
Children with pain and an inability to bear weight after water sliding together with an adult companion at their backs should raise suspicion among medical staff of a femoral neck fracture.
Dr. Guy Rubin,
Department of Orthopaedic, Emek Medical Center, Afula, Israel,
E-mail: guytalr@bezeqint.net
Abstract
Introduction: In contrast to adults, fractures of the neck of femur in children are relatively rare. The commonly described mechanism of injury is high energy trauma. Treatment options are almost always surgical. Prognosis, which entails relatively high rates of complications, varies with specific anatomic location, time to surgery, and reduction quality.
Case Report: We describe two cases of 10- and 12-year-old girls who suffered a fracture of the neck of the femur, Delbet Type II and Type III, respectively, due to a suspected hyper-abduction injury while sliding on a water slide. Both patients were treated surgically, with the younger one developing signs of femoral head avascular necrosis a year postoperatively.
Conclusion: Children with pain and an inability to bear weight after water sliding together with an adult companion at their backs should raise suspicion among medical staff of a femoral neck fracture. Prompt pediatric orthopedic consultation and treatment are needed in case of fracture diagnosis to reduce the risk of complications.
Keywords: Avascular necrosis, child, femoral neck fracture.
Fractures of the femoral neck in children and adolescents are relatively rare and are responsible for only a small fraction of the overall percentage of pediatric fractures [1]. Nonetheless, these fractures, regardless of the treatment method, may have high rate of complications, with avascular necrosis (AVN) of the femoral head being the direst one [2,3]. The Delbet classification [4], which was crafted by the French surgeon Pierre Delbet in the beginning of the 20th century and later developed by Colonna [5], addresses the anatomic location of the fracture line from the femoral head distally and may predict the possible risk for future AVN. As opposed to osteoporotic hip fractures in the elderly, pediatric femoral neck fractures in healthy individuals are considered a relatively high energy injury [6,7,8]. Water slide recreational injuries have been scarcely investigated in the