
[box type=”bio”] Learning Point of the Article: [/box]
Total Elbow Arthroplasty is the salvage treatment option for Elbow Mobility in middle aged sedentary worker with secondary bone loss.
Case Report | Volume 10 | Issue 4 | JOCR July 2020 | Page 63-65 | R. Sivakumar, V. Somashekar, Prahalad Kumar Shingi, M. Chidambaram. DOI: 10.13107/jocr.2020.v10.i04.1804
Authors: R. Sivakumar[1], V. Somashekar[1], Prahalad Kumar Shingi[1], M. Chidambaram[1]
[1]Department of Orthopaedics, Preethi Hospitals, Uthangudi, Madurai, India.
Address of Correspondence:
Dr. V. Somashekar,
Department of Orthopaedics, Preethi Hospitals ( P) Ltd., No. 50, Melur Main Road, Uthangudi, Madurai – 625 107, Tamil Nadu. India.
E-mail: somuortho@gmail.com
Abstract
Introduction: Total elbow arthroplasty (TEA) is a viable treatment for pain-free mobility in stiff elbow of sedentary patients with rheumatoid arthritis and ankylosis. Secondarily, TEA is useful in cases of stiff failed fixation and bone loss of distal humerus fractures.
Case Report: A Fifty one years old sedentary male presented to our institute with a history of injury to the right elbow (sideswipe injury). On clinical and radiological examination, it was open Grade III B fracture of distal humerus with bone loss. He was treated with wound debridement and initial temporary fixation with k-wires and later soft-tissue reconstruction. One year later, the patient upper limb was flail, limited range of motion (passive 40° 70°) and no infection. Radiology revealed non-union of condylar fragments with bone loss of distal humerus. The patient underwent TEA through standard triceps reflecting approach. He was implanted cemented modular Coonrad-Murray semi-constrained prosthesis Type III. The post-operative period was uneventful. At 4-year follow-up, the patient is pain free with elbow range of motion 5°120°.
Conclusion: In failed osteosynthesis and sedentary patients, TEA is a SALVAGE surgery for pain-free mobility with its own long-term limitations.
Keywords: Post-traumatic arthritis, total elbow arthroplasty, non-union distal humerus.
Introduction
Total elbow arthroplasty (TEA) is a viable treatment for pain-free mobility in stiff elbow of sedentary patients with rheumatoid arthritis and ankylosis. Secondarily, TEA is also useful in cases of failed fixation with stiffness and bone loss of distal humerus fractures. Unlike other arthroplasties of hip and knee, TEA may not be considered as primary treatment. Elbow is a complex joint involving four articulations and also complex biomechanics come into play. Certainly, TEA gives satisfactory results in complex post-traumatic bone loss around the elbow.
Case Report
A 51-year-old male presented to our institute with a history of injury to right elbow (sideswipe injury). On clinical and radiological examination, it was open Grade III B fracture of distal humerus with bone loss (Fig. 1). He was operated with wound debridement and initial temporary fixation with k-wires and later soft-tissue reconstruction.
