
Retrograde Hooked Guide Wire Surgical Technique is easy, simple, biological, cost effective, does not need any special device and also avoid any new incision, bone drilling, or opening of fracture site.
Dr. Bipul K Garg,
Department of Orthopaedic Surgery,
Sir J.J. Group of Hospitals and Grant Medical College, Mumbai, Maharashtra, India.
E-mail: garg.bipul@gmail.com
Abstract
Introduction: Removal of a distal piece of a broken nail often possesses a technical challenge. Several methods have been described in the past to extract a distal piece by using specialized instruments like such as hooks, olive wires, and talwalkar radial square nail etc. It is difficult to extract a distal piece from a proximal incision site and often fracture or the nonunion site has to be opened. In this article, we describe a novel technique to extract a distal piece of broken intramedullary tibia nail by retrograde manner using a guide wire with a “‘U”’ shaped bend at its distal end to hook the tip of a distal piece of broken nail and help in extraction.
Case Report: A 43- year-s old male presented with complain of pain in left leg since 3 months. Patient had sustained left- sided compound Grade 2 tibia shaft fracture in a road traffic accident 4 years back. He was operated with tibia interlock nail followed by skin grafting for wound coverage in a different facility. On clinical examination: There was tenderness around distal tibia, no swelling, no coronal or sagittal plane fracture mobility, and no crepitus or loss of transmitted movements which suggested fracture union clinically. Radiographs confirmed complete union of tibia shaft fracture with hypertrophic nonunion of distal fibula with broken intramedullary nail IMN at the level of proximal most screw hole of distal locking holes with both distal locking screws broken. As fracture was united, we planned for removal of broken nail without opening fracture site. For extraction for distal tibial broken nail part, we used this new Retrograde Hooked Guide Wire technique.
Conclusion: It is a simple, cost effective, minimally invasive procedure with minimal blood loss and decrease time of surgery that can be used before attempting more invasive extraction methods and hence should be included in standard procedures for extraction.
Keywords: Tibia, interlock nail, broken nail, retrograde guide wire, nail removal.
Intramedullary nail (IMN) is currently considered the treatment of choice for most of the lower limb long bone diaphyseal fractures. Nail is a load sharing implant with a simple operative technique. It allows for stability as well as for a biologically and mechanically advantageous environment for fracture healing with minimal surrounding soft-tissue damage. Despite all this advantages, IMN as an implant is not without complications. Common long-term complication include nail failure due to metal fatigue secondary to non-union without significant deformity of metal and plastic deformation of the nail before definitive union of the bone. Several techniques [1,2,3,4,5,6,7,8,9,10,11]] have been described in literature to extract broken distal nail piece by opening the fracture or non-union site or using specialized instruments such as hooks, olive wires, talwalkar radial square nail. Here, we describe a newer simple and cost-effective technique to extract distal broken nail piece without opening fracture or non-union site using a guidewire in retrograde manner with a “U” shaped bend at distal end to engage the broken distal nail piece and remove it from proximal entry site.
A 43-year-old male presented to outpatient department with complain of pain in left leg since 3 months. Patient had sustained left-sided compound Grade 2 tibia shaft fracture in a road traffic accident 4 years back. He was operated with tibia interlock nail followed by skin grafting for wound coverage in a different facility. On clinical examination: There was tenderness around distal tibia and ankle, no swelling, no coronal or sagittal plane fracture mobility, and no crepitus or loss of transmitted movements which suggested fracture union clinically. Radiographs (X-ray tibia Anteroposterior and Lateral) confirmed complete union of tibia shaft fracture with hypertrophic nonunion of distal fibula with broken IMN at the level of proximal most screw hole of distal locking holes with both distal locking screws broken (Fig. 1). As fracture was united, we planned for removal of broken nail without opening fracture site.

Under spinal anesthesia, patient was placed supine on operative table. First, proximal interlocking screws were removed. The proximal part of broken nail was removed using a universal nail extractor from the nail entry site.
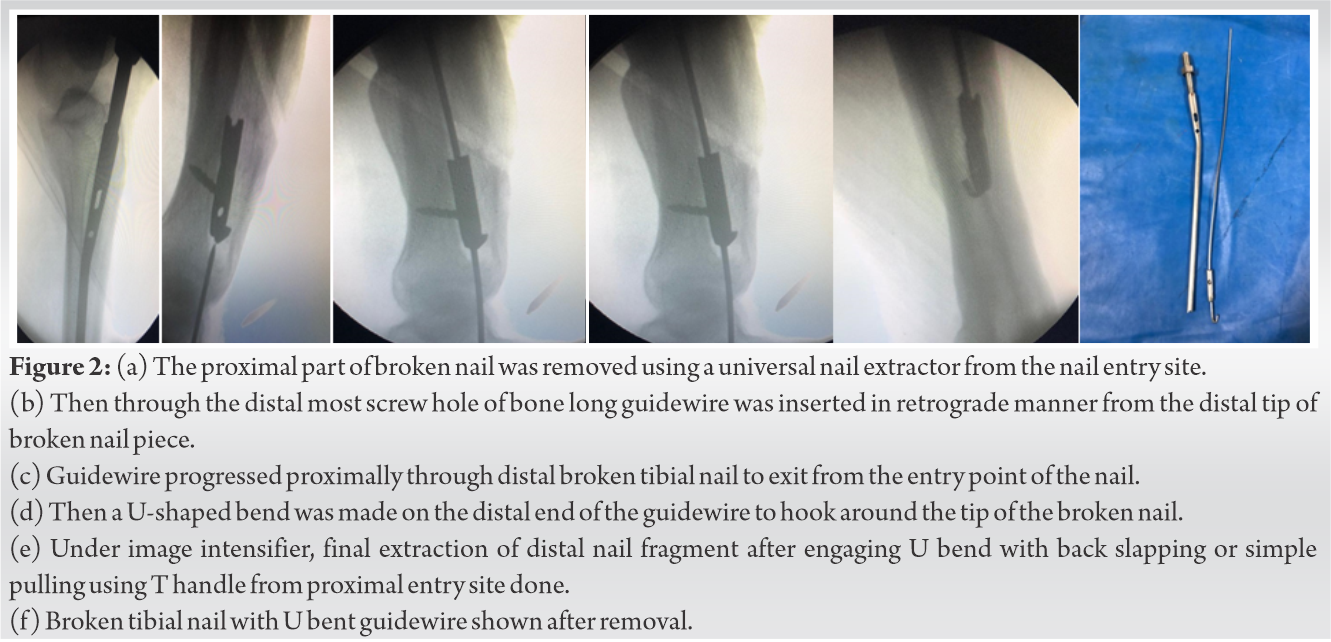
Then, the distal broken screws were removed. Mosquito forceps were then inserted through the distal most screw hole and engaged into the nail and then using this mosquito forceps, nail piece was pushed proximally so that now the distal most end of nail piece laid at the level of screw hole. Then through the distal most screw hole (of bone), long guidewire was inserted in retrograde manner from the distal tip of broken nail piece and progressed proximally through it to exit from the entry point of the nail. Then, a U-shaped bend was made on the distal end of the guidewire to hook around the tip of the broken nail. Under image intensifier, final extraction of distal nail fragment after engaging U bend with back slapping or simple pulling using T handle from proximal entry site done (Figs. 2 and 3). Thorough wound wash was given and wound was closed in layers.
Nail breakage is a known complication of IMN fixation of tibial fractures. Close removal of the broken distal nail piece can be a very hard task to achieve. Several techniques have been described for the extraction of the distal nail piece. Some of them required specific instruments while others required opening of fracture or nonunion site. The AO-recommended technique involves extraction of the proximal fragment followed by over-reaming of the medullary canal down to the distal nail fragment and extraction of distal broken piece using extraction hook [1]. Brewster et al. modified the AO-recommended technique using several guidewires impacted around the hook to form a stable construct which could easily be removed as one piece but requires the use of several pieces of equipment and substantial force for removal [2]. Abdelgawad et al. described a technique using small distractor hook and a small (~2 in) piece of flexible nail [3]. Charnley and Farrington used Petelin laparoscopic grasping forceps to extract the distal segment of a broken cannulated tibial IMN under fluoroscopic guidance. Levine and Georgiadis made a hole in medial malleolus to reach nail tip and used ball-tipped guide wire to extract the distal broken piece retrogradely [4]. Khan et al. recommended a technique using a hand-reamer and Sivananthan et al. suggested impaction of a smaller nail into the opening of the distal nail fragment [5,6]. These methods are not applicable to the new generation of nails with small inner holes, which are constructed for passage of only a guidewire [5]. J.A. Gill et al used strykers implant extractor system that may add significantly to the total cost and can be difficult to be arranged in remote areas [7]. In general, regardless of the method used, good planning is of utmost importance to ensure that adequate and necessary tools are present during surgery. The technique described here can be applied to all cannulated nails and does not need any special device and also avoid any new incision, bone drilling or opening of fracture site. Hence, it avoids soft-tissue damage, periosteal stripping, and risk of infection that may adversely affect the fracture union. Every techniques have some drawbacks as so our technique. Although it can be one of the option for broken nail removal, it cannot be accepted for all cases as in snug fitting nail (which is preferable) or in long standing cases with no infection, a simple maneuver of pushing the nail up with mosquito forceps might not always be possible. If thicker guidewire is used, it is difficult to bent distally and put inside medullary canal. If thinner wire is used, while pulling from above hook can be straighten due to angulation at the union/non-union site.
The above described method is easy, simple, biological, and cost effective and would be of definite use especially in an average orthopedic setup where implant removal instrumentation is not readily available.
The technique described here can be applied to all cannulated nails and does not need any special device and also avoid any new incision, bone drilling or opening of fracture site. Hence, it avoids soft-tissue damage, periosteal stripping, and risk of infection that may adversely affect the fracture union.
References
- 1.Muller ME, Allowger M, Schneider R, Willeneger H. Manual of Internal Fixation: Technique Recommended by the Ao-Asif Group. 2nd ed. Berlin: Springer Verlag; 1979. p. 158. [Google Scholar | PubMed]
- 2.Brewster NT, Ashcroft GP, Scotland TR. Extraction of broken intramedullary nails: An improvement in technique. Injury 1995;26:286. [Google Scholar | PubMed]
- 3.Abdelgawad AA, Kanlic E. Removal of a broken cannulated intramedullary nail: Review of the literature and a case report of a new technique. Case Rep Orthop 2013;2013:461703. [Google Scholar | PubMed]
- 4.Levine JW, Georgiadis GM. Removal of a broken cannulated tibial nail: A simple intramedullary technique. J Orthop Trauma 2004;18:247-9. [Google Scholar | PubMed]
- 5.Khan M, Schranz PJ, Ward MW. Removal of a broken intramedullary tibial nail using a hand reamer. Injury 1997;28:693-4. [Google Scholar | PubMed]
- 6.Sivananthan KS, Raveendran KK, Kumar T, Sivananthan S. A simple method for removal of a broken intramedullary nail. Injury 2000;31:433-4. [Google Scholar | PubMed]
- 7.Gil JA, McClure P, Born CT. Removal of the distal aspect of a broken tibial nail. Am J Orthop 2017;46:112-5. [Google Scholar | PubMed]
- 8.Hak DJ, McElvany M. Removal of broken hardware. J Am Acad Orthop Surg 2008;1:16:113-20. [Google Scholar | PubMed]
- 9.Blake SM. A technique for the removal of the distal part of a broken intramedullary nail. Ann R Coll Surg Eng 2009;91:169-70. [Google Scholar | PubMed]
- 10.Sidky A, Buckley RE. Hardware removal after tibial fracture has healed. Can J Surg 2008;51:263-8. [Google Scholar | PubMed]
- 11.Reith G, Schmitz-Greven V, Hensel KO, Schneider MM, Tinschmann T, Reith GB, Greven SV, Hensel KO, et al. Metal implant removal: Benefits and drawbacks-a patient survey. BMC Surg 2015;15:96. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Primary Bone Lymphoma of the Tibia Mimicking Chronic Osteomyelitis: A Case Report
November 1, 2025 Primary Bone Lymphoma of the Tibia Mimicking Chronic Osteomyelitis: A Case Report November 1, 2025 Locking Plate Fixators for Infected Extra-articular Long Bone Fractures without Bone Loss
November 1, 2025 Locking Plate Fixators for Infected Extra-articular Long Bone Fractures without Bone Loss August 1, 2025 Histological Dedifferentiation in Recurrent Adamantinoma of the Tibia: A Case Report
August 1, 2025 Histological Dedifferentiation in Recurrent Adamantinoma of the Tibia: A Case Report October 1, 2024 Brodie’s Abscess of the Ankle Presenting as a Tumor: A Summary of Five Cases
October 1, 2024 Brodie’s Abscess of the Ankle Presenting as a Tumor: A Summary of Five Cases