literature. In 1983, Leonard et al. [9] described a cluster of injuries from waterslides with ten orthopedic injuries of which the vast majority were spinal column fractures. Malpass et al. [10] described a wide array of water slide injuries of which 7% were fractures. In 2016, a report from a water park in Jamaica described three open-book pelvic fractures in adults, all contributed to high velocity sliding with hyper-abduction of the legs [11]. In the present study, we present independent cases that, to the best of our knowledge, have yet to be described of two girls who suffered femoral neck fractures while sliding reluctantly on a water slide.
Two female patients, aged 10 and 12 years, were admitted to the Emergency Department of our institution after they had recreated in water amusement parks abroad and apparently suffered from an indirect hip trauma while sliding on a waterslide.
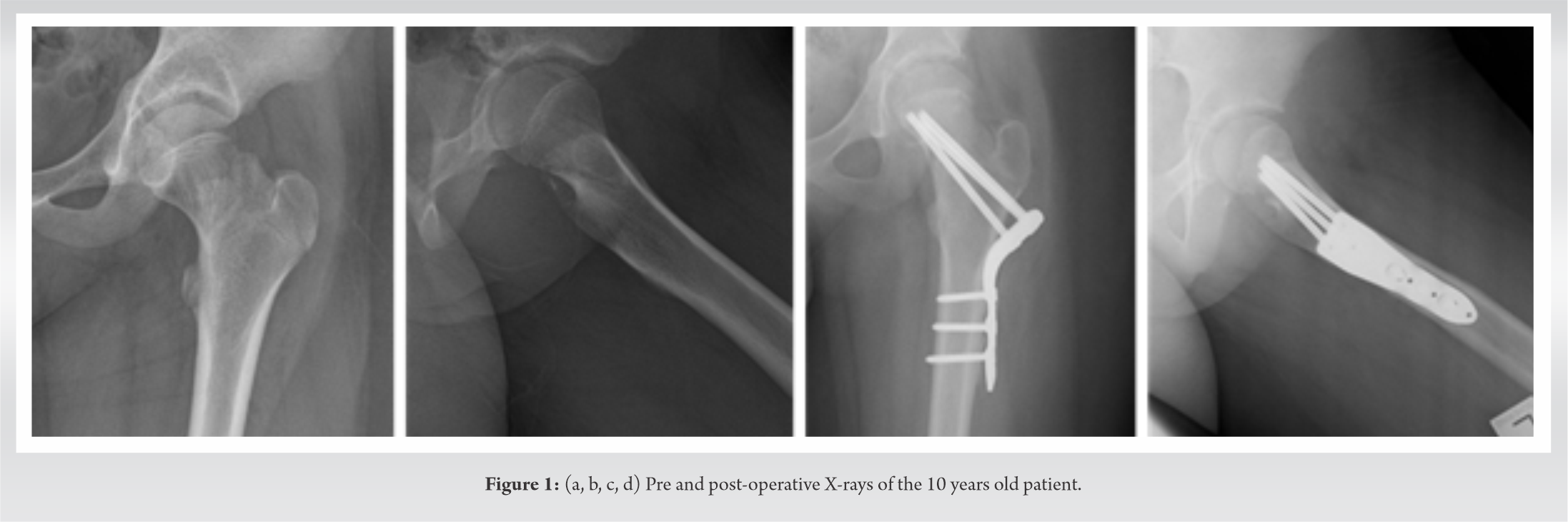
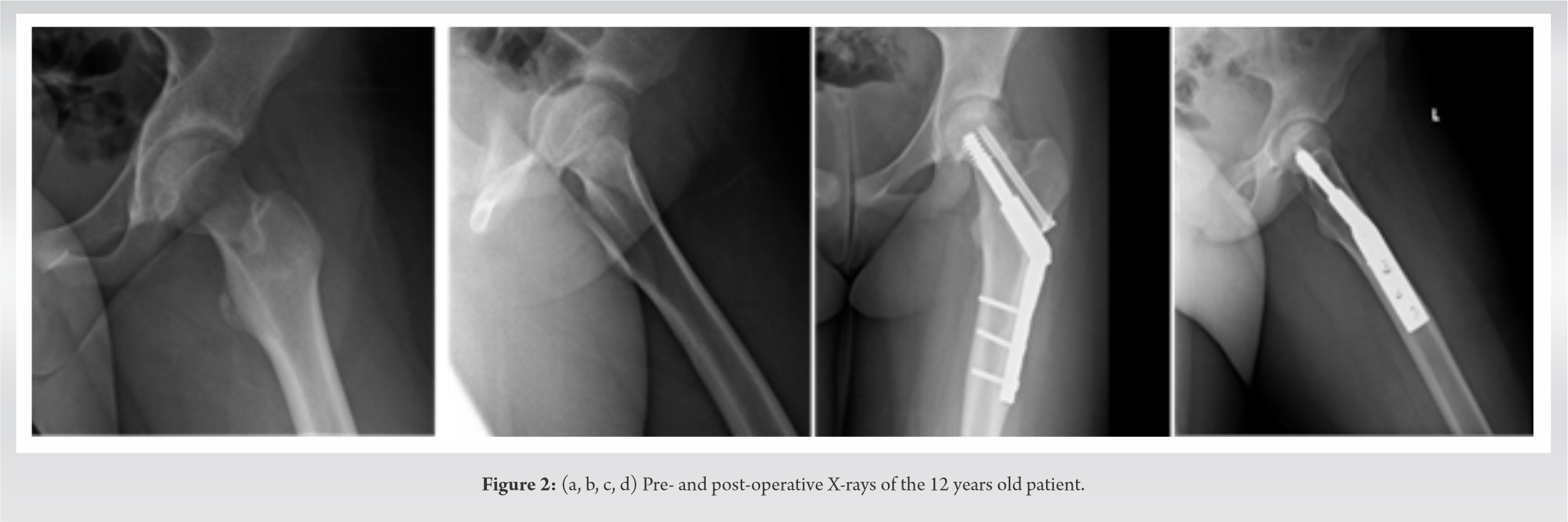
Both patients described how they reluctantly went down the waterslide with their fathers behind them at the back. Both girls apparently were trying to slow themselves down with their legs upfront. The two girls were unable to bear weight after sliding. On physical evaluation, both refused to bear weight on their left legs, and leg rolling tests was positive. Both had no other complaints. After physical clearance, the girls were X-rayed and diagnosed with hip fractures. The 10-year-old suffered a Delbet Type II fracture (Fig. 1a, b) while the 12-year-old had a Delbet Type III fracture (Fig. 2a, b). Both were admitted to the Pediatric Orthopedic Unit in our institution and were surgically treated, approximately 4 days after their initial injury, with closed reduction and internal fixation. The 10-year-old patient with the Delbet Type II fracture was fixated using NAa LCP Pediatric Hip Plate 5.0 (DePuy Synthes, Raynham, MA, USA) (Fig. 1c, d), as recommended by Beaty et al. [1]. The 12 years old patient, who suffered from the Delbet Type III fracture, was overweight for her age at roughly 65 kg. The surgeon’s intra-operative decision was to fixate her with more robust hardware, using an adult Compression Hip Screw (Smith and Nephew Richards, Memphis, TN, USA) augmented with a 7.5 mm cannulated screw to prevent rotation (Fig. 2c , d).
