a pseudomeningocele on the right side at D3 level. There was a focal hyperintensity at the D5 level. CT scan showed D4-D6 vertebral bodies with the left sided lateral wedging with dysplasia. D2 and D3 posterior elements show dysplasia. D4 and D6 were fused anteriorly and D5 was posteriorly placed and fused with D6.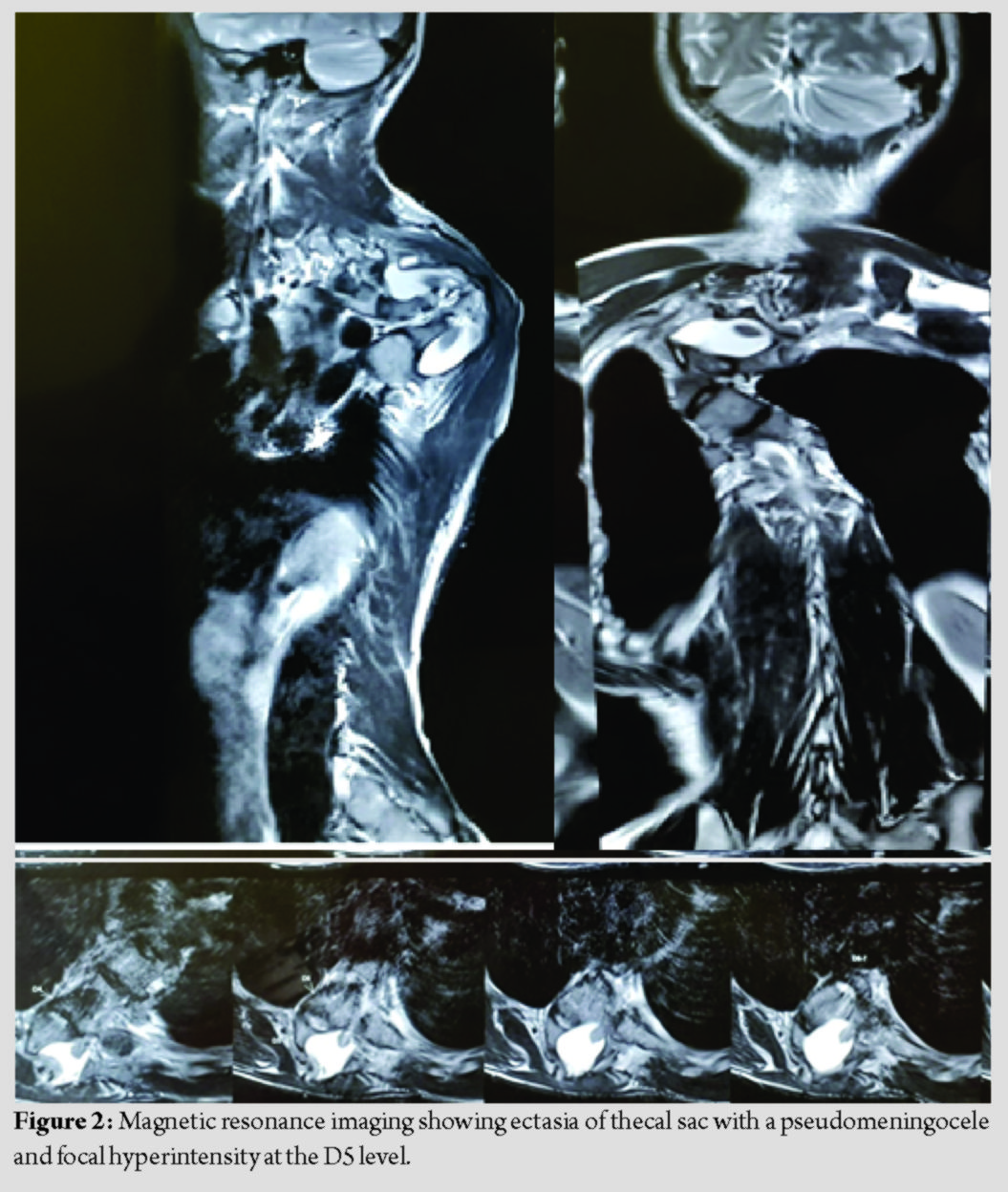
A single Stage 3 column osteotomy with posterior fixation by an all posterior approach was performed. Closing osteotomy was performed at D5 level. The intraoperative neuromonitoring was unchanged from baseline throughout the procedure. C7-T2 and D8-L1 pedicle screw fixation with titanium rod was done. 