
Clinician should always look for a cartilage cap while evaluating osteochondroma.
Dr. Deepak A Tambe, Department of Orthopaedics, Dr. BVP Rural Medical College, Pravara Medical Trust, Pravara Institute of Medical Sciences, Ahmednagar - 413 736, Maharashtra, India. E-mail: deepaktambe06@gmail.com
Abstract
Introduction: Fibrous dysplasia is a benign disorder of unknown etiology. It represents a disturbance of normal bone development – a defect in osteoblastic differentiation and maturation that originates in the mesenchymal precursor of the bone. It is characterized by slow progressive replacement of bone by abnormal isomorphic fibrous tissue. Temporal bone involvement is extremely rare. We report an unusual case of fibrous dysplasia presented like a solitary osteochondroma.
Case Report: A 14-year-old girl presented with the complaints of slow-growing swelling on the left temporal region in scalp near left eye for 2 years. The swelling was small to begin with, which increased gradually over a period of 2 years. There were no other presenting symptoms. Hearing was normal. Parents of the patient were concerned with cosmesis only. She had undergone 3D CT scan of skull where it showed bony outgrowth with features suggestive of exostosis. This bony outgrowth had cortex in continuity to cortex of temporal bone and medullary canal same as that of the temporal bone and ground-glass appearance. Repeat CT scan showed bony outgrowth with cortical continuity and had pedicle. It was suggestive of pedunculated osteochondroma. There was no evidence of malignant transformation as swelling showed calcified osteoid-like mass throughout. Hence, the clinical and radiological diagnosis of the left temporal bone solitary osteochondroma was made. However, histopathology showed irregularly shaped bony trabeculae in fibrous stroma of variable cellularity without accompanying osteoblast rimming. Thus, diagnosis was fibrous dysplasia of bone. Histopathological slide was reviewed by two independent pathologists with same conclusion.
Conclusion: Our case was unique in that the lesion presented clinically and radiologically as solitary osteochondroma. However, in hindsight, lack of cartilage cap on CT scan should have prompted us to look for another diagnosis. To the best of our knowledge, this was unique varied presentation of fibrous dysplasia of temporal bone.
Keywords: Fibrous dysplasia, osteochondroma, temporal bone.
Fibrous dysplasia is a developmental disorder caused by abnormal proliferation and maturation of fibroblast. These fibroblasts replace mature bone which results in structurally weak, immature woven bone. The craniofacial fibrous dysplasia represents around 3% of all bone tumors and 7% of benign tumors [1] However, fibrous dysplasia limited to temporal bone is very rare [2].
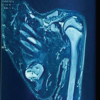
A 14-year-old school girl brought by her grandfather in June 2021 to the outpatient department with the complaints of slow-growing swelling on the left temporal region in scalp near left eye for 2 years. The swelling was small to begin with, which increased gradually over a period of 2 years to present size of 2*2 cm round-shaped swelling. Examination shows that the swelling was in the temporal fossa, above the zygomatic arch, smooth, not attached to overlying skin, becomes slightly less prominent on clenching of teeth, non-pulsatile, no transillumination, hard with no dilated veins over it and arising from bone. There were no other presenting symptoms. Hearing was normal. Parents of the patient were concerned with cosmesis only. She had been shown to an orthopedic surgeon 1 year back in July 2020 for the same complaint of swelling near left eye and had undergone 3D CT scan of skull where it showed bony outgrowth from the left temporal bone with features suggestive of exostosis. This bony outgrowth had cortex in continuity to cortex of temporal bone and medullary canal same as that of the temporal bone and ground-glass appearance (Figs. 1a, b, c).
Now, the patient was advised repeat CT scan with 3D reconstruction to look for increase in size and condition of underlying bone. Repeat CT scan showed (Fig. 1b) bony outgrowth of 35*28*22 mm arising from the left temporal bone with same cortical continuity and had pedicle. It was suggestive of pedunculated osteochondroma. There was no evidence of malignant transformation as swelling showed calcified osteoid-like mass throughout. Hence, the clinical and radiological diagnosis of the left temporal bone solitary osteochondroma was made. However, it is surprising to see absence of cartilage cap over the bony mass in both CT scans. As complaints were purely cosmesis, and relatives insisted surgical excision, surgery (extraperiosteal resection of solitary osteochondroma) was planned.
After explaining the procedure, the patient was taken for surgery for excisional biopsy. Hairs were removed from surgical site (Fig. 2a). After GA, the patient was given lateral decubitus position. A curvilinear incision was taken over swelling. Temporal fascia and temporalis muscle were incised in a “T” shape using a bipolar cautery. Bony mass reached; peduncle identified. Extraperiosteal excision of tumor with some amount of normal surrounding bone and periosteum was done using sharp 10 mm osteotome. Tumor was hard to cut. Bed of the tumor was bleeding and cauterized thoroughly. Bone wax was applied. Wound was closed in layers, no drain required (Fig. 2c). Excised part was smooth rounded (Fig. 2b) with a peduncle at one end and was bony hard on palpation with appearance suggestive of osteochondroma. Postoperatively, on check dress on day 2, there was no discharge or bleeding. The patient was given IV antibiotics. The patient was discharged on oral antibiotics and analgesics on day 3. However, histopathology showed irregularly shaped bony trabeculae in fibrous stroma of variable cellularity without accompanying osteoblast rimming (Fig. 3a, b, c). Thus, diagnosis is fibrous dysplasia of bone.  Histopathological slide was reviewed by two independent pathologists with same conclusion. On the last follow-up (11-month post-operative), the patient was stable with no complaint. There was no visible swelling and scar was hidden behind hairline (Figs. 4a, b). There was no hearing loss.
Histopathological slide was reviewed by two independent pathologists with same conclusion. On the last follow-up (11-month post-operative), the patient was stable with no complaint. There was no visible swelling and scar was hidden behind hairline (Figs. 4a, b). There was no hearing loss.
Fibrous dysplasia is characterized by slow, progressive replacement of bone by an abnormal proliferative isomorphic fibrous tissue. It is intermixed with poorly formed, irregularly arranged trabeculae. In 1937, McCune and Bruch [3] suggested it to be a distinct entity among abnormalities of bone formation. Lichtenstein introduced the term fibrous dysplasia. It reportedly constitutes 2.5% of all osseous and 7% of all benign osseous tumors. Male:female ratio is 2:1. It is more common amongst Caucasians (80%). Cases among African-American (2%) and Asians (1%) are extremely rare(1). Precise etiology is unknown. Lichtenstein and Jaffe [4] suggested abnormal differentiation of mesenchyme. Reed [5] suggested that there is an arrest of growth at an immature woven stage and a disturbance of post-natal cancellous bone maintenance. Albin et al. suggested that it may be associated with increased levels of steroid hormone receptors (estrogen and progesterone) [6]. Fibrous dysplasia has three subtypes: Monostotic, polyostotic, and McCune-Albright syndrome. The most common are monostotic and it commonly involves femur and ribs (70%). Their growth is very slow and it usually stops growing after puberty. Polyostotic disease usually becomes evident late in childhood and leads to more severe skeletal and craniofacial abnormalities [6]. Polyostotic disease usually affects the sphenoid, frontal, maxillary, and ethmoid bones. Occipital and temporal bone involvement is very rare [7]. McCune-Albright syndrome is more common in female which is associated with short stature. Hyperthyroidism is most common among many associated endocrine abnormalities. Our patient had no clinical features suggestive of endocrine anomaly. Progressive conductive hearing loss due to occlusion of the Eustachian tube or external auditory canal is the most common symptom of fibrous dysplasia of temporal bone [8]. Progressive hearing loss and post-auricular mass are usual presentation. Sensory-neural hearing loss occurs in 14–17% of the patients. Cholesteatoma occurs in about 40% of the cases and facial nerve involvement reported in 10% [8]. Other unusual symptoms include tinnitus, dizziness, pain, and trismus [1,7]. These symptoms were not present in our patient. Three classical radiologic findings are described as: Pagetoid, sclerotic, and myxoid [9]. The pagetoid or ground-glass pattern is commonest. The sclerotic pattern shows uniform density. The cystic pattern is characterized by ovoid or spherical lucidity surrounded by a dense bony shell [2]. Distinguishing features of fibrous dysplasia on CT scan include ground-glass appearance, involvement of the paranasal sinuses, thickened cranial cortices, nasal cavity involvement, the presence of a soft-tissue mass, maxillary involvement, and the presence of cystic changes [10]. This typical appearance was absent in our patient. There is no specific medical treatment for fibrous dysplasia. Asymptomatic lesions can be monitored regularly without any intervention. Indication for surgery includes bony encroachment of external auditory canal, recurrent infection, and secondary canal cholesteatoma. Surgery of the dysplastic temporal bone can be hazardous as landmarks are not clear and intraoperative bleeding can be vigorous. Radiation therapy is strictly avoided as it has high chances of malignant transformation.
Our case was unique in that the lesion presented clinically and radiologically as solitary osteochondroma. However, in hindsight, lack of cartilage cap on CT scan should have prompted us to look for another diagnosis. To the best of our knowledge, this was unique varied presentation of fibrous dysplasia of temporal bone.
Fibrous dysplasia of bone can present as a solitary round hard bony outgrowth and can have medullary canal same as that of the bone of origin. However, one should always look at a cartilage cap over it, as absence of cartilage cap suggests that it could be fibrous dysplasia
References
- 1.Nager GT, Kennedy DW, Kopstein E. Fibrous dysplasia: A review of the disease and its manifestations in the tem-poral bone. Ann Otol Rhinol Laryngol Suppl 1982;92:1-52. [Google Scholar | PubMed]
- 2.Brown EW, Megerian CA, McKenna MJ, Weber A. Fibrous dysplasia of the temporal bone: Imaging findings. AJR Am J Roentgenol 1995;164:679-82. [Google Scholar | PubMed]
- 3.McCune D, Bruch H. Osteodystrophia fibrosa: Report of a case in which the condition was combined with precocious puberty, multiple pigmentation of the skin and hyperthyr-oidism. Am J Dis Child 1937;52:745-8. [Google Scholar | PubMed]
- 4.Lichtenstein L, Jaffe H. Fibrous dysplasia of bone. Arch Pathol 1942;33:777-816. [Google Scholar | PubMed]
- 5.Reed RJ. Fibrous dysplasia of bone. A review of 25 cases. Arch Pathol 1963;75:480-95. [Google Scholar | PubMed]
- 6.Albin J, Wu R. Abnormal hypothalamic-pituitary function in polyostotic fibrous dysplasia. Clin Endocrinol (OXf) 1981;14:435-43. [Google Scholar | PubMed]
- 7.Lambert PR, Brackmann DE. Fibrous dysplasia of the temporal bone: The use of computerized tomography. Otolaryngol Head Neck Surg 1984;92:461-7. [Google Scholar | PubMed]
- 8.Megerian CA, Sofferman RA, McKenna MJ, Eavey RD, Nadol JB Jr. Fibrous dysplasia of the temporal bone: Ten new cases demonstrating the spectrum of otologic sequelae. Am J Otol 1995;16:408-19. [Google Scholar | PubMed]
- 9.Nager GT, Holliday MJ. Fibrous dysplasia of the temporal bone. Update with case reports. Ann Otol Rhinol Laryngol 1984;93:630-3. [Google Scholar | PubMed]
- 10.Tehranzadeh J, Fung Y, Donohue M, Anavim A, Pribram HW. Computed tomography of Paget disease of the skull versus fibrous dysplasia. Skeletal Radiol 1998;27:664-72. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report
August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report