
Intraspinal extradural arthrosynovial cervical cysts could be treated by an undirect approach with anterior cervical discectomy and fusion.
Dr. Mathieu Lozouet, Department of Neurosurgery, Rouen University Hospital, 1 rue de Germont, 76000 Rouen, France. E-mail: mathieu.lozouet@chu-rouen.fr
Abstract
Introduction: Intraspinal extradural arthrosynovial cysts, which belong to the spectrum of degenerative spinal diseases are mainly located at lumbar level and their location at cervical level joint is therefore unusual. The most common surgical approach for symptomatic arthrosynovial cervical cyst remains a direct resection of the cyst by a cervical hemilaminectomy with or without a posterior arthrodesis. However, another surgical approach may also be discussed when considering the cyst as a result of a local spinal instability or hypermobility.
Case Report: We report in this work the case of a patient with cervical radiculopathy due to intraspinal extradural compressive arthrosynovial cervical cyst which was treated by anterior discectomy and fusion without direct resection of the cyst. The post-operative radiological control performed at 3 months showed a complete regression of the cyst with a patient pain-free. To the best of our knowledge, this is the first case of intraspinal cervical degenerative cyst at C7-T1 level treated by anterior approach and fusion without direct cyst resection.
Conclusion: For the treatment of a joint spinal cervical cyst, the anterior approach is a relevant option that gives the advantages to respect the posterior cervical muscles and articular structures.
Keywords: Intraspinal cervical cyst, anterior discectomy and fusion, hemilaminectomy.
Cystic joint lesions belong to the spectrum of degenerative joint pathologies and were first described in 1877 by Baker for the knee joint [1]. Synovial spinal cysts are usually asymptomatic and they start giving clinical signs most often following an intracystic bleeding [2-4] or when they increase in size. Genesis of these cysts has been explored by many studies and it seems that traumatisms [2], and segmental hypermobility [5,6] are involved. For symptomatic synovial cervical cysts, a rare disorder, the surgical treatment described in literature is leaded by posterior laminectomy and direct removal of the cyst potentially associated with posterior fusion. An anterior approach is also considered, offering the advantage of treating the cyst without compromising cervical stability and while respecting the posterior neck muscles. Below, we present a case of a patient who was successfully treated using anterior approach.
We report the case of a 54-year-old patient, with medical history of breast cancer 10 years ago, consulting for 2-month history of a mild neck pain with radiation in the right upper extremity. None cervical traumatic injury was described by the patient in the past. The patient reported also paresthesia and right-hand weakness for 1 year. There was no pain in the left arm. Neurological examination revealed right C8 radicular pain without any other clinical sign. Magnetic resonance imaging (MRI) of the cervical spine (Fig. 1a and b) showed a right extradural cyst in T1-isosignal and T2-hyposignal reflecting the spinal cord with the right foraminal stenosis at level C7-T1 associated with a degenerative aspect of C7-T1 disk, inducing nerve root compression. There were no pre-operative dynamic X-rays.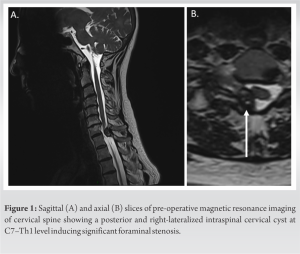
Despite best medical treatment, the patient kept disabling radicular pain and a surgical treatment was decided. Because an abnormal articular mobility at the C7-T1 level was strongly suspected, a surgical approach including a cervical fusion was preferred to a decompressive surgery alone. An anterior fusion without direct removal of the cyst was retained by the surgical staff. Surgical treatment was anterior discectomy of the cervical disk C7-Th1 and arthrodesis by an intersomatic cage and a C7-Th1 anterior plate. In the immediate post-operative period, there was no dyspnea, no dysphagia. As expected, there was no initial improvement in the right arm or neck pain. Post-operative X-ray (Fig. 2a) was conducted, revealing correctly placed surgical implants.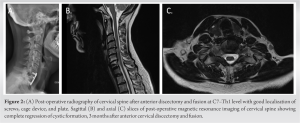
Patient discharged at day 4.
Three months later, the patient was totally free of symptom without neck or right arm pain, motor deficit, and walking disorder. Post-operative cervical MRI (Fig. 2b and c) done at 3 months showed a complete regression of the cervical cyst at the level C7-T1.
