
Complex combination of fractures in young patients having comorbidities must be appropriately managed by multi-specialty teams in the shortest possible time frame for optimal functional outcomes.
Dr. M K Rajak,
Department of Orthopaedics,
Tata Main Hospital, Jamshedpur, Jharkhand, India.
E-mail: manojrajak@tatasteel.com
Abstract
Introduction: Simultaneous fractures in the neck of femur on the one side and contralateral intertrochanteric fracture of the femur with only trivial injury are among rarest injuries. Fracture neck of femur or intertrochanteric fracture either isolated or in combination such as simultaneous bilateral fracture neck of femur and simultaneous bilateral intertrochanteric fractures are relatively commonly reported in literature. Herein, we report a very rare case of a young female with chronic kidney disease who presented with simultaneous fractures neck of femur on the one side and contralateral intertrochanteric fracture of femur after a fall from standing height.
Case Report: A 41-year-old female with chronic kidney disease from the past 5 years presented to us with severe pain at both hip and inability to stand after a fall from standing height. Clinical examination and investigations were done. She suffered fracture neck of femur on the right side and intertrochanteric fracture femur on the left side. Single stage fixation of both these fractures by two different methods was done successfully after optimization of her medical condition with multidisciplinary approach. She was advised weight bearing according to fixation method used and progress of fracture union. She regained her preoperative walking status gradually in 6 months.
Conclusion: Simultaneous fractures in the neck of femur on the one side and intertrochanteric fracture of the femur on the other side are very rare presentation and can happen in patients with primary or secondary bone disease. Multidisciplinary team effort is needed for overall effective management and prompt surgical treatment can help achieve favorable outcome.
Keywords: Simultaneous, fracture neck of femur, intertrochanteric fracture femur.
The complex anatomy and enough loading force borne by proximal femur make it vulnerable to fractures. Isolated fracture neck of femur or intertrochanteric fractures are commonly seen. These generally occur in elderly following simple fall and in young after high energy trauma [1]. In literature, we find that simultaneous bilateral fracture neck of femur and simultaneous bilateral intertrochanteric fractures are rare and generally occur after major trauma, epilepsy or primary, and secondary bone disease and they are reported as a case report or case series sporadically [2,3,4,5,6,7,8]. We report a very rare case of fracture neck of femur on the one side and contralateral intertrochanteric fracture femur occurring simultaneously in a 41-years-old female with history of hypertension and chronic renal failure and discuss the challenges in orthopedic management of this patient and outcome. Unfortunately, we did not find any such report in literature.
This patient reported in emergency in our hospital with history of fall from standing height. At the time of admission, she was conscious, oriented, and hemodynamically stable. From the time of fall she was not able to get up and complained of pain at both hips. She was not able to move either lower limb due to unbearable pain which was more on attempt of moving the limbs. The right lower limb was apparently shorter than the left and left lower limb was relatively more externally rotated. She also had injury at the back of right shoulder and the shoulder movement was painfully restricted. There was no neurological deficit.
