
This clinical case demonstrates the utility of multiple modified Sofield-Millar osteotomies with intramedullary nailing in allowing for acute correction of leg length discrepancy and severe malalignment in an adult patient. Correction of deformity can allow for improvement in pain and ambulatory function as described in this case report.
Dr. Keneth W. Graf, Department of Orthopaedics, Cooper University Hospital, Camden, New Jersey, United States. E-mail: saa322@drexel.edu
Abstract
Introduction: Approximately 70% of the population have a leg length discrepancy, with 2 cm being the threshold for surgical treatment. Although there are reports of patient outcomes after incremental leg-lengthening, there is a paucity of data regarding acute lengthening procedures. We present a unique case of acute leg lengthening and correction of severe malalignment in an adult patient after femoral malunion treated with multiple modified Sofield-Millar osteotomies and intramedullary nailing, a technique that has only previously been performed in pediatric long bone deformities. To the author’s knowledge, there have been no previous reports of acute lengthening in an adult patient to correct for such a severe deformity in a single operation.
Case Report: A 48-year-old woman with a 35-year history of a right femur fracture malunion presented with a 5 cm leg length discrepancy and severe malalignment associated with pain and ambulatory dysfunction. Multiple modified Sofield-Millar osteotomies followed by placement of an intramedullary nail were performed and resulted in successful acute correction of limb length discrepancy and anatomical alignment. There was a complete union of bone with callus formation at osteotomy sites at 9 months postoperatively, and the patient reported minimal pain and improved ambulation. The patient was followed for 2 years postoperatively and experienced an improvement in ambulatory function with no pain. No post-operative complications were observed.
Conclusion: Multiple modified Sofield-Millar osteotomies with intramedullary nailing were utilized for successful acute correction of limb length discrepancy and severe malalignment with improvement in pain and ambulatory function in this case of femoral leg length discrepancy in an adult patient.
Keywords: Leg length discrepancy, malalignment, acute correction.
Approximately 70% of the population have a leg length discrepancy, with 5% possessing a discrepancy of more than 1.5 cm [1,2]. Trauma of the lower extremity and congenital abnormalities is two common reasons for leg length discrepancies [1,3]. Conservative measures, such as insoles, prosthesis, and orthosis, can be used to manage discrepancies under 2 cm [2,4]. Deformities with over 2 cm in discrepancy can cause gait dysfunction and are an indication for surgical correction with either acute or incremental lengthening [2,3]. Although incremental leg lengthening procedures have been studied, especially in the pediatric literature, there is little information regarding outcomes after acute lengthening. A few case reports have described the use of Sofield-Millar osteotomies to treat long bone deformities in pediatric patients with osteogenesis imperfecta (OI) [5,6,7]. However, there is no information available about outcomes of this technique in an adult patient with a leg length discrepancy and severe malalignment. The purpose of this case report is to present a unique case of acute femoral lengthening and realignment in an adult patient after femoral malunion treated with multiple modified Sofield-Millar osteotomies and intramedullary nailing, a technique that has only previously been performed in pediatric long bone deformities. The goal of this procedure was to surgically correct the limb length discrepancy and severe malalignment with a single operation.
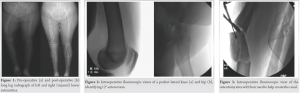
A 48-year-old female with a 35-year history of a right femur fracture malunion presented to the outpatient setting with a 5 cm leg length discrepancy and severe malalignment. Orthopedic history is significant for conservative treatment of a right femur and tibial shaft fracture. In the years before presentation, the patient reported pain and difficulty ambulating due to her limb deformity. She was evaluated by an orthopedic surgeon outside of our hospital system for right knee pain and was recommended to undergo total knee arthroplasty (TKA) for severe joint arthrosis. Pre-operative radiographic evaluation of the right lower extremity demonstrated a 5 cm leg length discrepancy, 45° procurvatum, 42° varus, and 35° internal rotation deformity compared to the contralateral, non-injured side (Fig. 1a). Due to the severity of the malalignment and leg length discrepancy, the patient required a limb lengthening and realignment procedure before planned TKA.