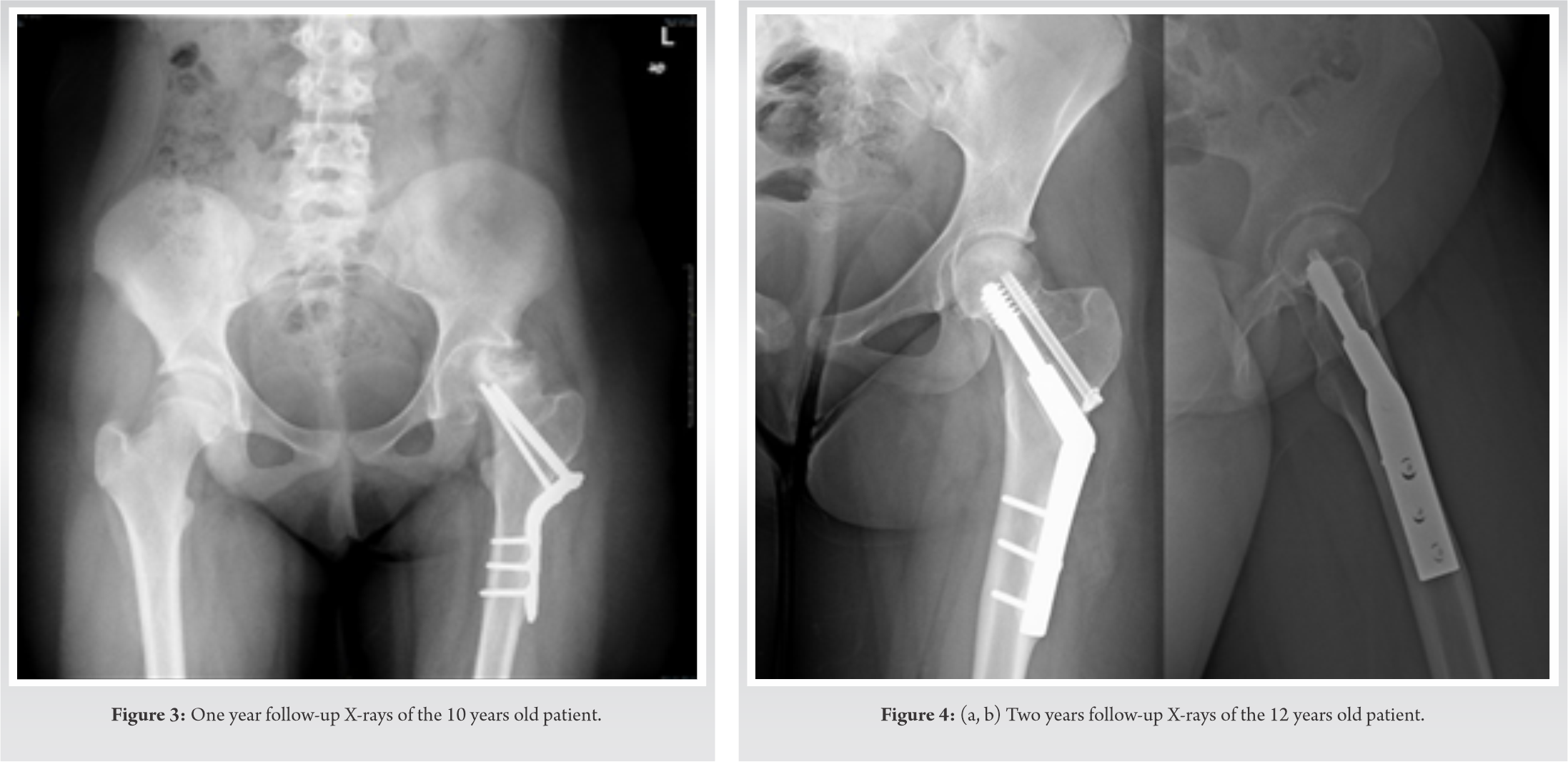
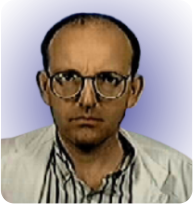
Both girls remained in hospital 4–5 days post-surgery for medical follow-up and intensive physiotherapy with non-weight bearing protocol. After discharge, both continued non-weights bearing physiotherapy for improving range of motion and muscle strength and were followed routinely in our Outpatient Pediatric Orthopedic Clinic. After a year of follow-up, the younger girl has had difficulty in weight-bearing on the injured limb with an apparent Trendelenburg gait. Leg lengths were equal. Hip range of motion was reduced by 10–15° in abduction, internal and external rotation compared with the contralateral side. On X-ray, despite proper fracture alignment and union, we noted signs of AVN of the femoral head with sclerosis of the epiphysis and meta-epiphysial cyst (Fig. 3). She is still in an on-going follow-up with continuation of the conservative treatment considered versus a more radical surgical one. The older girl had a full physical recovery after 2 year, free of pain and without any limp or reduction of hip range of motion. X-rays have shown full union without signs of AVN (Fig. 4a , b).
In these two cases, we described an unusual injury mechanism of a water slide accident which resulted in fractures of the neck of the femur in two healthy girls. To the best of our knowledge, this specific type of injury fracture of the neck of the femur in children probably due to hyper-abduction of the legs in a water slide has not been described before in the literature. As a whole, water slide injuries have been described only scarcely. Yet, in the few studies that described orthopedic injuries, some, such as adult pelvic fractures, have been attributed to a hyper-abduction mechanism, with inter-person collision being described as a possible catalyst, as might have occurred in our cases [9,10,11,12,13,14]. As for the mechanism of injury, fractures of the femoral neck in the pediatric population have been “classically” attributed to high energy trauma, such as a fall from a height or traffic accident, with up to 30% of major non-orthopedic concomitant injuries [6,7,8], while the hyper-abduction mechanism, to the best of our knowledge, has not been described in the pediatric trauma literature and only scarcely as a cause of anterior hip dislocation in adults [15]. These relatively rare fractures, as emphasized by the case of the 10-year-old girl, may have serious consequences even with proper treatment, with AVN of the femoral head considered to be the worst [16,17,18]. Predictors of outcome have been attributed to anatomic location, described by the Delbet classification, time to surgery, anatomic reduction, type of fixation, and more [17]. When analyzing retrospectively the apparently different outcomes between the two girls, we can compare the predictors of bad outcome. With regard to time to surgery – both our patients suffered from an injury while travelling abroad and were only diagnosed on arrival at our hospital, up to 4 days later. The anatomic location of both fractures was slightly different with the younger one, with a Delbet Type II fracture, having almost one-and-a-half times the risk of AVN as compared to the older girl with a Delbet Type III [17,18]. As for the surgical technique, both fractures were fixated internally using closed reduction as proper alignment was achieved to the satisfaction of the surgeon. Closed reduction is always recommended at first, but transformation to an open technique is mandatory when anatomic reduction cannot be achieved after only a few gentle manipulations, since it has been shown both with meta-analysis and retrospective works that open reduction is superior to a closed technique in reduction of the risk for AVN [19,20]. With regard to our cases, a possible suboptimal reduction of the Delbet Type II fracture of the younger girl might have played a role in the development of the AVN. A third notable difference between the two cases is the choice of fixation hardware, which is directly related to the difference in the anatomic location of the fractures and physical characteristics of the patients. The younger and lighter of the two weighed approximately 35 kg and were fixated with a designated pediatric proximal femur plate, while the older girl was fixated rather like an adult type base of neck femoral fracture using a sliding hip plate. The exact type of internal fixation in the surgeon’s armamentarium for such fractures varies between cannulated screws, locked proximal femur implants, sliding hip screw or Kirschner wire fixation with or without spica-cast supplementation [1,21], but surgeon’s preference plays the decisive role as no actual guidelines exit in the literature [21,22]. It may be assumed that three of the described factors played a negative role in the younger patient’s outcome – long time to surgery, Delbet Type II fracture, and possibly a suboptimal reduction.
In our view, the two cases of the injured girls described in this work should emphasize the general risk of water-sliding but, more importantly, show that even a non “classical” case of high energy trauma but rather an injury caused by hyper-abduction of the hips during water-sliding can result in a pediatric neck of femur fracture. We believe that medical staff should be aware that, when a child is unable to bear weight after such an activity, femoral neck fracture should be taken into account with proper medical examination and treatment to reduce the risk of consequent complications.
Children with pain and an inability to bear weight after water sliding together with an adult companion at their backs should raise suspicion among medical staff of a femoral neck fracture. Prompt pediatric orthopedic consultation and treatment are needed in case of fracture diagnosis to reduce the risk of complications.
References
- 1.Beaty JH, Kasser JR. Rockwood and Wilkins’ Fractures in Children. Philadelphia, PA: Walter Klower, Lippincott, William and Wilkins; 2010. p. 769-96. [Google Scholar | PubMed]
- 2.Canale ST, Bourland WL. Fracture of the neck and intertrochanteric region of the femur in children. J Bone Joint Surg Am 1977;59:431-43. [Google Scholar | PubMed]
- 3.Shrader MW, Jacofsky DJ, Stans AA, Shaughnessy WJ, Haidukewych GJ. Femoral neck fractures in pediatric patients: 30 years experience at a level 1 trauma center. Clin Orthop Relat Res 2007;454:169-73. [Google Scholar | PubMed]
- 4.Delbet MP. Fractures du col de femur. Bull Mem Soc Chir Paris 1907;35:387-9. [Google Scholar | PubMed]
- 5.Colonna PC. Fractures of the neck of the femur in children. Am J Surg 1929;6:793-7. [Google Scholar | PubMed]
- 6.Bali K, Sudesh P, Patel S, Kumar V, Saini U, Dhillon MS. Pediatric femoral neck fractures: Our 10 years of experience. Clin Orthop Surg 2011;3:302-8. [Google Scholar | PubMed]
- 7.Boardman MJ, Herman MJ, Buck B, Pizzutillo PD. Hip fractures in children. J Am Acad Orthop Surg 2009;17:162-73. [Google Scholar | PubMed]
- 8.Ratliff AC. Fractures of the neck of the femur in children. J Bone Joint Surg Br 1961;44-B:528-42. [Google Scholar | PubMed]
- 9.Paulozzi LJ, McKnight B, Marks SD. A cluster of injuries at a water slide in Washington State. Am J Public Health 1986;76:284-5. [Google Scholar | PubMed]
- 10.Malpass CA Jr., Schuman SH. Waterslide injuries. Ann Emerg Med 1981;10:360-3. [Google Scholar | PubMed]
- 11.Fletcher CK, McDowell D. Water slide injuries in Jamaica. Trauma Surg Acute Care Open 2016;1:e000008. [Google Scholar | PubMed]
- 12.Ball DJ. Some observations on waterslide injuries. Inj Prev 1998;4:225-7. [Google Scholar | PubMed]
- 13.Foye PM, Abdelshahed DM, Kamrava E, Enriquez R, D’Onofrio GJ. Tailbone pain from coccyx injuries on water slides: A case series. J Emerg Med 2018;55:e33-5. [Google Scholar | PubMed]
- 14.Alboudi AM, Sarathchandran P, Geblawi SS. Delayed presentation of neck arteries dissection, caused by water slide activity. BMJ Case Rep 2018;11:e226333. [Google Scholar | PubMed]
- 15.Epstein HC, Harvey JP. Traumatic anterior dislocations of the hip: Management and results, an analysis of fifty five cases. J Bone Joint Surg Am 1972;54:1561-2. [Google Scholar | PubMed]
- 16.Dial BL, Lark RK. Pediatric proximal femur fractures. J Orthop 2018;15:529-35. [Google Scholar | PubMed]
- 17.Moon ES, Mehlman CT. Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and meta-analysis of 360 cases. J Orthop Trauma 2006;20:323-9. [Google Scholar | PubMed]
- 18.Wang WT, Li YQ. Risk factors for the development of avascular necrosis after femoral neck fractures in children: A review of 239 cases. Bone Joint J 2019;101-B:1160-7. [Google Scholar | PubMed]
- 19.Song KS. Displaced fracture of the femoral neck in children: Open versus closed reduction. Bone Joint J Br 2010;92:1148-51. [Google Scholar | PubMed]
- 20.Wang W, Wei J, Xu Z. Open reduction and closed reduction internal fixation in treatment of femoral neck fractures: A meta-analysis. BMC Musculoskelet Disord 2014;15:167. [Google Scholar | PubMed]
- 21.Herring J. Tachdjian’s Pediatric Orthopaedics: From the Texas Scottish Rite Hospital for Children. 5th ed. Philadelphia, PA: Saunders; 2013. p. 1388-92. [Google Scholar | PubMed]
- 22.Barreto Rocha DF, Horwitz DS, Sintenie JB. Femoral neck fractures in children: Issues, challenges, and solutions. J Orthop Trauma 2019;33 Suppl 8:S27-32. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making
June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study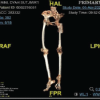 June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review
June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review