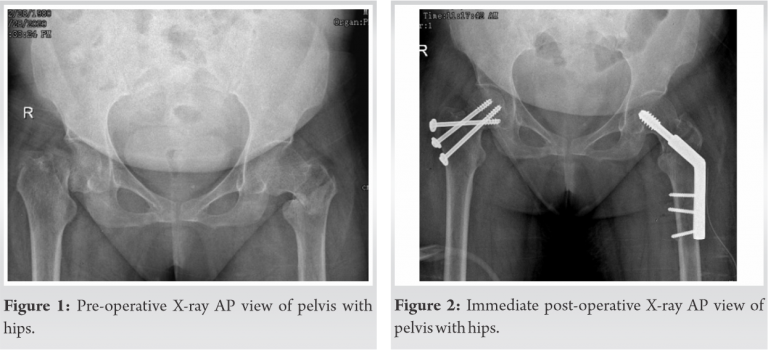
Her medical history revealed chronic kidney disease Stage IV and hypertension for which she was taking medication. Patient was examined for any other injury which may get masked because of these severe painful conditions. Radiological investigation revealed fracture neck of femur on right and intertrochanteric fracture on the left side (Fig. 1) and undisplaced fracture of lateral border of right scapula. Both lower limbs were immobilized with bilateral skin traction and for scapula fracture universal shoulder immobilizer was used. On investigation, she was found to be anemic with hemoglobin 5.7 gm/dl, her serum creatinine level was 4.83 mg/dl, and serum potassium was 2.8 meq/l. General physician, nephrologist, and anaesthesiologist were involved to optimize the medical condition of the patient as she needed major surgery. She was an active lady and our goal was to bring her to pre-injury level as early as possible. Dynamic hip screw fixation has stood the test of time for fixation of stable intertrochanteric fracture. In elderly patient, a prosthetic replacement is adequate for fracture neck of femur but at the age of 41 years it was reasonable to plan preserving the femoral head. The presence of this combination of injury in a comorbid patient and trying to preserve the femoral head presented an additional challenge in attempted osteosynthesis.
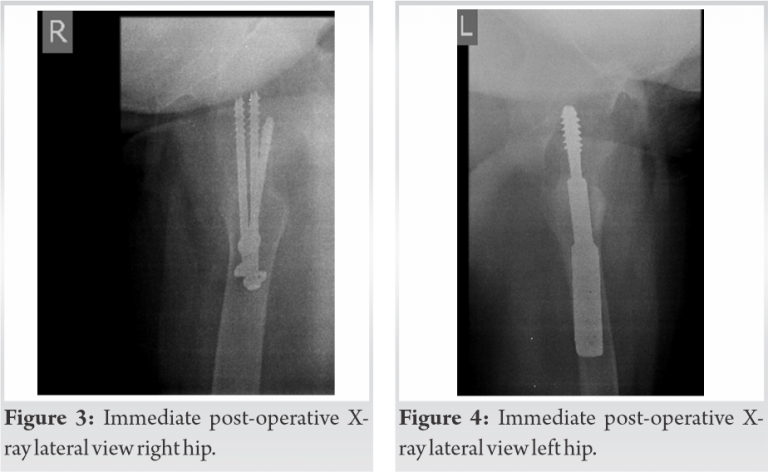
We planned dynamic hip screw for the intertrochanteric fracture and multiple cannulated cancellous screws to stabilize fracture neck of femur in the same sitting. The patient and relatives were prognosticated about the per-operative, post-operative, early, and late complications. In the operation theater with the patient on traction table, we first stabilized the intertrochanteric fracture with dynamic hip screw on the left side. After attempting closed reduction of the displaced femoral neck fracture on the right side, under image intensification, and having achieved it, it was fixed with three 6.5 mm cannulated cancellous screws, one of them as derotation screw. The per-operative period was uneventful. For next 48 h, she was kept in high dependency unit for monitoring after which she was shifted to the general orthopedic ward. Check X-ray taken on 2nd post-operative day was acceptable (Fig. 2, 3, 4). The same day 1st change of dressing was done. In bed physiotherapy was started with leg hanging and quadriceps exercise. Right shoulder remained immobilized. Patient was discharged with advice to attend OPD for stitch removal on 14th post-operative day. At stitch removal, her surgical wounds were found to be healthy. Patient was advised to carry on physiotherapy and non-weight bearing and was asked to follow-up after 1 month.