Radiographs and computed tomography scanogram of the right femur and tibia were performed for initial evaluation, which depicted malunion deformity of the right femur. Moderate deformity of the right tibial shaft as well as healed proximal lateral tibia and proximal fibula fractures were noted. Prominent degenerative changes were present in all compartments. Due to the patient’s complaints of pain and ambulatory dysfunction, imaging results, and desire for TKA, the decision was made to treat the patient’s deformity with modified Sofield-Millar osteotomies and intramedullary nailing to acutely correct the leg length discrepancy and malalignment with a single operation.
Once the patient consented for the procedure, fluoroscopy was used to check a perfect lateral of the non-injured contralateral knee and hip, which established a baseline of 12° of anteversion (Fig. 2a, 2b). Afterward, she was positioned in the lateral decubitus position on a radiolucent table in the operating room. A drill bit and osteotome were used to perform the three osteotomies (Fig. 3). The first osteotomy was made between the malunion site and the distal femur, while the second osteotomy was done between the malunion site and proximal femur. The third osteotomy was performed in the middle of the malunion. Afterward, anterior-posterior and lateral views of the hip were obtained to identify the medial tip of the greater trochanter proximally (Fig. 4a, 4b). Radiographic imaging was used to guide a high-speed burr followed by a 4.5 mm drill bit through osteotomized pieces to create a canal in the bone. Then, an opening reamer for the tibial nail was used to enlarge the canal to allow for insertion of the ball tip guide wire (Fig. 5a, 5b). We reamed from 8 to 13 mm for placement of the 11 mm reconstruction nail. Once the nail was placed, the osteotomy sites were compressed in anatomical alignment.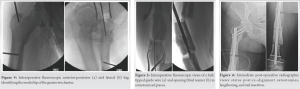
Perfect lateral knee and hip radiographs were obtained to confirm 12° of anteversion consistent with the contralateral side. Screws were then placed in a center-center position in the head (Fig. 6a). Osteotomy sites were compressed. A drill bit and osteotome were used to make a small osteotomy, because the intercalary segment was being translated by the distal metaphysis. Once the joint was in anatomical position, two distal interlocking screws were inserted, and the osteotomy sites were packed with biologic bone graft for healing (Fig. 6b). Postoperatively, the patient was weight-bearing as tolerated and discharged on post-operative day 3 once physical therapy determined that the patient was stable. Radiographic imaging at 1, 3, and 4 months postoperatively demonstrated anatomical alignment of the femur with increased bone healing and callus formation at the osteotomy sites. The distal femur was the slowest to initiate callus formation. By 6 months postoperatively, the patient had clinically equal limb lengths and had returned to the pre-operative level of function, using a cane for ambulation. Radiographs at 9 months postoperatively depicted complete bone union with callus formation, and the femur measured 1.2 cm shorter on the operative side (Fig. 7a, 7b). The osteotomies fully healed by 1 year postoperatively. Radiographs of the femur demonstrated anatomical alignment (Fig. 8a, 8b). At that time, the patient also reported minimal pain and decided to no longer undergo TKA. The patient was followed for 2 years postoperatively and continued to have a satisfactory range of motion with minimal pain. Radiographs continued to demonstrated knee arthrosis, but the joint was anatomically aligned, and the osteotomy had healed (Fig. 1b). No post-operative complications associated with infection, pain, failure of hardware, or re-fracture were observed during the follow-up.

Leg length discrepancy is a common problem affecting 70% of the population, usually caused by trauma or congenital anomalies [1,2,3]. Our current case describes the successful outcome of an adult patient who underwent multiple modified Sofield-Millar osteotomies and intramedullary nailing for acute femoral lengthening and full acute correction of severe malalignment after malunion with a single operation. Although incremental leg lengthening procedures have been studied in the orthopedic literature, there is little information regarding outcomes after acute lengthening. Multiple modified Sofield-Millar osteotomies and intramedullary nailing are a technique used to treat long bone deformities in pediatric patients with OI, with a few pediatric case reports documenting outcomes in patients who underwent this procedure [5,6,7]. To et al. documented improved ambulatory status within the 1st post-operative year in a pediatric OI patient, which corroborates the results of our case [7]. Abulsaad and Abdelrahman also reported improved ambulatory status and rapid bone union in their series of OI patients who underwent the procedure [5]. However, they also observed the necessity for surgical revision after 2 years in their study cohort due to bone growth observed in the pediatric population [5]. Since our patient is an adult with closed epiphyseal plates, it was unlikely that she would need to undergo surgical revision. During the 2 years of follow-up, no complications were observed, and the patient did not require surgical revision. In our current case, the patient initially presented to an orthopedic surgeon for knee pain and was recommended to undergo TKA for severe right knee arthrosis. However, due to the patient’s leg length discrepancy and severe malalignment, she was instructed to first undergo limb lengthening and alignment correction. The previous studies have associated leg length discrepancy with hip, knee, and lower back degenerative joint disease [1,8,9]. Two separate studies performed by Harvey and Noll identified limb length discrepancy as a risk factor for osteoarthritis in the shortened limb [1,2,9]. These findings are consistent with the presentation of this case. After the patient underwent treatment with multiple modified Sofield-Millar osteotomies and intramedullary nailing, she reported an improvement in pain and ambulatory status. Although severe joint arthrosis continued to be present on radiographic imaging, the patient elected to no longer undergo TKA due to her lack of pain and improved quality of life. The patient was also able to resume employment due to her significant clinical improvement.