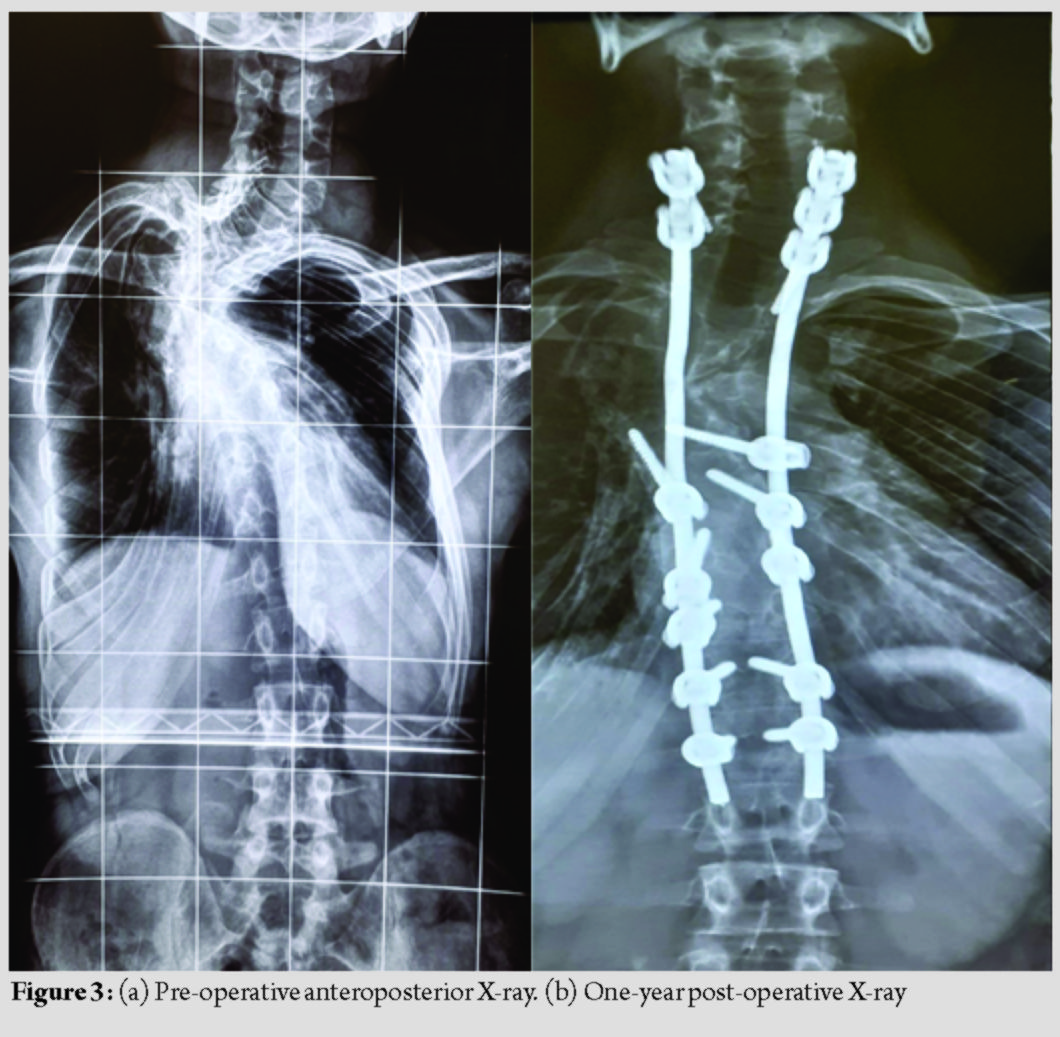 Copious amounts of morselized autologous bone graft were placed posteriorly to promote posterior bony fusion. Time for surgery was 4.5 h. Blood loss was 800 ml. There were no intraoperative adverse events. The post-operative period was uneventful. Kyphosis was corrected from 100° to 65° and scoliosis (Coronal Cobbs angle) was corrected from 100° to 60°. The patient was back to full functional status. At 1-year follow-up, good fusion was achieved, as seen on the X-ray (Fig. 3a and b and 4a and b).