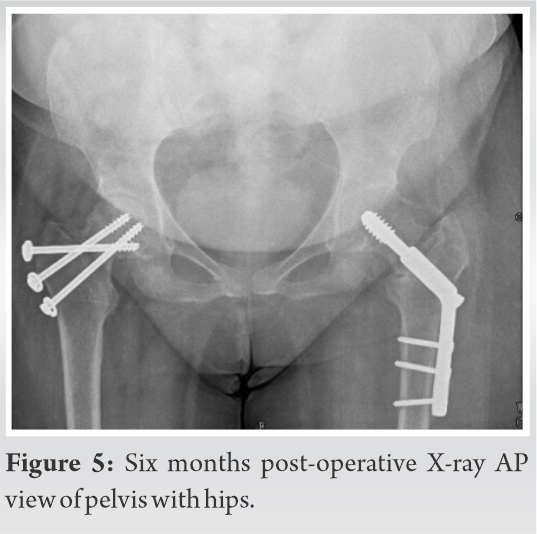
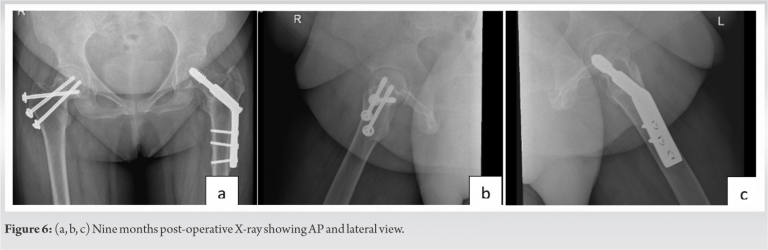
As lockdown was enforced from March 23, 2020, in COVID-19 pandemic, restricting mobility and because of fear of contracting COVID, she did not attend OPD. Telephonic conversation was done to know her condition and it was found satisfactory. Patient physically reported at the end of 3rd month. X-ray of pelvis with both hips was taken which showed well-advanced stage of union. We wanted her to start weight bearing on the left lower limb (and no weight bearing on right lower limb) but she was apprehensive to use crutches because of post-injury discomfort in right shoulder. She started this in 4th month as per telephonic conversation. After 6 months from the surgery, she was readmitted in our hospital under the nephrology unit with reduced hemoglobin. She was treated and two units of packed cell were transfused. Her X-ray showed fractures well united (Fig. 5) and she could walk without support. She was asked to follow-up at 3 months interval. At last follow-up of 9 months her X-ray showed well united fracture in both AP and lateral view (Fig. 6a, b, c) and she had good range of movement in both hips.
Simultaneous fracture neck of femur on the one side and intertrochanteric fracture on the other side is one of the rarest patterns of injury. We did not find any report about such injury in English scientific literature. In bilateral cases, generally the mode of injury is high velocity trauma in young or trivial fall with secondary bone disease. Our patient had a history of chronic kidney disease Stage IV and she fell from standing height. Managing this case was very challenging as she had simultaneous bilateral proximal femur fracture and more so one of them was fracture neck of femur. At the patient’s age of 41 our goal was to preserve the head and fix the fracture. She was managed by a multidisciplinary team comprising of orthopedic surgeon, general physician, nephrologist, anaesthesiologist, physician, and physiotherapist. We planned for single stage fixation to start mobilizing the patient as early as possible. The intertrochanteric fracture was fixed first with dynamic hip screw. Fracture neck of femur was fixed with three cannulated screw after satisfactory closed reduction. One of the three screws used was short reach 16 mm derotation screw which also helped in achieving additional compression at femoral neck fracture site. Two major complications associated with fracture neck of femur following osteosynthesis is nonunion and avascular necrosis of femoral head, which is estimated at 10–30% and 15–30%, respectively, if treated within 24 h [9,10]. As our case had multiple comorbidities, fixation was done after 1 week, after obtaining fitness for surgery, thereby increasing the chances of the complications. Fixation of femoral neck fracture using three cannulated screws is preferred method as it affords adequate stabilization [11]. In our case, the preferred method was used. Due to COVID, we could not follow up the patient at regular intervals, but she was always under our consultation over telephone. At 9 months follow-up she could walk independently with good functional outcome, and her X-rays showed well united fracture and there was no evidence of avascular necrosis.
Simultaneous fracture neck of femur on the one side and intertrochanteric fracture of the opposite side is one of the rarest injuries. We are not sure about any such report in the literature. To the best of our knowledge, this may be the first case being reported. Associated diseases need aggressive management by a multidisciplinary approach to optimize the medical condition and prevent morbidity associated with long immobilization in bed. Single stage fixation with physiotherapy leads to good functional outcome.
