
Limb salvage surgery using modern reconstructive techniques provides satisfactory functional outcomes and preserves limb function in shoulder girdle tumours, offering an effective alternative to amputation.
Dr. J Nishanth Reddy, Department of Orthopaedics, Vydehi Institute of Medical Sciences and Research Centre, Whitefield, Bengaluru - 560 066, Karnataka, India. E-mail: drnishanthreddyj@gmail.com
Abstract
Introduction: The shoulder girdle, encompassing the proximal humerus, scapula, lateral third of the clavicle, and surrounding soft tissues, is the third most frequent site for bone tumours. The proximal humerus is the most commonly affected area, followed by the scapula and clavicle. Managing malignant or aggressive benign bone tumors in this region is particularly challenging due to the proximity to vital neurovascular structures and the need to maintain both stability and dexterity in the shoulder. While traditional treatment often involved extensive resections, contemporary limb salvage techniques focus on preserving function while ensuring effective tumour control.
Case Series: This prospective study included 18 patients who underwent various limb salvage procedures at the Department of Orthopaedics, Vydehi Institute of Medical Sciences and Research Centre, in Bengaluru, between 2012 and 2019, with a minimum follow-up of 2 years. Diagnosis and staging were performed using imaging modalities and core needle biopsies, with musculoskeletal tumours staged according to the Enneking System. Functional outcomes were assessed using the Musculoskeletal Tumour Society Rating Scale (MSTS). Surgical techniques varied and included endoprosthetic reconstruction, arthrodesis with fibular grafting and plating, and plate fixation with primary shortening. Among the 18 patients, the majority (61%) had giant cell tumours, followed by aneurysmal bone cysts (17%), chondrosarcoma (11%), and osteosarcoma (11%). Functional outcomes, as measured by the MSTS, showed a 75% satisfactory rate. The study population was composed of 55.56% males and 44.44% females. Key parameters evaluated included pain, functional activity, hand positioning, dexterity, lifting ability, and emotional acceptance.
Conclusion: Limb salvage surgery for primary bone tumours of the shoulder girdle offers favourable functional outcomes and represents a viable alternative to amputation. Modern reconstruction techniques, such as endoprosthetic reconstruction and fibular grafting with plating, achieve satisfactory results in both function and appearance. The MSTS scoring system is an effective tool for assessing postoperative functional status, and there is a growing preference for less aggressive surgical techniques that preserve limb function while ensuring tumour control.
Keywords: Bone tumors, endoprosthetic reconstruction, limb salvage, musculoskeletal tumor society, shoulder girdle.
The shoulder girdle, which includes the proximal humerus, scapula, 1/3 lateral clavicle, and surrounding soft tissue, is the third most prevalent location for bone tumours. The most common place in the shoulder girdle is the proximal humerus, followed by the scapula and clavicle. Orthopaedic oncologists face significant challenges when treating malignant or invasive benign bone tumours in this region [1]. Tumours of the shoulder girdle are always located near the neurovascular bundle, making it difficult to resolve the conflict between shoulder stability and dexterity. Local excision of bone and muscle may result in inadequate functional outcomes and put the patient at risk of a local recurrence. Thus, it has long been generally believed that local resection of malignant bone tumours of the shoulder girdle is risky [2]. Classic surgery consists of en bloc excision of the entire scapula, proximal humerus, lateral clavicle, and surrounding soft tissue, followed by replantation of the shortened limb, known as type VI resection. Modified Tikhoff-Linberg methods, also known as type-IV and type-V resection, have been developed to lower the extent of resection while improving the function of the remaining extremity [3]. With improving survival rates for patients with sarcomas, the detrimental effects of severe ablative excision become more apparent, prompting the development of a less aggressive surgical technique. Various limb salvage methods are currently being tested to keep the functioning limb while maintaining tumour control. Limb salvage operations for bone tumours of the shoulder girdle, like those for other anatomical sites, consist of three steps: complete tumour excision, bone defect restoration, and adequate soft tissue covering. Enneking et al. developed a system in 1990 to describe and compare the scope of tumour resection and therapeutic outcomes, but it was unable to adequately express the surgical margins, the relationship of the tumour to anatomical compartments, the abductor mechanism, the status of the glenohumeral joint, and the magnitude of the surgery [4]. Malawer proposed a surgical classification system that classified tumour resections into type-I, type-II, type-III, type-IV, type-V, and type-VI. These were further categorised into two subclasses based on the state of the shoulder’s abduction system (deltoid and rotator cuff) [3]. Due to an improved understanding of the biological behavior of musculoskeletal cancers, the use of appropriate adjuvant therapy, and the development of bone defect restoration, 80–90% of malignant tumours of the shoulder girdle can be safely resected using various limb salvage methods [1]. In recent years, the possibilities for reconstruction have expanded, and with better surgical alternatives, postoperative functional capacities have improved. Nowadays, common surgical options include anatomical hemiarthroplasty, allograft-prosthesis composite, and reverse shoulder megaprothesis. The reverse shoulder prosthesis was originally designed for individuals with rotator cuff deficiency and is best suited to patients who present with irreparable rotator cuff injuries and subsequent loss of function. As a result, this prosthesis is also suited for shoulder joint reconstruction following oncologic proximal humerus resections [5]. Following bone tumour removal, bone defect restoration was determined by criteria such as the patient’s economic status, cancer type and extension, surgeon skills, and instrument availability. The present study comprises 18 patients who underwent limb salvage procedures.