One year later, the patient did not show any signs of infection and was essentially flail limb, with a limited range of motion (passive range of motion 40° 70°). Radiology revealed the non-union of condylar fragments with bone loss (Fig. 2). We advised TEA as a treatment option as he was a sedentary office worker with deliberate discussion about the advantages as well as long-term prognosis.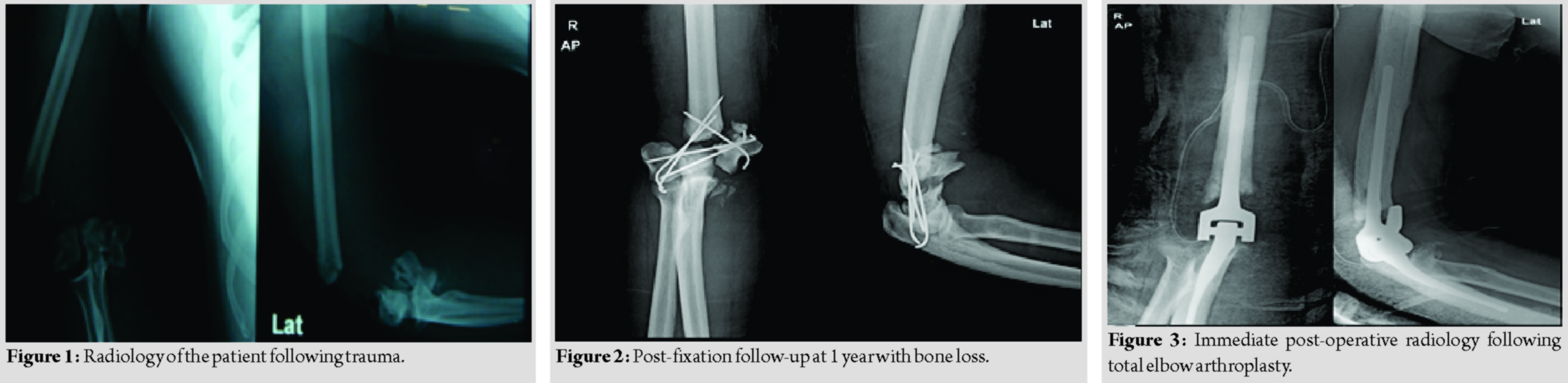 After routine evaluation for surgery, the elbow was approached in lateral position through the previous scar posteriorly. Triceps were reflected off subperiosteally [1]. Humerus and ulna prepared, there were no condyles per say only distal humerus. After cementing a modular Coonrad-Murray semi-constrained prosthesis implanted. Triceps sutured back with no. 5 Ethibond. Soft padding dressing done (Fig. 3).
After routine evaluation for surgery, the elbow was approached in lateral position through the previous scar posteriorly. Triceps were reflected off subperiosteally [1]. Humerus and ulna prepared, there were no condyles per say only distal humerus. After cementing a modular Coonrad-Murray semi-constrained prosthesis implanted. Triceps sutured back with no. 5 Ethibond. Soft padding dressing done (Fig. 3). The patient followed a regular follow-up with elbow range of motion exercises as pain tolerated. Strengthening exercises were avoided. The patient cautioned not lifting more than 1 lb for 3 months and after surgery not >5 lb with an operated arm.
The patient followed a regular follow-up with elbow range of motion exercises as pain tolerated. Strengthening exercises were avoided. The patient cautioned not lifting more than 1 lb for 3 months and after surgery not >5 lb with an operated arm.
At 4-year follow-up (Fig. 4), the patient is pain free with elbow range of motion from 5 to 125 degrees (Fig. 5-8).
Discussion
TEA is a relatively specialized procedure with few surgeons performing this operation frequently [2]. The functional range for elbow includes 30130 and 50° in supination pronation. Biomechanically loss of 50% elbow motion equals 80% total loss of upper limb mobility. Resection and anatomical arthroplasty were commonly performed between 1885 and 1947. Constrained, metal-to-metal, partial, and total hinge arthroplasties were in vogue between 1947 and 1970. It was in 1973, the original Coonrad total elbow replacement (Zimmer, Warsaw, and Indiana) (Type – I) incorporated high-molecular-weight polyethylene bushings but had only 2°–3° of laxity, subsequently came Type II with more valgus varus laxity [3]. At present, Type III is available [4, 5] with PMMA interposition with good laxity and anterior flange in humeral component. Arthrodesis may still be an alternative in the manual laborers or individuals who can compensate for loss of movement. However, arthrodesis is seldom now considered to be acceptable by patients [6]. Gill and Morrey [4], in their study of 69 patients with 78 Coonrad-Morrey TEAs with over 10 years for RA, concluded that prosthesis survival rate 92.4%, with 86% good or excellent results (results almost comparable to THA). With different implants, Little et al. [2] compared 33 Souter-Strathclyde, 33 Kudo, and 33 Coonrad-Morrey TEAs for rheumatoid arthritis. He concluded similar results in terms of pain relief (+ +) and functional improvement (moderate), but better survival after Coonrad- Morrey (less dislocations). When using TEA for Trauma, Frankle et al. [7] in older women showed that osteosynthesis group had problems of stiffness and failure of fixation. TEA group had ulnar nerve issues, infection, and implant fracture. They concluded