Intraspinal degenerative cysts encompass a broad category of spinal cysts including cyst from the disc, ligamentum flavum, and joints, according to the definition of Shima et al. [7]. The pathogenesis of these cysts remains unclear, but degenerative lesions, repetitive microtraumas, and joint hypermobility seem to lead to synovium injury and to cyst formation [5]. Symptomatic synovial cysts are more frequently found in the lumbar spine compared to the cervical spine [8]. Intraspinal cervical degenerative cyst (ICDC) remains rare with approximately 200 cases documented in the literature, representing 6.6% of all spinal cysts described in the literature [8]. The rarity of ICDC highlights the need for further research to better understand their pathogenesis and management. The pathogenesis of cervical and lumbar cysts appears to differ. Lumbar cysts are commonly found at L4–L5 level [6,8], mostly involved in degenerative lesions of lumbar spine. In contrast, cervical degenerative lesions often occur at C4–C5, C5–C6, and C6–C7 levels [9,10], whereas cysts occurred usually at C1–C2 (30.1%) and C7–T1 (38%) [11] levels suggesting that the mechanism of these degenerative cysts is different. The increased prevalence at C7–T1 level may be due to the greater mobility of the cervical spine in comparison with thoracic spine [12]. Many theories exist for cystic formations at C1–C2 level, such as congenital factors or deficiency of arterial blood, but segmental instability seems to be the main at this level [13,14]. There is currently no consensus on the management of such lesions. Usually, ICDC is treated with hemilaminectomy with cyst resection without systematic posterior fusion [8]. Alternative surgical approaches such as anterior corporectomy with fusion and direct cyst resection [4], laminectomy [15], or CT aspiration [16] have also been reported with favorable neurological outcomes and cyst regression. The posterior approach could probably be considered as the gold standard, offering minimal risk of recurrence and good neurological outcome [7,17]. However, the recurrence of painful symptoms was found in nine out of 35 patients who underwent a posterior surgical approach for symptomatic cervical cysts most often without fusion. Interestingly, post-operative imaging showed no cysts in patients with recurrent pain [15]. Regarding C1–C2 cysts in the literature, some patients with atlantoaxial articular cysts were successfully treated conservatively using a Philadelphia collar leading to good neurological outcome and cyst regression [18,19]. Other patients with atlantoaxial cysts achieved success with posterior fusion alone without direct cyst resection [13,20,21]. This implies that segmental stabilization and fixation consequently enable the indirect resorption of the cervical cyst at this cervical level. To the best of our knowledge, this is the first case of ICDC at C7–T1 level treated by undirect approach involving anterior cervical discectomy and fusion without direct cyst resection. Our surgical strategy was based on the notion that abnormal articular mobility was the primary contributor to the development of this cyst. Our surgical approach and its results lend support to the hypothesis that the pathophysiology underlying the formation of this cyst is likely associated with abnormal articular mobility. Existing literature extensively studies the clinical outcome and morbidity of anterior approach compared to posterior approach, with or without fusion, particularly in the context of treating degenerative cervical myelopathy. It is noteworthy that in the majority of these studies, minimal differences or none at all are observed in terms of morbidity, complications, and clinical outcomes between anterior and posterior approaches for the treatment of degenerative cervical myelopathy [22-24]. Anterior discectomy and fusion seem to be more preferable to laminoplasty alone due to the risk of loss of lordosis without posterior fixation [25]. Anterior approach allows for greater preservation of the posterior muscular and articular structures and would facilitate the management of any associated discopathy. In our specific case, the patient did not have any motor deficit or symptoms indicative severe medullar compression symptoms that would contraindicate the use of an anterior approach. In such instances, rapid decompression through laminectomy or hemilaminectomy with direct cyst resection is recommended with fusion considerations being made on a case-by-case basis. It is worth noting that spontaneous regression of the cyst can occur, which might also account for our results. However, this appears to be an exceedingly rare event, documented in only one case in the literature [26]. Given the potentially recurrent nature of cysts in the mid to long term, our follow-up, limited to 3 months, may not suffice. Extended monitoring is essential for a comprehensive understanding of the outcomes, especially considering the potential for recurrence in these lesions. The main limitation of this study is that it involves only a single patient, justified by the rarity of the pathology, especially at the cervical level. Moreover, the patient’s follow-up duration is short, and the risk of recurrence cannot be ruled out. Nevertheless, patients with cervical cysts, without motor deficits or signs of neurological compression necessitating urgent surgical decompression, especially when associated with cervical discopathy and lordosis deficiency, appear to be potential candidates for indirect treatment through an anterior approach. However, this hypothesis should be validated by further studies.