This is a prospective study of 18 patients who had various limb salvage procedures performed at the Department of Orthopaedics, Vydehi Institute of Medical Sciences and Research Centre in Bengaluru, India. The study was conducted between 2012 and 2019, with a minimum follow-up of 2 years. The outcome data were analysed at the end of 2 years. Imaging modalities such as radiography, computed tomography, magnetic resonance imaging, bone scans, and positron emission tomography (if required) were used to diagnose the type of tumour and staging. A core needle biopsy was used to confirm the histological diagnosis of all tumours. All patients were staged with the Enneking System for Benign and Malignant Musculoskeletal Tumors [4]. The functional result of the procedure was assessed using the Musculoskeletal Tumour Society Rating Scale (MSTS) [6]. The scoring evaluates six factors: pain, function, emotional acceptance, hand positioning, dexterity, and lifting ability for upper extremity tumours, or walking, gait, and use of supports for lower extremity tumours. Each factor is scored on a scale of 0–5, with 0 being the worst and 5 being the best. The total score ranges from 0 to 30, with higher scores indicating better functional outcomes and lower impact of the tumour and its treatment on the patient’s quality of life.
Inclusion and exclusion criteria:
Patients of all ages belonging to either sex diagnosed with giant cell tumors (GCTs) (aggressive and recurrent), osteosarcomas, chondrosarcomas of the proximal humerus, and aneurysmal bone cysts (ABCs) were included in the study. The exclusion criteria comprised patients who had involvement of three or more key components, i.e., bone, nerves, vessels, and soft-tissue involvement.
Endo-prosthetic reconstruction:
The patients underwent tumour excision with endoprosthetic reconstruction/arthrodesis with fibular grafting and plating/plate fixation with primary shortening, depending on the type, location, and stage of the tumour. Standard sutures were employed to locate key soft-tissue components, such as the glenohumeral capsule and tendon stumps. To rehabilitate the damaged region, the endoprosthesis’s modular components, including the humeral head, body, and shaft, were connected to ensure proper soft-tissue tensioning. Cemented/uncemented intramedullary stems were chosen. Non-absorbable sutures were used to attach proximal soft tissues to specific holes in the endoprosthesis. Following surgery, patients were given a sling and were advised to avoid putting weight on the afflicted arm and limit shoulder movement (Fig. 1).