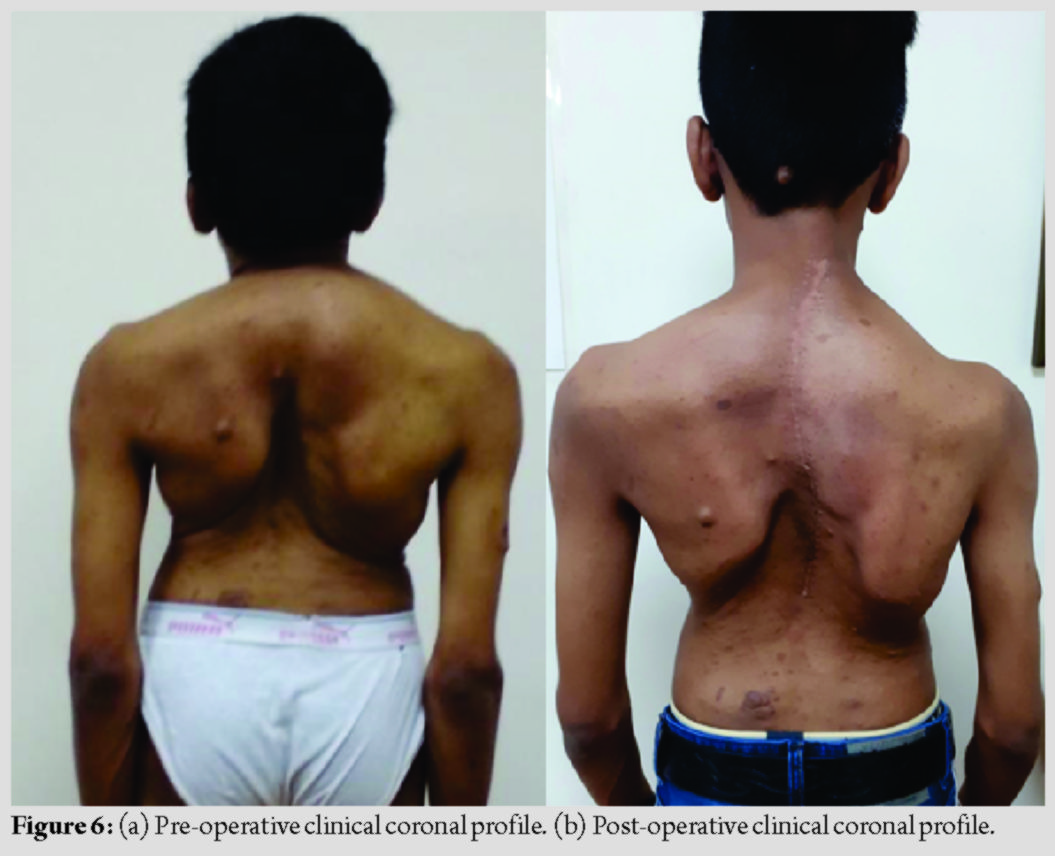
Copious amounts of morselized autologous bone graft were placed posteriorly to promote posterior bony fusion. Time for surgery was 4.5 h. Blood loss was 800 ml. There were no intraoperative adverse events. The post-operative period was uneventful. Kyphosis was corrected from 100° to 65° and scoliosis (Coronal Cobbs angle) was corrected from 100° to 60°. The patient was back to full functional status. At 1-year follow-up, good fusion was achieved, as seen on the X-ray (Fig. 3a and b and 4a and b).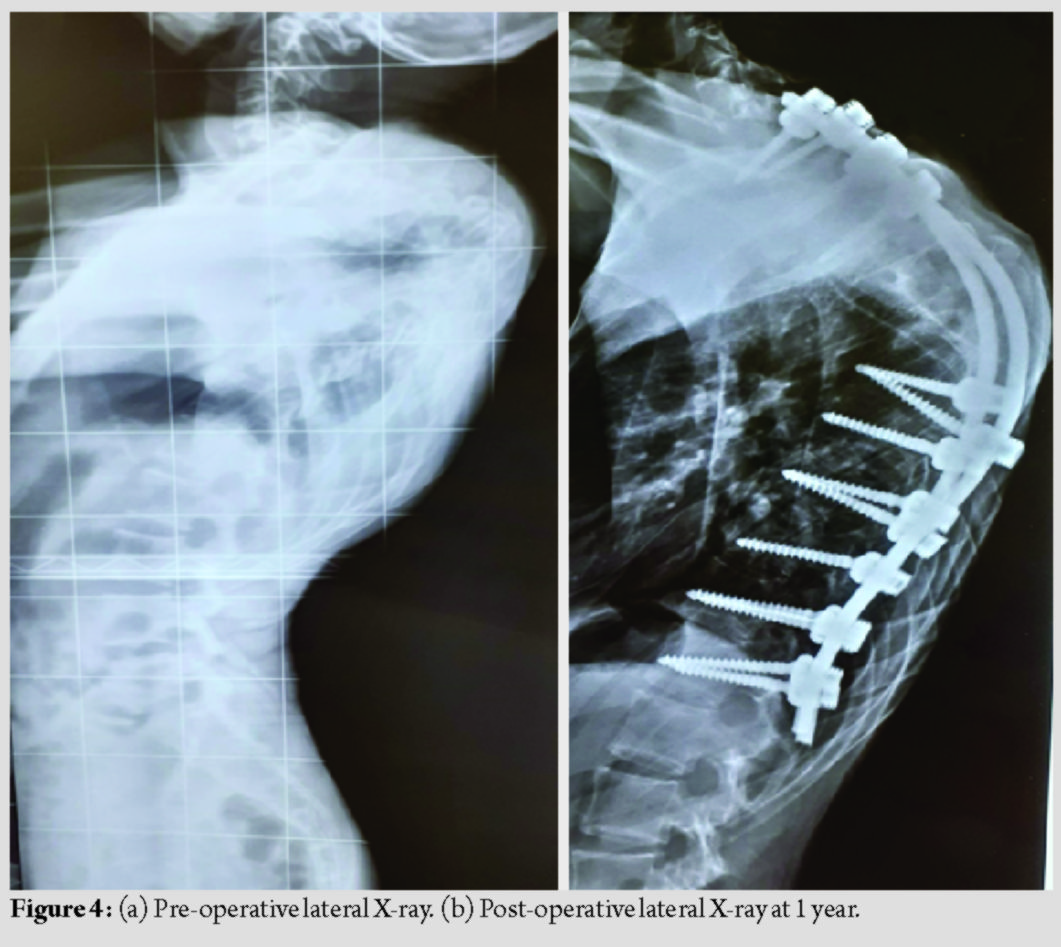 There was no coronal or sagittal imbalance at end of 1 year and upper back hump was cosmetically better compared to pre-operative (Fig. 5a and b) (Fig. 6a and b).
There was no coronal or sagittal imbalance at end of 1 year and upper back hump was cosmetically better compared to pre-operative (Fig. 5a and b) (Fig. 6a and b).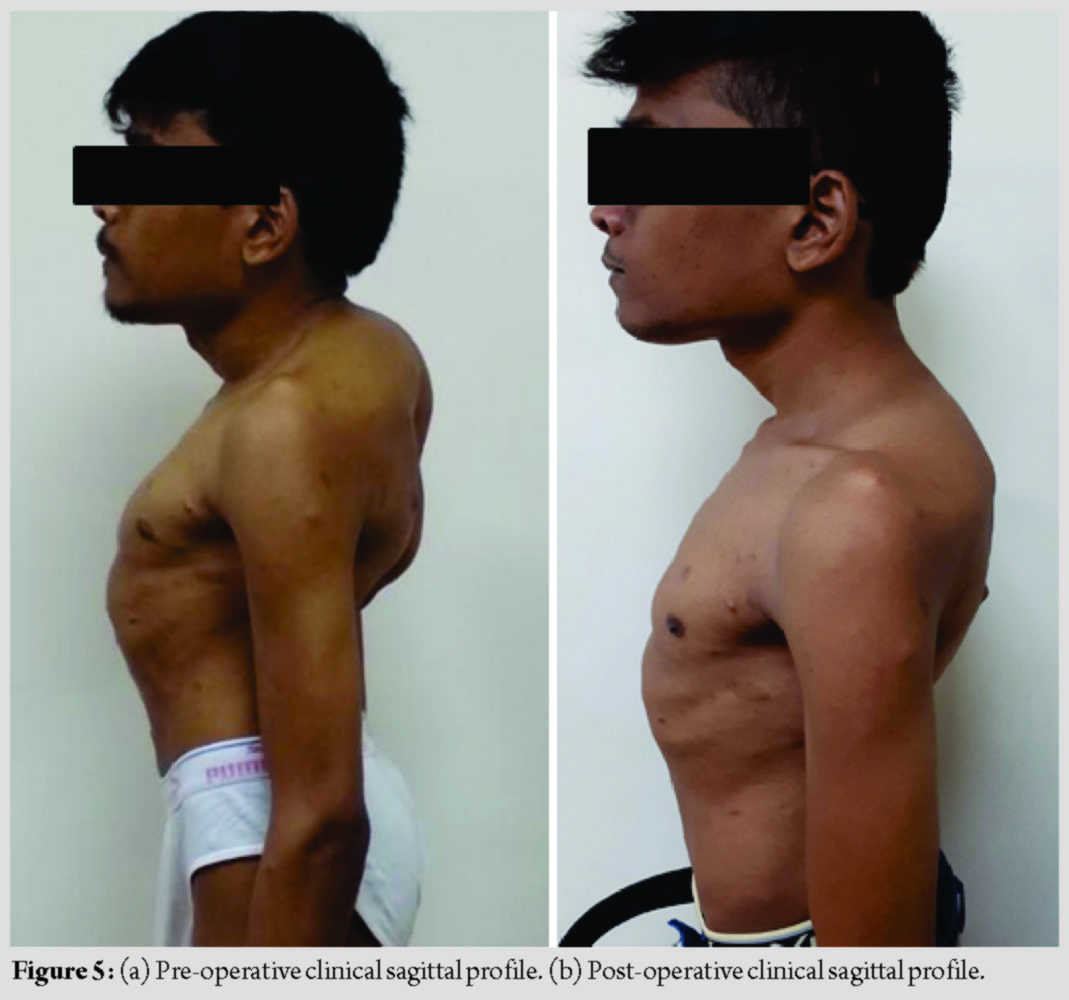
Discussion
NF-1 is an autosomal dominant disorder. Scoliosis is seen in about 10–64% of NF-1 [1, 3]. The prevalence of NF-1 is 1:3000 [8, 9]. Curves are dystrophic or non-dystrophic type. Non-dystrophic curves usually present like idiopathic scoliosis [10]. Tsirikos et al. [11] reported that dystrophic curves <20° should be closely observed and a sudden progression in the curve should be considered for surgery. Dystrophic curves more than 20° generally require surgery. The approach for surgery in such patients remains unresolved. The choice is between a combined anterior plus posterior fusion and an all posterior fusion. Kim and Weinstein [12] believed that dystrophic scoliotic curves of 20–40° and kyphosis <50° can be managed with posterior spinal instrumented fusion only. To obtain better correction and avoid pseudoarthrosis, anteroposterior fusion was recommended when dystrophic scoliosis was greater than 40° and/or kyphosis was greater than 50°. The efficacy of anterior surgery is often compromised due to hyperkyphosis and vertebral rotation according to some authors [3, 13]. The presence of tumor or excessive plexiform venous channels around the vertebral bodies sometimes makes it impossible to approach the apex of the curve anteriorly. Due to dystrophy, apical vertebrae can be significantly subluxated and malaligned from rest of the spine. Such malalignment does not allow anterior strut grafts to be placed in the concavity of the kyphosis, and hence, they are mechanically ineffective in preventing its progression [14]. Some authors have described the use of pre-operative halo gravity traction, especially in rotatory subluxation of vertebrae in NF-1 dystrophic curve to minimize risk of correction surgery, improve flexibility of the curve and pre-operative pulmonary function [6, 7]. We concluded that pre-operative traction in such a patient may not be as effective in distracting the apex of the deformity as there was partial fusion observed at the apex of the deformity, especially the D5-D6 vertebra. In our opinion, the purpose of surgery in these cases is to stabilize the vertebral column and halt further progression of deformity rather than aiming for full correction of the curve. We believe that kyphosis correction through the anterior approach would have been difficult, in such a lesion in the upper thoracic spine due to the deep, high apex, and crowding of the vital structures around this region. We also observed in the radiological investigations that the dysplastic vertebra of D5 was posteriorly sequestered with the vertebra of D4 and D6 partially covering it anteriorly. In our opinion, the access to the D5 vertebra in such a situation would have been