Our case potentially introduces a novel surgical indication for anterior discectomy and fusion for the treatment of cervical cysts usually treated by posterior approach and supports the hypothesis of excessive joint mobility for the genesis of these cervical cysts. Nevertheless, this is the first case treated by this approach and it does not seem to be suitable for patients requiring rapid nerve or spinal cord decompression. This surgical treatment needs to be studied further.
- Pathogenesis and treatment of intraspinal extradural arthrosynovial cysts are not well known
- Segmental cervical instability seems to be a key point for their development
- Anterior cervical discectomy and fusion for arthrosynovial cervical cysts could be an alternative to posterior approach.
References
- 1.Baker WM. On the formation of synovial cysts in the leg in connection with disease of the knee-joint. 1877. Clin Orthop Relat Res 1994;299:2-10 [Google Scholar | PubMed]
- 2.Yarde WL, Arnold PM, Kepes JJ, O'Boynick PL, Wilkinson SB, Batnitzky S. Synovial cysts of the lumbar spine: diagnosis, surgical management, and pathogenesis. Report of eight cases. Surg Neurol 1995;43:459-64. [Google Scholar | PubMed]
- 3.Wang YY, McKelvie P, Trost N, Murphy MA. Trauma as a precipitant of haemorrhage in synovial cysts. J Clin Neurosci 2004;11:436-9. [Google Scholar | PubMed]
- 4.Jabre A, Shahbabian S, Keller JT. Synovial cyst of the cervical spine. Neurosurgery 1987;20:316‑8. [Google Scholar | PubMed]
- 5.Howington JU, Connolly ES, Voorhies RM. Intraspinal synovial cysts: 10-year experience at the Ochsner Clinic. J Neurosurg 1999;91:193-9. [Google Scholar | PubMed]
- 6.Epstein NE. Lumbar synovial cysts: A review of diagnosis, surgical management, and outcome assessment. J Spinal Disord Tech 2004;17:321-5. [Google Scholar | PubMed]
- 7.Shima Y, Rothman SL, Yasura K, Takahashi S. Degenerative intraspinal cyst of the cervical spine: Case report and literature review. Spine (Phila Pa 1976) 2002;27:E18-22. [Google Scholar | PubMed]
- 8.Bruder M, Cattani A, Gessler F, Droste C, Setzer M, Seifert V, et al. Synovial cysts of the spine: Long-term follow-up after surgical treatment of 141 cases in a single-center series and comprehensive literature review of 2900 degenerative spinal cysts. J Neurosurg Spine 2017;27:256-67. [Google Scholar | PubMed]
- 9.Chagas H, Domingues F, Aversa A, Vidal Fonseca AL, de Souza JM. Cervical spondylotic myelopathy: 10 years of prospective outcome analysis of anterior decompression and fusion. Surg Neurol 2005;64 Suppl 1:S130-5. [Google Scholar | PubMed]
- 10.Sampath P, Bendebba M, Davis JD, Ducker T. Outcome in patients with cervical radiculopathy. Prospective, multicenter study with independent clinical review. Spine (Phila Pa 1976) 1999;24:591-7. [Google Scholar | PubMed]
- 11.Machino M, Yukawa Y, Ito K, Kato F. Cervical degenerative intraspinal cyst: A case report and literature review involving 132 cases. BMJ Case Rep 2012;2012:bcr2012007126. [Google Scholar | PubMed]
- 12.Krauss WE, Atkinson JL, Miller GM. Juxtafacet cysts of the cervical spine. Neurosurgery 1998;43:1363-8. [Google Scholar | PubMed]
- 13.Le Pape S, Gauthé R, Latrobe C, Leroux J, Roussignol X, Ould-Slimane M. Cervical myelopathy involving os odontoideum and retro-odontoid cyst treated with Harms C1-C2 arthrodesis. Orthop Traumatol Surg Res 2016;102:817-20. [Google Scholar | PubMed]
- 14.Guerrouj I, Abbou W, Aichouni N, Skiker I, Kamaoui I. Cervical myelopathy involving os odontoideum with retro-odontoid cyst and atlanto-axial instability: A case report. Radiol Case Rep 2022;17:1982-5. [Google Scholar | PubMed]
- 15.Lyons MK, Birch BD, Krauss WE, Patel NP, Nottmeier EW, Boucher OK. Subaxial cervical synovial cysts: Report of 35 histologically confirmed surgically treated cases and review of the literature. Spine (Phila Pa 1976) 2011;36:E1285-9. [Google Scholar | PubMed]
- 16.Kostanian VJ, Mathews MS. CT Guided aspiration of a cervical synovial cyst. Case report and technical note. Interv Neuroradiol 2007;13:295-8. [Google Scholar | PubMed]
- 17.Lunardi P, Acqui M, Ricci G, Agrillo A, Ferrante L. Cervical synovial cysts: Case report and review of the literature. Eur Spine J 1999;8:232-7. [Google Scholar | PubMed]
- 18.Sagiuchi T, Shimizu S, Tanaka R, Tachibana S, Fujii K. Regression of an atlantoaxial degenerative articular cyst associated with subluxation during conservative treatment. Case report and review of the literature. J Neurosurg Spine 2006;5:161-4. [Google Scholar | PubMed]
- 19.Cecchi PC, Peltz MT, Rizzo P, Musumeci A, Pinna G, Schwarz A. Conservative treatment of an atlantoaxial degenerative articular cyst: Case report. Spine J 2008;8:687-90. [Google Scholar | PubMed]
- 20.Puffer RC, Van Gompel JJ, Morris JM, Krauss WE. Resolution of cystic deterioration of the C1-2 articulation with posterior fusion: treatment implications for asymptomatic patients. World Neurosurg 2013;79:773-8. [Google Scholar | PubMed]
- 21.Morio Y, Yoshioka T, Nagashima H, Hagino H, Teshima R. Intraspinal synovial cyst communicating with the C1-C2 facet joints and subarachnoid space associated with rheumatoid atlantoaxial instability. Spine (Phila Pa 1976) 2003;28:E492-5. [Google Scholar | PubMed]
- 22.Jiang L, Tan M, Dong L, Yang F, Yi P, Tang X, et al. Comparison of anterior decompression and fusion with posterior laminoplasty for multilevel cervical compressive myelopathy: A systematic review and meta-analysis. J Spinal Disord Tech 2015;28:282-90. [Google Scholar | PubMed]
- 23.Wang B, Lü G, Kuang L. Anterior cervical discectomy and fusion with stand-alone anchored cages versus posterior laminectomy and fusion for four-level cervical spondylotic myelopathy: A retrospective study with 2-year follow-up. BMC Musculoskelet Disord 2018;19:216. [Google Scholar | PubMed]
- 24.Wang X, Liu H, Li J, Sun Y, Zhang F, Guo L, et al. Comparison of anterior cervical discectomy and fusion with cervical laminectomy and fusion in the treatment of 4‐level cervical spondylotic myelopathy. Orthop Surg 2021;???:13058. [Google Scholar | PubMed]
- 25.Montano N, Ricciardi L, Olivi A. Comparison of anterior cervical decompression and fusion versus laminoplasty in the treatment of multilevel cervical spondylotic myelopathy: A meta-analysis of clinical and radiological outcomes. World Neurosurg 2019;130:530-6.e2. [Google Scholar | PubMed]
- 26.Colen CB, Rengachary S. Spontaneous resolution of a cervical synovial cyst. Case illustration. J Neurosurg Spine 2006;4:186. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 November 23, 2017 A Unique Case of Cervical Myelopathy in an Adult Patient with Scheie Syndrome
November 23, 2017 A Unique Case of Cervical Myelopathy in an Adult Patient with Scheie Syndrome May 10, 2020 Delayed Treatment of a Galeazzi Fracture Using an External Ring Fixator
May 10, 2020 Delayed Treatment of a Galeazzi Fracture Using an External Ring Fixator July 1, 2026 Short-term Functional Outcomes of Shoulder Girdle Limb Salvage in Primary Bone Tumors: A 2-year Follow-up Study
July 1, 2026 Short-term Functional Outcomes of Shoulder Girdle Limb Salvage in Primary Bone Tumors: A 2-year Follow-up Study January 1, 2026 Performance of ChatGPT‑5 in Diagnosing Fractures on Proximal Humerus and Intertrochanteric Femur X-Rays
January 1, 2026 Performance of ChatGPT‑5 in Diagnosing Fractures on Proximal Humerus and Intertrochanteric Femur X-Rays