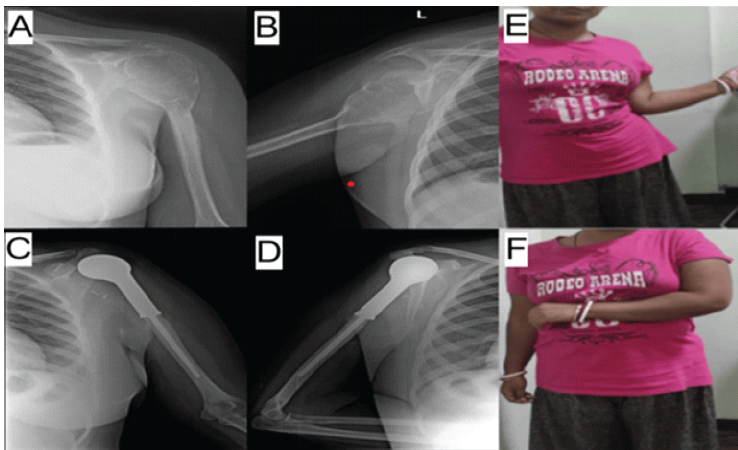
Figure 1: Case of giant cell tumor (GCT) of lefe proximal humerus managed by tumor excision with endoprosthetic reconstruction. (a) Pre-operative anteroposterior (AP) X-ray of GCT of left proximal humerus. (b) Pre-operative lateral X-ray of GCT of left proximal humerus. (c) Post-operative AP X-ray of of endoprosthetic reconstruction of left proximal humerus. (d) Post-operative lateral X-ray of endoprosthetic reconstruction of left proximal humerus. (e) 2-year follow-up range of movement (external rotation) of left shoulder. (f) 2-year follow-up range of movement (internal rotation) of left shoulder.
Arthrodesis with fibular grafting and plating:
This procedure involved a typical S-shaped curvilinear incision crossing the scapula’s spine and extending to the anterolateral aspect of the arm. The tumor was exposed through soft-tissue dissection and was eliminated. Tenodesis of the biceps tendon was performed after the rotator cuff was resected from the proximal humerus. For fixation, a fibular graft and locking compression plate were employed. Afterward, the patient received a hanging U-slab, and the wound was closed in layers (Fig. 2).
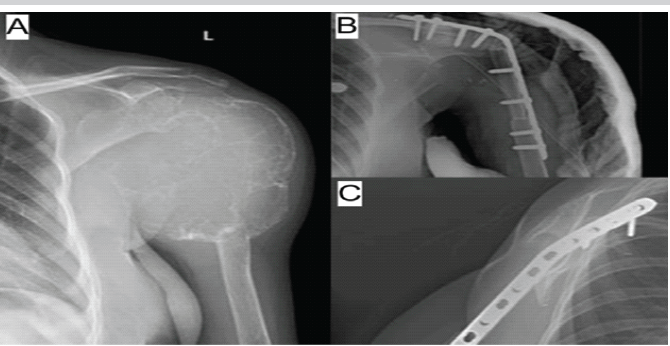
Figure 2: Case of osteosarcoma of proximal humerus managed with tumor excision and shoulder arthrodesis with fibular grafting and locking compression plate (LCP). (a) Antero-posterior view of osteosarcoma of the left shoulder. (b) Antero-posterior view of tumor excision with tumor excision and shoulder arthrodesis with fibular grafting and LCP. (c) Lateral view of tumor excision with tumor excision and shoulder arthrodesis with fibular grafting and LCP.
Plate fixation with primary shortening:
A standard antero-medial approach to the proximal humerus was taken. Soft-tissue dissection was carried out to expose the tumour. Resection of the tumor was performed, followed by the use of an appropriately sized proximal locking plate to fix the proximal humerus. The extent of primary shortening was noted. The wound closed in layers, and the patients were given an arm sling for support, followed by partial mobilisation after a few days of surgery (Fig. 3).
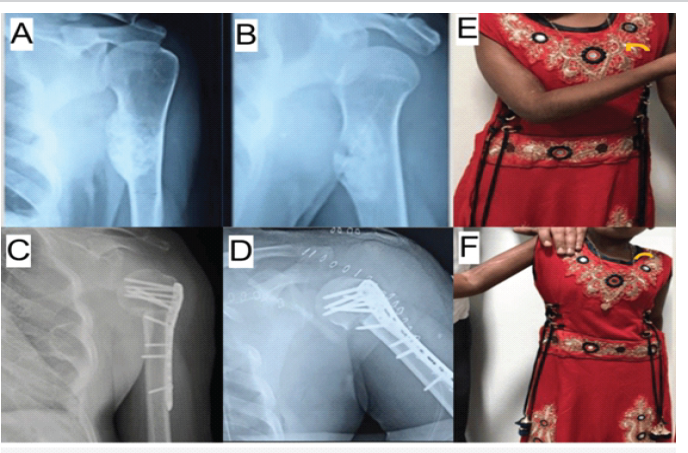
Figure 3: Chondrosarcoma of left proximal humerus managed with wide tumor excision with primary shortening and plate fixation. (a) Antero-posterior X-ray of chondrosarcoma of left proximal humerus. (b) Lateral X-ray of chondrosarcoma of left proximal humerus. (c) Antero-posterior X-ray of chondrosarcoma of left proximal humerus managed with wide tumor excision with primary shortening and plate fixation. (d) Lateral X-ray of chondrosarcoma of left proximal humerus managed with wide tumor excision with primary shortening and plate fixation. (e) 2-year follw-up range of movements (internal rotation) of left shoulder. (f) 2-year follw-up range of movements (external rotation) of left shoulder.