Multiple modified Sofield-Millar osteotomies with intramedullary nailing were utilized for successful acute correction of leg length discrepancy and severe malalignment with improvement in pain and ambulatory function in our current case report. Due to the patient’s significant clinical improvement, she no longer needed to undergo further surgery for TKA. To the best of our knowledge, there have been no previous reports of acute lengthening in an adult patient to correct such a severe deformity in a single operation.
This clinical case demonstrates the utility of multiple modified Sofield-Millar osteotomies with intramedullary nailing in allowing for acute correction of leg length discrepancy and severe malalignment in an adult patient. Correction of deformity can allow for improvement in pain and ambulatory function as we see in our patient.
References
- 1.Harvey WF, Yang M, Cooke TD, Segal NA, Lane N, Lewis CE, et al. Association of leg-length inequality with knee osteoarthritis: A cohort study. Ann Intern Med 2010;152:287-95. [Google Scholar | PubMed]
- 2.Hasler CC, Krieg AH. Current concepts of leg lengthening. J Child Orthop 2012;6:89-104. [Google Scholar | PubMed]
- 3.Gurney B. Leg length discrepancy. Gait Posture 2002;15:195-206. [Google Scholar | PubMed]
- 4.Campbell TM, Ghaedi BB, Ghogomu TE, Welch V. Shoe lifts for leg length discrepancy in adults with common painful musculoskeletal conditions: A systematic review of the literature. Arch Phys Med Rehabil 2018;99:981-93.e2. [Google Scholar | PubMed]
- 5.Abulsaad M, Abdelrahman A. Modified sofield-millar operation: Less invasive surgery of lower limbs in osteogenesis imperfecta. Int Orthop 2009;33:527-32. [Google Scholar | PubMed]
- 6.Li YH, Chow W, Leong JC. The sofield-millar operation in osteogenesis imperfecta. A modified technique. J Bone Joint Surg Br 2000;82:11-6. [Google Scholar | PubMed]
- 7.To M, Gupta V, Chow W. Surgical management of long bone pseudarthrosis with severe limb length discrepancy in osteogenesis imperfecta. J Pediatr Orthop B 2013;22:63-9. [Google Scholar | PubMed]
- 8.Murray KJ, Molyneux T, Grande MR, Mendez AC, Fuss FK, Azari MF. Association of mild leg length discrepancy and degenerative changes in the hip joint and lumbar spine. J Manipulative Physiol Ther 2017;40:320-9. [Google Scholar | PubMed]
- 9.Noll DR. Leg length discrepancy and osteoarthritic knee pain in the elderly: An observational study. J Am Osteopath Assoc 2013;113:670-8. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Concomitant Neck of Femur and Greater Trochanter Fracture in a Young Adult – A Case Report
October 1, 2025 Concomitant Neck of Femur and Greater Trochanter Fracture in a Young Adult – A Case Report February 10, 2021 Delayed Slipped Capital Femoral Epiphysis Following Septic Arthritis of a Hip: A Case Report
February 10, 2021 Delayed Slipped Capital Femoral Epiphysis Following Septic Arthritis of a Hip: A Case Report December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point
December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point January 19, 2013 Use of Fibula Bridge Graft Technique to Treat a Distal Tibia Non Union- A Case Report
January 19, 2013 Use of Fibula Bridge Graft Technique to Treat a Distal Tibia Non Union- A Case Report