less than adequate anteriorly, leading to the possibility of incomplete excision of the D5 vertebra and the posterior bony knuckle caused by it. According to the recently published guidelines of management of kyphosis by Rajasekaran et al., this patient was considered to be a Type III B type of kyphosis [15]. The authors recommended doing a posterior vertebrectomy and posterior fixation with or without a pre-operative halo gravity traction. Keeping in mind the aim of our surgery to stabilize the kyphosis and prevent further progression of the deformity, along with removing the offending bony knuckle of the D5 vertebra causing the pressure on the cord, we chose to do a three column osteotomy at the apex D5 level and posterior fixation from C7 to T2 and T8-L1 fixation along with titanium rods. We did not excise the whole of the D5 body, but left behind the endplates of the D5 body, on which the osteotomy was closed. This we chose to do keeping in mind the higher rates of pseudoarthrosis in NF-1. We tried to eliminate the need of a metallic mesh cage with autologous bone graft and instead chose to keep the native bone to bone contact and augmented the posterior fusion bed with the remaining autologous bone. We managed to achieve an acceptable kyphosis correction from 100° to 65° and scoliosis correction from 100° to 60°. These measurements remained same at the end of 1 year follow-up with a good fusion status, as seen on the X-ray. There was excellent cosmetic improvement of the upper back deformity and no further progression of the myelopathy in the patient. The limitations of this report are the short period of post-operative follow-up and lack of documentation of the fusion status by a CT scan. We usually avoid doing regular CT scans on our patients when we observe on the X-ray that there is no implant loosening, loss of correction, or progression of the deformity.
Conclusion
Proximal thoracic dystrophic kyphoscoliosis with cord compression causing early myelopathic symptoms and signs in NF type 1 can be treated with single Stage 3 column osteotomy with posterior fixation by an all posterior approach with acceptable cosmetic and neurological outcomes.
Clinical Message
Proximal thoracic kyphosis is not clinically visible unless it is of higher degree. Early myelopathic symptoms and signs should be picked up. NF-1 with proximal thoracic kyphosis can be managed by 3 column osteotomy from all posterior approach.
References
1. Akbarnia BA, Gabriel KR, Beckman E, Chalk D. Prevalance of scoliosis in neurofibromatosis. Spine (Phila Pa 1976). 1992;17 Suppl 8:S244-8.
2. Halmai V, Domán I, de Jonge T, Illés T. Surgical treatment of spinal deformities associated with neurofibromatosis Type 1: Report of 12 cases. J Neurosurg 2002;97 Suppl 3:310-6.
3. Crawford AH. Pitfalls of spinal deformity associated with neurofibromatosis in children. Clin Orthop Relat Res 1989;245:29-42.
4. Khong PL, Winnie HS, Virginia CN, Fung CW, Ooi GC. Imaging of spinal tumors in children with neurofibromatosis 1. Am J Roentgenol 2003;180:413-7.
5. Funasaki H, Winter R, Lonstein J, Denis F. Pathophysiology of spinal deformities in neurofibromatosis. An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
6. Garabekyan T, Hosseinzadeh P, Iwinski H. Results of preoperative halo-gravity traction in children with severe spinal deformity. J Pediatr Orthop B 2014;23:1-5.
7. Nemani V, Kim H, Bjerke-Kroll B, Yagi M, Akoto H, Papadopoulos EC, et al. Preoperative halo-gravity traction for severe spinal deformities at an SRS-GOP site in West Africa: Protocols, complications, and results. Spine 2015;40:153-61.
8. Crawford AH, Schorry EK. Neurofibromatosis update. J Pediatr Orthop 2006;26:413-23.
9. Littler M, Morton N. Segregation analysis of peripheral Neurofibromatosis (Nf1). J Med Genet 1990;27:307-10.
10. Crawford AH, Parikh S, Schorry EK, Von Stein D. The immature spine in Type-1 neurofibromatosis. J Bone Joint Surg Am 2007;89:123-42.
11. Tsirikos AI, Saifuddin A, Noordeen MH. Spinal deformity in neurofibromatosis Type-1: Diagnosis and treatment. Eur Spine J 2005;14:427-39.
12. Kim HW, Weinstein SL. Spine update. The management of scoliosis in neurofibromatosis. Spine (Phila Pa 1976) 1997;22:2270-6.
13. Crawford AH, Herrera-Soto J. Scoliosis associated with neurofibromatosis. Orthop Clinic North Am 2007;38:553-62.
14. Hsu LC, Lee PC, Leong JC Dystrophic spinal deformities in neurofibromatosis. Treatment by anterior and posterior fusion. J Bone Joint Surg Br 1984;66:495-9.
15. Rajasekaran S, Kanna R, Shetty AP, Kanna R, Shetty AP. Classification for kyphosis based on column deficiency, curve magnitude, and osteotomy requirement. J Bone Joint Surg Am 2018;100:1147-56.
 |
 |
 |
 |
| Dr. Munjal S Shah | Dr. Kutbuddin Akbary | Dr. Priyank M Patel | Dr. Abhay M Nene |
| How to Cite This Article: Shah MS, Akbary K, Patel PM, Nene AM. Management of proximal thoracic kyphoscoliosis with early myelopathy in a young adult with neurofibromatosis type 1: A case report and review of literature. Journal of Orthopaedic Case Reports 2020 July;10(4): .8-12 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Impaired Bone Healing and Fracture Complications during Limb Lengthening in a Neurofibromatosis Type 1 Patient Receiving Selumetinib: Case Report and Literature Review
February 1, 2026 Impaired Bone Healing and Fracture Complications during Limb Lengthening in a Neurofibromatosis Type 1 Patient Receiving Selumetinib: Case Report and Literature Review July 10, 2022 Cervical Kyphosis due to Neurofibromatosis Type 1 Treated by Circumferential Spinal Fusion using an Autologous Vascularized free Fibula Followed by Teriparatide Administration: A Case Report
July 10, 2022 Cervical Kyphosis due to Neurofibromatosis Type 1 Treated by Circumferential Spinal Fusion using an Autologous Vascularized free Fibula Followed by Teriparatide Administration: A Case Report March 10, 2023 Medial Swivel Dislocation of the Talonavicular Joint Due to High-Energy Trauma: A Case Report
March 10, 2023 Medial Swivel Dislocation of the Talonavicular Joint Due to High-Energy Trauma: A Case Report July 30, 2019 Neglected Posttraumatic Atlantoaxial Spondyloptosis with Type 2 Odontoid Fracture: A Case Report
July 30, 2019 Neglected Posttraumatic Atlantoaxial Spondyloptosis with Type 2 Odontoid Fracture: A Case Report