Statistical analysis:
This study uses descriptive statistics to report the frequency and percentage distributions of key variables. The percentages provided allow for easy comparison and interpretation of the results across various dimensions.
The study included 18 patients with various types of shoulder girdle tumours, with a majority (61%) diagnosed with GCTs. Other cases included ABC (17%), chondrosarcoma (11%), and osteosarcoma (11%). The gender distribution was 55.56% male and 44.44% female (Tables 1 and 2).
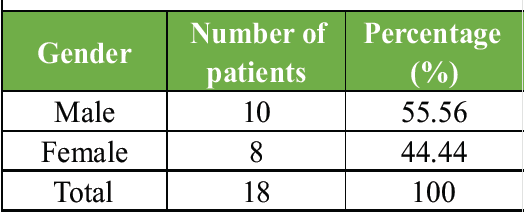
Table 1: Patient demographics
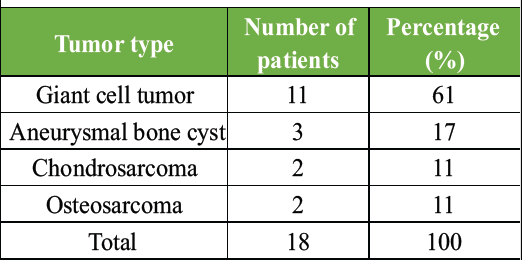
Table 2: Tumor distribution
MSTS score:
Functional outcomes were assessed using the MSTS score, which evaluates parameters such as pain, functional activity, hand positioning, dexterity, lifting ability (muscle power), and emotional acceptance. The MSTS scoring system ranges from 0 to 30, with higher scores indicating better functional outcomes. The MSTS scores in this study showed a mean of 22.5 out of 30, indicating a 75% satisfactory rate overall (Table 3).
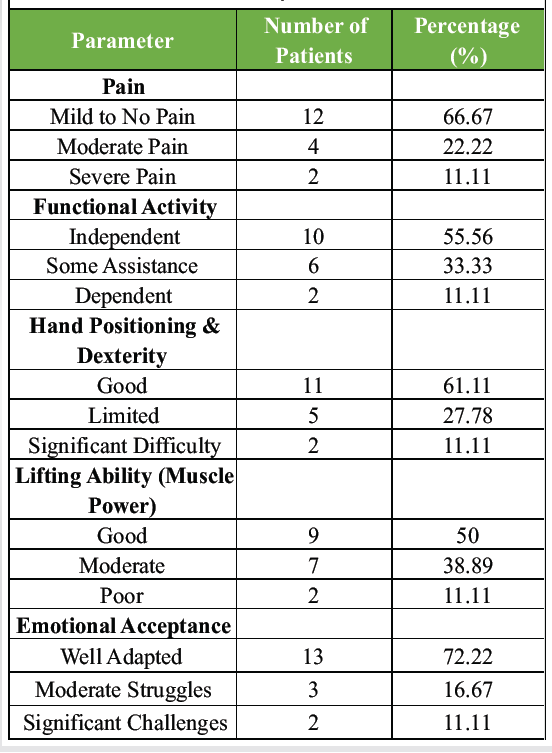
Table 3: Musculoskeletal tumor society rating scale score components and outcomes
Pain:
This category includes 12 patients, representing 66.67% of the study population. These patients reported experiencing either no pain or mild pain postoperatively, indicating successful pain management and a positive recovery process. Four patients, or 22.22%, experienced moderate pain. This level of pain may suggest the need for ongoing pain management strategies and could be indicative of the surgical or rehabilitative challenges faced by these patients. Two patients (11.11%) reported severe pain, highlighting a subgroup with significant postoperative discomfort, which could impact their overall recovery and quality of life.