that TEA to be a viable treatment option for distal intra-articular humerus fractures in women older than 65 years, especially if the patient had comorbidities such as rheumatoid arthritis, osteoporosis, and systemic steroid use. In a retrospective study by Sørensen et al. involving 24 complex distal humerus fractures operated with TEA AO Type B3 or C3 fracture and severe rheumatoid arthritis aged more than 65 years had mean follow-up of 21 months. Mayo Elbow Performance Score there were 15 patients with excellent results, four good, one fair, and none poor concluding TEA on fractures of the distal humerus in elderly patients can result in acceptable short- to medium-term outcome [8]. Treating distal humerus non-unions when an osteosynthesis has failed are demanding for the treating surgeon. Gandhi et al. treated seven such non-unions with a mean age of 72 and the number of operations per patient before TEA was 2.3 with a gap of 10 years from trauma to TEA. Average follow-up was 24 months, range improved in flail limb at pre-TEA to functional range of pain-free motion with mean flexion of 137° at post-TEA. They conclude that TEA can achieve excellent functional and patient-reported outcomes in distal humeral non-unions even after a failed osteosynthesis [9].
Conclusion
Osteosynthesis is a treatment for distal humerus fractures in young and with good bone quality. TEA is a viable treatment in patients with severe rheumatoid arthritis of limited functional demands. In failed osteosynthesis and sedentary patients, TEA is a SALVAGE surgery for pain-free mobility with its own long-term limitations.
Clinical Message
TEA is the salvage treatment option for elbow mobility in middle-aged sedentary worker with secondary bone loss.
References
1. Bryan RS, Morrey BF. Extensive posterior exposure of the elbow. A triceps-sparing approach. Clin Orthop Relat Res 1982;166:188-92.
2. Little CP, Graham AJ, Carr AJ. Total elbow arthroplasty: A systematic review of the literature in the English language until the end of 2003. J Bone Joint Surg Br 2005;87:437-44.
3. Aldridge JM 3rd, Lightdale NR, Mallon WJ, Coonrad RW. Total elbow arthroplasty with the Coonrad/Coonrad-Morrey prosthesis. A 10- To 31-year survival analysis. J Bone Joint Surg Br 2006;88:509-14.
4. Gill DR, Morrey BF. The Coonrad-Morrey total elbow arthroplasty in patients who have rheumatoid arthritis. A ten to fifteen-year follow-up study. J Bone Joint Surg Am 1998;80:1327-25.
5. Gschwend N, Simmen BR, Matejovsky Z. Late complications in elbow arthroplasty. J Shoulder Elbow Surg 1996;5:86-96.
6. Beckenbaugh RD. Arthrodesis. In: Morrey BF, editor. The Elbow and its Disorders. 3rd ed. Philadelphia, PA: W.B. Saunders Co.; 2001. p. 731-7.
7. Frankle MA, Herscovici D Jr., DiPasquale DG, Vasey MB, Sanders RW. A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intraarticular distal humerus fractures in women older than age 65. J Orthop Trauma 2003;17:473-80.
8. Sørensen BW, Brorson S, Olsen BS. Primary total elbow arthroplasty in complex fractures of the distal humerus. World J Orthop 2014;5:368-72.
9. Gandhi MJ, Moores TS, Malhotra A, Hay SM. Total elbow arthroplasty for management of distal humeral nonunions. Tech Shoulder Elb Surg 2018;19:97-100.
 |
 |
 |
 |
| Dr. R. Sivakumar | Dr. V. Somashekar | Dr. Prahalad Kumar Shingi | Dr. M. Chidambaram |
| How to Cite This Article: Sivakumar R, Somashekar V, Shingi PK, and Chidambaram M. Total elbow arthroplasty as treatment of non-union with bone loss of distal humerus – A case report. Journal of Orthopaedic Case Reports 2020 July;10(4): 63-65. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


