
WALANT is a surgical approach that uses local anesthetic and hemostatic drugs to create ideal conditions for hand surgery without sedation or a tourniquet which allows for more surgeries in an ambulatory setting, hence reducing costs and improving patient safety
Dr. Nilesh S Sakharkar, Department of Orthopaedics, Government Medical College and Hospital, Nagpur-440003, Maharashtra, India. E-mail: orthodrnilesh@gmail.com
Abstract
Introduction: To improve hemostasis and visibility, a tourniquet was used throughout the majority of hand and wrist procedures, despite the fact that patient experience unnecessary and excruciating pain from the tourniquet. The more current method known as wide-awake local anesthesia without tourniquet (WALANT) enables intraoperative function evaluation while the patient is completely conscious.
Materials and Methods: Individuals with displaced distal radius fractures that required surgery and isolated, non-concomitant injuries requiring spinal or general anesthesia were considered for WALANT technique. In our study, five patients underwent dorsal plate fixation and 20 patients underwent volar plate fixation. Patients receiving dorsal plate fixation required definite dorsal buttress to prevent radiocarpal dislocation.
Conclusion: The WALANT technique is a simple, reliable, and effective anesthetic method for internal fixation and open reduction of distal radius fractures. Since a tourniquet is not necessary, the patient is protected from the discomfort and risks associated with one.
Keywords: WALANT technique, distal end radius fracture, tourniquet, volar plating, dorsal plating.
Conventionally, the majority of wrist and hand surgeries are done under a tourniquet to have a bloodless and clear surgical field. However, prolonged tourniquet use causes discomfort, which is very unpleasant for patients. The use of a tourniquet mandates the use of regional anesthesia so that tourniquet site discomfort is taken care of. Tourniquet use has its own set of problems and complications later. However, older patients with extensive chronic medical illnesses are often unable to undergo surgery in a timely manner until they have been optimized and are deemed medically fit. Wide-awake local anesthesia without tourniquet technique (WALANT) is a more current approach where a patient is operated under local anesthesia without a tourniquet in which lidocaine and epinephrine are injected for local anesthesia and vasoconstriction, respectively. Since the patient is fully awake during the procedure, intraoperative assessment of function is possible [1,2]. Distal radius fractures are one of the most common injuries in orthopedic practice. They make up 8%−15% of all bony injuries in adults [3]. Recently, locking plate fixation has gained favor and helps maintain anatomical reduction and facilitates earlier return to normal daily activities. We used the WALANT technique since January 2020 on 10 patients to perform open reduction and plating for distal radius fracture. The purpose of this retrospective study was to evaluate the perioperative variables, advantages and complications, and clinical outcomes of open reduction and internal fixation (ORIF) for distal radius fractures under WALANT technique, which includes the operation time, the blood loss, the duration of hospitalization, the time of union, the range of motion (ROM) of the affected wrist, the pain, and the functional outcome score 1 year postoperatively.
From January 2020 to January 2021, 10 patients with distal radius fractures were treated. Patients with isolated without any concomitant injury which required spinal or general anesthesia with displaced distal radius fractures that required surgery were enrolled in the study. The patients were counseled before performing WALANT surgery. The whole procedure was explained and information about the content of the local injection solution and hemostatic agent were clearly explained to patients. Furthermore, the pros and cons of classical anesthesia were also informed. All patients were presented to our emergency department, a standard anterio-posterior and lateral X-ray were obtained and a slab was applied for immobilization. Patients were treated using volar plate fixation and dorsal plate according to the fracture pattern and depending on the surgeon’s preference. In our study, five patients were treated with volar plate fixation, and five patients were treated with dorsal plate fixation, those needed definite dorsal buttress to avoid radiocarpal subluxation.
WALANT technique
WALANT block was carried out about 20–30 min before the first incision. Preparation of solution was done before removal of cast (Fig. 1).
The injected solution comprised 20 mL of 0.9% normal saline and 20 mL of 1% lidocaine with 1:1,000,000 epinephrine. We also added 10 mL of bupivacaine for its long-term effect. Then, cast was removed and the surgical site was prepared using a sterile alcohol solution. The surgical approach was used according to fracture configuration, the modified Henrys approach was used for volar plating, and the classical Thomason approach was used for dorsal plating.
Surgical technique
The volar and dorsal skin marking was done using a sterile skin marker (Fig. 2 and 3).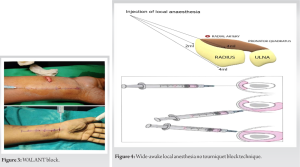
The styloid process of the radial bone was palpated, and four skin points were marked from about 10 cm proximal to the wrist crease and distal to the radial styloid process, approximately 2 cm apart from each other. WALANT case series protocol started with 3–5 mL of 1% lignocaine given dorsally in the fracture site as a hematoma block to minimize the discomfort while performing reduction maneuver. 5–10 mL of solution was injected subcutaneously along the skin marking using a 23G needle. Ensure that at least 1 cm of visible or palpable subcutaneous solution is injected. At each radial skin point, a needle was inserted and the bone was palpated. The periosteum was infiltrated adequately with solution, and it would eliminate pain and bleeding with bone maneuvers and drilling. 2 mL of the solution was injected subcutaneously and 4 mL was injected volar and 4 mL dorsally in a fan shape subperiosteally (Fig. 4).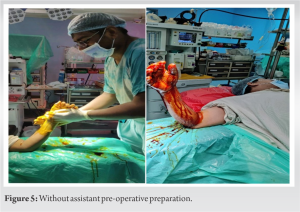
After about 15–20 min, the injected area became pale with a yellowish appearance. All patients had a visual analog scale (VAS) score of 0 at the beginning of the surgery. Here, the advantage of WALANT is that the patient can keep his hand in the air, there is no need of assistance here for painting draping (Fig. 5).
Volar plating
The procedure started as per modified Henry’s approach, with a longitudinal skin incision approximately 5–10 cm along the flexor carpi radialis (FCR) tendon. The FCR sheath was opened, and the tendon was retracted medially. The incision was progressed between the flexor pollicis longus and radial artery to achieve exposure of the pronator quadratus (PQ). The PQ then split in reverse L fashion and elevated for fracture reduction done with reduction maneuver. The volar plate is inserted and fixed with screws. Over the entire procedure, the patients were awake and after definitive fixation, the patients were asked to actively flex and extend their wrists and fingers to examine the stability of the fixation and no tendon impingement (Fig. 6).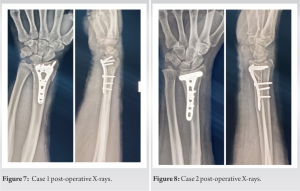
Dorsal plating
Using a single dorsal skin incision started according to Thomson’s approach, along the line between the third and fourth compartments, the extensor retinaculum was carefully dissected. Then, the extensor retinaculum was opened as far as needed for fracture reduction, plate placement, drilling procedures, and screw fixations. Again, patients were asked to do active flexion and extension of the wrist and finger to evaluate stability and tendon impingement. Fracture fixation and tendons were checked, and no abnormalities were noted. The skin was sutured and a soft dressing was applied.
Post-operative care and follow-up
Two doses of IV antibiotics postoperatively given and 1 g paracetamol IV 2 doses were given. Some patients need additional tramadol coverage. Patients were discharged on post-operative day 2 and followed up after 1 week in Outpatient Department (OPD). A short arm splint was given to patients for 1 week. Then, patients were taught to use passive wrist motion with flexion and extension from the removal of the splint to post-operative 1 month. Then, active ROM started using objects of 5 kg weight since the 2nd month postoperatively. Patients were followed up for 12 months postoperatively starting from 3 weeks, 6 weeks, and 12 weeks and thereafter on every 3 months. Anteroposterior (AP) and lateral wrist radiographs were obtained for the radiographic evaluation of the bone union after 3 weeks, 6 weeks, and 12 weeks, in which the fracture gap disappeared on the AP and lateral views. The functional outcomes using the quick disabilities of the arm, shoulder, and hand (quick DASH) questionnaire [4] were evaluated 12 months postoperatively, and the maximum ROM at the wrist was also recorded at every OPD visit.
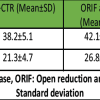
In our study, the average age of the patients was 47.52 years (range from 20 to 75 years). The average surgical time was 72.8 min (range 60–90 min). The average blood loss during surgery was 14.8 mL (range 10–30 mL). The union was said to be achieved when there were bridging callus in at least 3 cortices in two (AP and lateral) views and when there was no pain clinically. The average union time was 17.88 weeks (range from 15 to 30 weeks). The average post-operative day 1 VAS score was 1.52 (range 1–3). The average quick DASH score was 6.632 (range from 4.5 to 11.9). The patient with the highest quick DASH score of 11.9 was a 75-year-old male. Turning the key and using of fork with his injured wrist was particularly difficult for him. The average flexion was 69.2 (range 60–75) and the extension was 67.2 (range 50–75). In this study, there was no need for any secondary intervention to any patients for union, all patients achieved union. We did not observe any complications such as wound infection, finger necrosis, palpitation, or other complications (Fig. 7 and 8).
Conventionally, distal end radius fractures are treated under regional anesthesia or general anesthesia. We were dependent on tourniquet for hemostasis. However, surgeons were bound to complete surgeries within the tourniquet time limit, as the patients could not tolerate very long operation time because of tourniquet pain. Moreover, also prolonged tourniquet may result in nerve injury. Hutchinson and McClinton [5] and Maury and Roy [6] studied the tourniquet tolerance among healthy volunteers, and they observed that the average tolerance to the forearm tourniquet was 13 and 25 min, respectively, with temporary pain and paresthesia. The decision about general or regional anesthesia in older patients should be made with caution, because elderly patients with chronic conditions may decompensate due to acute physiological derangements induced on by anesthesia and surgery [7]. Some patients such as uremia patients with ipsilateral wrist fractures and arteriovenous shunts who could not be subjected to tourniquet applications, also patients with chronic illnesses such as chronic occlusive pulmonary disease or severe congestive heart failure, and other cardiovascular problems were unfit for general anesthesia. This patient needed to wait for surgery until they became fit. However, they need to bear the cost of various pre-operative work-ups and investigations. Again, the chances of intraoperative complications were high because of the delay in surgery. To avoid all these complications in recent years, the WALANT was developed. While performing WALANT, some systemic adverse reactions could occur such as anaphylactic shock. Lidocaine has some cardiotoxic features. To prevent these adverse reactions, we kept the injected dosage within the “safe” range of 7 mg/kg [8]. Ruxasagulwong et al. conducted a clinical trial in patients with minor orthopedic hand surgeries under WALANT block without tourniquet versus the conventional method with tourniquet use in 2015. They observed that the tourniquet’s pain and the amount of blood loss in the conventional group were significantly higher than in the wide-awake group [9]. We also observed similar results in our study, the average blood loss was 14.8 mL, and the amount of blood loss in the conventional group with tourniquet use was significantly higher because of vasodilatation and during the release of tourniquet pressure before suture to check for bleeding. There was no question of tourniquet pain as we performed surgeries without tourniquets. We performed all these procedures in the main operation room with strict sterile conditions and we gave 1 dose of antibiotic preoperatively 30 min prior, so did not encounter any infection and wound complications. Younge in 1989 [10] observed compartment syndrome may occur in distal radius fracture as a consequence of hematoma block during reduction. Moreover, in our study, the possibility of compartment syndrome was minimal, despite the large volume of WALANT solution because, unlike hematoma block, we performed an open volar or dorsal approach with partial fasciotomy of the forearm. In addition, we did not use tourniquet and did adequate hemostasis intraoperatively. We asked to perform wrist and finger motions to confirm the stability of fracture fixation intraoperatively, it also confirms that there is no impingement of implants in the tendons especially during dorsal plating. Ki Lee et al. in 2020 compared WALANT block versus conventional local anesthetic technique in minor hand surgeries and stated that, for post-operative management, the WALANT group showed significantly lower post-operative pain until the 1st day after surgery and significantly lower analgesic use until the 2nd day after surgery [11]. However, Moscato et al. did not show any significant difference in post-operative pain in patients with WALANT and regional block [12]. In our study, we also observed minimum use of analgesics in post-operative period and the average VAS score was 1.52. Ingall et al. observed quick DASH score of 9.8 in distal radius fracture fixation with ORIF plating at 9–12 months postoperatively [13]. In our study, we observed the quick DASH score of 6.63 at 12 months postoperatively. The quick DASH score in Moscato et al. study group was (4.93–7.27) in WALANT group and was (13.47–10.63) in conventional regional anesthesia group. It was significantly better compared to the RA group, with an 8.5-point difference between the two groups (P = 0.01). Another advantage of WALANT block was that there was no need for pre-operative fasting, especially in diabetic patients and reduces the chances of low blood sugar. There is no need to change or stop the anticoagulant therapy. The most important advantage of this technique is that the cost of pre-operative check-up is reduced and cutoff in the waiting period for fitness. Early treatment also benefited patients with good results and low complications. Although intraoperative active motion of the wrist and fingers are beneficial but this technique is not appropriate for all types of patients, especially those with a minor cognitive disorder or severe anxiety disorders. Our study had several limitations, such as its retrospective nature and small sample size. A larger study with a control group of general anesthesia without tourniquet was needed for comprehensive analysis.
The WALANT technique is an easily applied, safe, and efficient anesthetic technique for open reduction and internal fixation of distal radius fractures. It does not require tourniquet so it keeps the patient free from tourniquet pain and complications. Epinephrine is used as vasoconstrictor so no blood loss. It is economical because it doesn’t require for any more expensive pre-operative investigations. There are no pre-operative fasting and no need for change in anticoagulant therapy. It does not require sedation, which allows the patients to communicate with the doctors during the procedure and perform active movement of the operated limb to examine if there is an impingement of implants. There was no need for various pre-operative examinations, intraoperative monitoring, post-operative anesthesia recovery room care, and also patient would be free from the side effects of opiates or sedation. We did not observe any complications such as implant failure or infection in our study. This technique might be a useful alternative to the traditional anesthetic technique in distal radius fracture fixation, especially in patients with comorbidities or when an anesthesiologist is not available.
With WALANT surgery, patients do not require numerous pre-operative investigations, specialists who monitor intraoperative status, post-operative anesthesia recovery rooms, and any drug-related adverse effects. As a patient is fully awake during the procedure, limb movements can be carried out to ensure proper implant positioning and avoid any impingement.
References
- 1.Lalonde D. Wide awake local anaesthesia no tourniquet technique (WALANT). BMC Proc 2015;9:A81. [Google Scholar | PubMed]
- 2.Lalonde D, Eaton C, Amadio P, Jupiter J. Wide-awake hand and wrist surgery: A new horizon in outpatient surgery. Instr Course Lect 2015;64:249-59. [Google Scholar | PubMed]
- 3.Pogue DJ, Vegas SF, Patterson RM, Peterson PD, Jenkins DK, Sweo TD, et al. Effects of distal radius fracture malunion on wrist joint mechanics. J Hand Surg Am 1990;15:721-7. [Google Scholar | PubMed]
- 4.Specjalski K, Kita-Milczarska K, Jassem E. The negative predictive value of typing safe local anesthetics. Int Arch Allergy Immunol 2013;162:86-8. [Google Scholar | PubMed]
- 5.Hutchinson DT, McClinton MA. Upper extremity tourniquet tolerance. J Hand Surg Am 1993;18:206-10. [Google Scholar | PubMed]
- 6.Maury AC, Roy WS. A prospective, randomized, controlled trial of forearm versus upper arm tourniquet tolerance. J Hand Surg Br 2002;27:359-60. [Google Scholar | PubMed]
- 7.Minto G, Biccard B. Assessment of the high-risk perioperative patient. Contin Educ Anaesth Crit Care Pain 2013;14:12-7. [Google Scholar | PubMed]
- 8.Horacek M, Vymazal T. Lidocaine not so innocent: Cardiotoxicity after topical anaesthesia for bronchoscopy. Indian J Anaesth 2012;56:95-6. [Google Scholar | PubMed]
- 9.Ruxasagulwong S, Kraisarin J, Sananpanich K. Wide awake technique versus local anesthesia with tourniquet application for minor orthopedic hand surgery: A prospective clinical trial. J Med Assoc Thai 2015;98:106-10. [Google Scholar | PubMed]
- 10.Younge D. Haematoma block for fractures of the wrist: A cause of compartment syndrome. J Hand Surg Br 1989;14:194-5. [Google Scholar | PubMed]
- 11.Ki Lee S, Gul Kim S, Sik Choy W. A randomized controlled trial of minor hand surgeries comparing wide awake local anesthesia no tourniquet and local anesthesia with tourniquet. Orthop Traumatol Surg Res 2020;106:1645-51. [Google Scholar | PubMed]
- 12.Moscato L, Laborde A, Kouyoumdjian P, Coulomb R, Mares O. Trapeziometacarpal (TMC) arthroplasty under Wide Awake local anesthesia with no tourniquet (WALANT) versus local anesthesia with peripheral nerve blocks (LAPNV): perioperative pain and early functional results in 30 patients. Hand Surg Rehabil 2021;40:453-7. [Google Scholar | PubMed]
- 13.Ingall EM, Bernstein DN, Shoji MM, Merchan N, Harper CM, Rozental TD. Using the quick DASH to model clinical recovery trajectory after operative management of distal radius fracture. J Hand Surg Glob Online 2020;3:1-6. Erratum in: J Hand Surg Glob Online 2021;3:316. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Beneath the Surface: Prophylactic Carpal Tunnel Release Cuts Carpal Tunnel Syndrome Risk Post Volar Plating
October 1, 2025 Beneath the Surface: Prophylactic Carpal Tunnel Release Cuts Carpal Tunnel Syndrome Risk Post Volar Plating October 1, 2025 Femoral Stem Subsidence Rate with Cementless Stems in Patients with Sub-capital Femoral Neck Fractures: Relationship to Proximal Femoral Geometry
October 1, 2025 Femoral Stem Subsidence Rate with Cementless Stems in Patients with Sub-capital Femoral Neck Fractures: Relationship to Proximal Femoral Geometry November 1, 2024 Hematoma Block as an Alternate Mode of Anesthesia for Management of Extra-Articular Distal End Radius Fracture with Percutaneous K-Wire Fixation in Emergency Department
November 1, 2024 Hematoma Block as an Alternate Mode of Anesthesia for Management of Extra-Articular Distal End Radius Fracture with Percutaneous K-Wire Fixation in Emergency Department May 10, 2020 Journal of Orthopaedic Case Reports 2020 May – June | Volume 10 | Issue 3
May 10, 2020 Journal of Orthopaedic Case Reports 2020 May – June | Volume 10 | Issue 3