Functional activity:
A total of 10 patients (55.56%) were able to perform daily activities independently, reflecting good functional recovery and the effectiveness of the surgical and rehabilitative interventions. Six patients (33.33%) required some assistance with daily activities, indicating a partial recovery and the need for continued support and rehabilitation. Two patients (11.11%) were dependent on others for most daily activities, suggesting poor functional recovery and highlighting the need for further investigation into the factors contributing to this outcome.
Hand positioning and dexterity:
Eleven patients (61.11%) exhibited good hand positioning and dexterity, demonstrating satisfactory motor skills and fine motor control post-surgery. Five patients (27.78%) had limited dexterity, suggesting some difficulties with fine motor tasks that might necessitate additional rehabilitative efforts. Two patients (11.11%) faced significant challenges with hand positioning and dexterity, indicating a severe impact on their fine motor abilities and overall functional outcomes.
Lifting ability (muscle power):
Nine patients (50%) showed good muscle power, indicating strong lifting ability and good functional recovery of the shoulder muscles. Seven patients (38.89%) demonstrated moderate muscle power, suggesting a partial recovery with some limitations in lifting and strength. Two patients (11.11%) had poor muscle power, reflecting significant functional impairment and the need for focused rehabilitative strategies to improve muscle strength.
Emotional acceptance:
Thirteen patients (72.22%) showed a good degree of emotional acceptance post-surgery, showing good psychological resilience and acceptance of their condition. Three patients (16.67%) experienced moderate emotional struggles, indicating some psychological challenges that might require counselling or additional support. Two patients (11.11%) faced significant emotional challenges, suggesting a need for comprehensive psychological support to aid in their overall recovery and quality of life. These outcomes indicate that limb salvage surgery for primary bone tumours of the shoulder girdle provides satisfactory functional results, with most of the patients experiencing minimal pain and retaining a good degree of independence in daily activities. Emotional acceptance was generally positive, further supporting the viability of limb salvage over more radical surgical options.
Our study found that patients undergoing limb salvage surgery for primary bone tumours of the shoulder girdle had satisfactory functional outcomes, with a mean MSTS score of 23.5 ± 3.1 at the 2-year follow-up. These results corroborate the findings of Yang et al., who reported good functional outcomes in patients who underwent limb-sparing surgery for shoulder girdle bone tumours, with a focus on preserving limb function and achieving satisfactory oncological control [1]. Similar to our findings, Denissen et al. conducted a systematic review and meta-analysis on the functional outcomes of patients with reverse shoulder megaprostheses following the resection of malignant bone tumours in the proximal humerus [5]. They reported a mean MSTS score of 24.2, highlighting the effectiveness of this surgical approach in preserving shoulder function and improving patient quality of life. Our study’s results are also consistent with those of Öztürk et al., who evaluated the surgical and functional outcomes of malignant tumours of the shoulder girdle. They found that limb salvage surgeries, particularly those employing endoprosthetic reconstruction, yielded favourable functional results, with patients achieving an MSTS score comparable to our findings [7].
Comparison with aggressive surgical approaches:
In contrast, aggressive surgical approaches, such as forequarter amputation, have been associated with significantly poorer functional outcomes. Sim et al. reported that patients undergoing forequarter amputation experienced substantial functional limitations, which were not observed in our cohort undergoing limb salvage surgery [2]. This highlights the importance of less aggressive surgical techniques in maintaining limb function while ensuring effective tumour control.
Advances in surgical techniques:
The current study’s use of reverse shoulder megaprostheses and other advanced reconstructive techniques is in line with recent trends in orthopaedic oncology. Malawer and Enneking et al. provided foundational work on the classification and surgical approaches for shoulder girdle tumours, which have been instrumental in developing modern limb salvage techniques [3,4]. Recent advancements in prosthetic design and surgical techniques have further improved outcomes. For example, a case report by Kapoor demonstrated the successful use of partial scapulectomy and reverse shoulder prosthesis in treating GCTs of the scapula, achieving excellent functional recovery [8].