We believe that this manuscript is appropriate for publication by Journal of Orthopedic Case Reports because of its rarity and need of proper management involving multidisciplinary team to take care of comorbidity and complex combination of fracture requiring quick and appropriate surgical treatment to prevent complications from being bed ridden for long and selection of method of treatment for fracture neck of femur in a relatively young patient.
References
- 1.Grisoni N, Foulk D, Sprott D, Laughlin RT. Simultaneous bilateral hip fractures in a level I trauma center. J Trauma 2008;65:132-5. [Google Scholar | PubMed]
- 2.Faraj AA. Bilateral simultaneous combined intra- and extracapsular femoral neck fracture secondary to nutritional osteomalacia: A case report. Acta Orthop Belg 2003;69:201-3. [Google Scholar | PubMed]
- 3.Rejev A. Bilateral spontaneous inter-trochanteric fractures of proximal femurs. Int J Surg Case Rep 2012;5:246-8. [Google Scholar | PubMed]
- 4.Copuroğlu C, Ozcan M, Dülger H, Yalnız E. Late-diagnosed bilateral intertrochanteric femur fracture during an epileptic seizure. Ulus Travma Acil Cerrahi Derg 2012;18:92-94. [Google Scholar | PubMed]
- 5.Karapinar H, Ozdemir M, Akyol S, Ulkü O. Spontaneous bilateral femoral neck fractures in an adult with chronic renal failure. Acta Orthop Belg, 2003;69:82-5. [Google Scholar | PubMed]
- 6.Nagao S, Ito K, Nakamura I. Spontaneous bilateral femoral neck fractures associated with a low serum level of Vitamin D in a young adult. J Arthroplasty 2009;24:e1-4. [Google Scholar | PubMed]
- 7.Grimaldi M, Vouaillat H, Tonetti J, Merloz P. Simultaneous bilateral femoral neck fractures secondary to epileptic seizures: Treatment by bilateral total hip arthroplasty. Orthop Traumatol Surg Res 2009;95:555-7. [Google Scholar | PubMed]
- 8.Akçali O, Koşay C, Günal I, Alici E. Bilateral trochanteric fractures of the femur in a patient with chronic renal failure. Int Orthop 2000;24:179-80. [Google Scholar | PubMed]
- 9.Swiontkowski MF. Intracapsular fractures of the hip. J Bone Joint Surg Am 1994;76:129-38. [Google Scholar | PubMed]
- 10.Vertelis A, Petrulis A, Jermolajevas V. Treatment results of displaced femoral neck fractures. Methods 2002;38:505-9. [Google Scholar | PubMed]
- 11.Forsh DA, Ferguson TA. Contemporary management of femoral neck fractures: The young and the old. Curr Rev Musculoskelet Med 2012;5:214-21. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 A Novel Approach to Proximal Humerus Giant Cell Tumor: Cement Spacer and Screw Interdigitation for Optimal Stability
April 1, 2026 A Novel Approach to Proximal Humerus Giant Cell Tumor: Cement Spacer and Screw Interdigitation for Optimal Stability November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report
November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report June 1, 2026 Nonvascularized Iliac Crest Autograft for Wrist and Hand Reconstructions: A Report of Two Clinical Cases and Literature Review
June 1, 2026 Nonvascularized Iliac Crest Autograft for Wrist and Hand Reconstructions: A Report of Two Clinical Cases and Literature Review September 24, 2017 Head-on Allograft Transplantation: A Unique Case Report Where a Large Piece of Femoral Bone was Extruded from One Patient’s Body and Impaled Another Patient’s Tibia
September 24, 2017 Head-on Allograft Transplantation: A Unique Case Report Where a Large Piece of Femoral Bone was Extruded from One Patient’s Body and Impaled Another Patient’s Tibia