Functional outcomes and rehabilitation:
The importance of rehabilitation in optimising functional outcomes cannot be overstated. Studies by Chu et al. and Das et al. have underscored the role of early and targeted rehabilitation protocols in enhancing recovery and functional status post-surgery [9,10]. Our findings support these observations, as patients who adhered to a structured rehabilitation programme demonstrated significantly better functional outcomes, as evidenced by their MSTS scores.
Limitations of the study:
While this study provides valuable insights into the functional outcomes of limb salvage surgery for primary bone tumors of the shoulder girdle, there are notable limitations, such as a small sample size, the single-center nature of the study, limited follow-up duration, and heterogeneity of surgical techniques. Addressing these limitations in future studies would enhance the reliability and applicability of the findings, contributing to improved patient care in the field of orthopaedic oncology.
This study reaffirms the efficacy of limb salvage surgery with advanced reconstructive techniques in treating primary bone tumours of the shoulder girdle. The functional outcomes, reflected by favourable MSTS scores, demonstrate the success of these procedures in preserving shoulder function and enhancing patient quality of life. Compared to more radical surgical options, limb salvage surgery offers significant advantages in maintaining functional independence while achieving effective tumour control. These findings support the continued use and ongoing refinement of limb-sparing techniques as a preferred approach in orthopaedic oncology, with a focus on improving both survival and functional outcomes for patients.
Limb salvage surgery for primary shoulder girdle bone tumours provides effective oncological control while preserving limb function, independence, and quality of life, making it a preferred alternative to amputation when adequate surgical margins can be achieved.
References
- 1. Yang Q, Li J, Yang Z, Li X, Li Z. Limb sparing surgery for bone tumours of the shoulder girdle: The oncological and functional results. Int Orthop 2010;34:869-75. [Google Scholar] [PubMed]
- 2. Sim FH, Pritchard DJ, Ivins JC. Forequarter amputation. Orthop Clin North Am 1977;8:921-31. [Google Scholar] [PubMed]
- 3. Malawer MM. Tumors of the shoulder girdle. Technique of resection and description of a surgical classification. Orthop Clin North Am 1991;22:7-35. [Google Scholar] [PubMed]
- 4. Enneking W, Dunham W, Gebhardt M, Malawar M, Pritchard D. A system for the classification of skeletal resections. Chir Organi Mov 1990;75:217-40. [Google Scholar] [PubMed]
- 5. Denissen JJ, Koenders N, Van Hinte G, Groen F, Van Der Wees PJ, Van Der Geest IC, et al. Functional outcomes after reverse shoulder megaprosthesis following resection of malignant bone tumor in the proximal humerus: A systematic review and meta-analysis. JSES Int 2023;7:592-600. [Google Scholar] [PubMed]
- 6. Fukumothi DK, Pupo H, Reganin LA, Matte SR, Lima BS, Mattos CA. Functional assessment of endoprosthesis in the treatment of bone tumors. Rev Bras Ortop 2016;51:569-73. [Google Scholar] [PubMed]
- 7. Öztürk R, Arıkan ŞM, Toğral G, Güngör BŞ. Malignant tumors of the shoulder girdle: Surgical and functional outcomes. J Orthop Surg (Hong Kong) 2019;27:2309499019838355. [Google Scholar] [PubMed]
- 8. Kapoor A. Giant cell tumour of the scapula treated by partial scapulectomy. BMJ Case Rep 2019;12:e228424. [Google Scholar] [PubMed]
- 9. Chu JY, Yeh KT, Lee RP, Yu TC, Chen IH, Peng CH, et al. Open reduction and internal fixation with plating is beneficial in the early recovery stage for displaced midshaft clavicular fractures in patients aged 30-65 years old. Ci Ji Yi Xue Za Zhi 2018;30:242-6. [Google Scholar] [PubMed]
- 10. Das A, Rollins KE, Elliott K, Johnston P, Van-Rensburg L, Tytherleigh-Strong GM, et al. Early versus delayed operative intervention in displaced clavicle fractures. J Orthop Trauma 2014;28:119-23. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report
August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization
August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series
August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature
July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature