
Enchondroma of carpal bones such as triquetrum and pisiform is a rare entity and requires a high index of suspicion. Extended curettage should be done whenever it is painful and restricting the range of motion.
Dr. Saumya Agarwal, 16 D, Old Fatehpura, Near Seva Mandir, Udaipur - 313 001, Rajasthan, India. E-mail: saumyathecalyx.agarwal@gmail.com
Abstract
Introduction: Enchondroma is a cartilaginous benign tumor of bone with the most common involvement of tubular bones of hands and feet. The triquetrum and pisiform are carpal bones and the enchondroma of the triquetrum and pisiform has not been reported in the literature to the best of our knowledge.
Case Report: A 26-year-old male presented with swelling over his right wrist with painful terminal motion. Based on magnetic resonance imaging findings, diagnosis of enchondroma of triquetrum and pisiform was made. Bone excision and curettage were performed, and histopathology confirmed the diagnosis. After 2 years of follow-up, the patient has gained pain-free wrist movements post excision, and there are no signs of recurrence. The Modified Mayo Wrist Score of 75 (fair) improved to 100 (excellent).
Conclusion: The surgeon should always keep in mind the possibility of a tumor at the rare site and accurately diagnose the tumor with the help of imaging modalities and biopsy.
Keywords: Enchondroma, triquetrum, pisiform, bone tumor, carpal.
Enchondroma is a common benign cartilaginous tumor that typically grows within the medullary cavity, particularly in the phalanges, metacarpals, and metatarsals [1]. However, its occurrence in carpal bones is rare, with only a few reported cases in the literature. Enchondromas are often incidentally discovered on radiography performed for unrelated reasons or following a pathologic fracture. Radiographically, enchondromas present as round, transparent osteolytic bony changes [2]. While they are generally asymptomatic, they may enlarge over time [3]. However, despite potential enlargement, the cortical margin of the involved bone remains intact, and there is no invasion into surrounding tissues [2]. In this report, we present a rare case of enchondroma involving the triquetrum and pisiform bones, presenting as chronic wrist pain. This case underscores the importance of considering rare causes of wrist pain, such as enchondromas, particularly when evaluating patients with carpal bone involvement. Early recognition and appropriate management are essential for optimal outcomes in such cases.
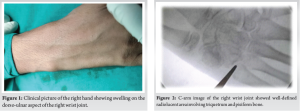
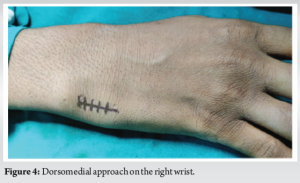
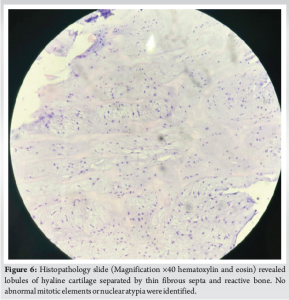
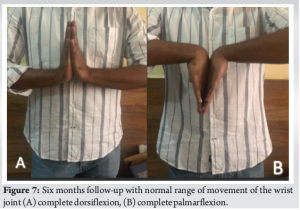
We present a case of a 26-year-old student who came to the orthopedics outdoor patient department with a complaint of pain and swelling at the dorsum of the right wrist joint for 1 year while playing. The pain was insidious in onset and progressive in nature. There was no reported history of previous trauma or infection. There was no history of loss of appetite, loss of weight, loss of sleep, and night sweats. Clinical examination revealed moderate swelling on the dorso-ulnar aspect of the right wrist joint (Fig. 1), with terminal painful motion, and decreased grip strength. On local examination, a swelling was found, which was of 2 × 1 cm in size, hard, non-fluctuant, not mobile, was attached to the underlying bone, non-tender, with normal skin without any neurovascular deficit. Ulnar deviation of the left wrist was found to be painful. All the laboratory investigations were within normal limits. C-arm image of the right wrist joint showed well defined radiolucent area involving triquetrum and pisiform bone (Fig. 2). Magnetic resonance imaging (MRI) scan shows hypointense signal in T1 weighted images and hyperintense signal in T2-weighted images on Triquetrum and pisiform bone of the right wrist and did not involve any soft tissue. The other bones of the carpus were of homogeneous density and normal in shape (Fig. 3). Informed consent was taken. The patient was operated under a supraclavicular block through a dorsomedial approach (Fig. 4). After careful dissection the triquetrum and pisiform were exposed and the lesion was identified. The lesion was meticulously curetted (Fig. 5) and for confirmation, a specimen was sent for histopathological examination. The Void was not filled with any graft. The capsular complex was well repaired. The diagnosis was confirmed by histological study after biopsy (Fig. 6). The arm was immobilized for 6 weeks in a long cast with the wrist in slight dorsiflexion. Histology showed small fragments of bone and ossifying cartilage in a reactive fibroblastic connective tissue stroma, consistent with an enchondroma. The patient improved symptomatically in 2 months with a normal range of movement at the wrist joint at around 6 months (Fig. 7). After a follow-up of 2 years, the patient remained asymptomatic with a wrist motion at 60° of flexion and 45° of extension and an arc of 30° for radioulnar deviation and radiographic study revealed no recurrence of the enchondroma.


Enchondromas are benign, slow-growing hyaline cartilage tumors most often found in the hands, representing the most common primary bone tumors of the hand [4,5]. These lesions typically develop in the third and fourth decades of life and tend to affect the ulnar-sided tubular bones [2,6], with the proximal phalanges being the most frequently affected, followed by the middle phalanges, metacarpals, and distal phalanges [7]. Carpal bone involvement is less common, accounting for approximately 1–3% of all hand and wrist enchondromas [2,6]. The scaphoid is the most common site of carpal enchondroma, and it typically remains minimally or asymptomatic until a pathologic fracture occurs [8]. These tumors are believed to arise from the proliferation of physeal remnants entrapped within the medullary canal [9]. Takigawa [2] reported 110 cases of hand enchondromas, with only 2 cases involving the carpal bones (scaphoid, lunate). Emecheta et al. [10] reported only three enchondromas in a series of 86 treated carpal bone lesions. A multidisciplinary approach that integrates surgical, radiographic, and histopathologic findings is useful in diagnosing bone tumors, especially hand enchondromas. Enchondroma of the hand is unique because it may exhibit hypercellularity and cytologic atypia, characteristics generally consistent with chondrosarcoma in long bones. Although, surgical curettage of enchondromas typically yields favorable outcomes and low complication rates, controversy exists regarding immediate versus delayed treatment of pathologic fractures, the role of surgical adjuncts after curettage, and the role and effect of void fillers [11]. Rustagi et al. presented a rare case of chondroblastoma pisiform, which should also raise a high index of suspicion among surgeons[12]. While many cases of enchondroma are discovered incidentally, the most common presenting signs and symptoms are nonspecific and include pain, swelling, and deformity. Multiple enchondromatosis syndromes are rare, and most patients present with a solitary enchondroma [2,4]. A solitary painless enchondroma may be observed. In the long bones, enchondromas are commonly located in the metaphysis, but in the tubular bones of the hand, they can be found in the metaphysis, diaphysis, or epiphysis or can span the entire phalanx [11]. Heterozygous mutations in the isocitrate dehydrogenase 1 and 2 genes have been detected in patients with solitary enchondroma, periosteal chondroma, and chondrosarcoma [13]. Malignant transformation of solitary enchondroma is very rare, and it has not been described in the carpus. The classic description of an enchondroma is a well-defined lytic lesion with stippled calcification. Although standard X-ray findings are essential in diagnosing enchondroma of the carpal bone, further investigations such as computed tomography-scan or MRI may be necessary. MRI is particularly helpful in identifying enchondroma, as it demonstrates low signal intensity on T1 sequences and high signal intensity on T2 sequences [14]. Based on histopathology, the characteristic microscopic features of enchondroma include a well-demarcated, relatively hypocellular specimen with darkly staining, lacunae-bound chondrocytes embedded in a cartilaginous matrix [11]. Intralesional curettage is the mainstay of treatment and is performed with variably sized and shaped curettes until the lesion has been completely evacuated. The tumor typically has a spongy, friable consistency. Overly aggressive curettage, especially in lesions with a thin, weakened cortical shell, can lead to an iatrogenic fracture or cortical perforation and should be avoided. The endpoint of curettage is a complete removal of the tumor under direct visualization[11]. Surgical adjuncts are often used after curettage of enchondroma to eliminate residual nests of tumor cells and theoretically decrease the likelihood of recurrence. The generated void may be filled or left vacant to fill in naturally with hematoma [15]. Proponents of void augmentation contend that defect filling may provide early structural support (in the case of bone cement) or an osteoconductive environment that could hasten bone healing and decrease post-operative fractures and recurrence. Advocates of curettage alone, on the other hand, argue that augmentation is unnecessary to prevent post-operative fractures or recurrence, risks donor-site morbidity when an autograft is used, adds surgical time and expense, and risks introducing foreign materials and transmitting disease when synthetic materials and allografts are used, respectively [11]. A retrospective review of 24 patients treated in this manner with a mean follow-up of 26 months revealed no post-operative fractures [16]. The post-operative rehabilitation protocol depends on the strength of the curetted bone or fixation construct and the patient’s demands and anticipated compliance. The most frequent complications after surgery are stiffness, contractures, and joint deformities, which generally do not require additional surgical treatment [7]. Enchondroma has been reported to be difficult to differentiate from low-grade chondrosarcoma by radiology [17]. Surgical removal of enchondroma is necessary because it will establish an accurate histopathologic diagnosis, free the patient of clinical symptoms, and strengthen the mechanical stability of the involved bone[18].
Enchondromas are most commonly found in the short tubular bones, especially phalanges, metacarpals, and metatarsals, but the atypical presentation is a possibility, therefore surgeon should always keep in mind the possibility of the tumor and accurately diagnose the tumor with the help of imaging modalities and biopsy. Most of the cases are asymptomatic and are advised conservative treatment but in patients with painful swelling and restricted joint movement with or without neurovascular deficit, extraperiosteal bony excision remains the mainstay of the treatment.
Enchondroma although common in tubular bones but involvement of triquetrum and pisiform has not been reported in the literature, and this demands high clinical suspicion and radiological and histopathological confirmation. Bone excision and curettage are required when the lesion is symptomatic with pain, restriction of movement, or any neurological deficit.
References
- 1.Ali SM, Sofien B, Feten S, Khaled B, Riadh M. Enchondroma of the scaphoid: A case report. Pan Afr Med J 2015;21:133. [Google Scholar | PubMed]
- 2.Takigawa K. Chondroma of the bones of the hand. A review of 110 cases. J Bone Joint Surg Am 1971;53:1591-600. [Google Scholar | PubMed]
- 3.Takka S, Poyraz A. Enchondroma of the scaphoid bone. Arch Orthop Trauma Surg 2002;122:369-70. [Google Scholar | PubMed]
- 4.Unni KK, Inwards CY. Chondroma in Dahlin’s bone tumors. 6th ed. Philadelphia, PA: Wolters Kluwer/Lippincott Williams and Wilkins; 2010. p. 22-40. [Google Scholar | PubMed]
- 5.Simon MJ, Pogoda P, Hövelborn F, Krause M, Zustin J, Amling M, et al. Incidence, histopathologic analysis and distribution of tumours of the hand. BMC Musculoskelet Disord 2014;15:182. [Google Scholar | PubMed]
- 6.Gaulke R. The distribution of solitary enchondromata at the hand. J Hand Surg Br 2002;27:444-5. [Google Scholar | PubMed]
- 7.Sassoon AA, Fitz-Gibbon PD, Harmsen WS, Moran SL. Enchondromas of the hand: Factors affecting recurrence, healing, motion, and malignant transformation. J Hand Surg Am 2012;37:1229-34. [Google Scholar | PubMed]
- 8.El Mrini A, Daoudi A, Loudyi D, Boutayeb F, Agoumi O, El Yaacoubi M. Scaphoid enchondroma revealed by a fracture. Chir Main 2006;25:103-5. [Google Scholar | PubMed]
- 9.Milgram JW. The origins of osteochondromas and enchondromas: A histopathologic study. Clin Orthop Relat Res 1983;174:264-84. [Google Scholar | PubMed]
- 10.Emecheta IE, Bernhards J, Berger A. Carpal enchondroma. J Hand Surg 1997;22:817-9. [Google Scholar | PubMed]
- 11.Lubahn JD, Bachoura A. Enchondroma of the hand. J Am Acad Orthop Surg 2016;24:625-33. [Google Scholar | PubMed]
- 12.Rustagi A, Agarwal S, Khanna G, Krishna LG, Talwar J, Prakash S. A rare case report of chondroblastoma pisiform in adolescent. J Orthop Case Rep 2020;10:9-13. [Google Scholar | PubMed]
- 13.Pansuriya TC, van Eijk R, d’Adamo P, van Ruler MA, Kuijjer ML, Oosting J, et al. Somatic mosaic IDH1 and IDH2 mutations are associated with enchondroma and spindle cell hemangioma in Ollier disease and Maffucci syndrome. Nat Genet 2011;43:1256-61. [Google Scholar | PubMed]
- 14.Douis H, Saifuddin A. The imaging of cartilaginous bone tumours I: Benign lesions. Skeletal Radiol 2012;41:1195-212. [Google Scholar | PubMed]
- 15.Tordai P, Hoglund M, Lugnegård H. Is the treatment of enchondroma in the hand by simple curettage a rewarding method? J Hand Surg Br 1990;15:331-4. [Google Scholar | PubMed]
- 16.Bachoura A, Rice IS, Lubahn AR, Lubahn JD. The surgical management of hand enchondroma without post-curettage void augmentation: Authors’ experience and a systematic review. Hand (N Y) 2015;10:461-71. [Google Scholar | PubMed]
- 17.Nelson DL, Abdul-Karim FW, Carter JR, Makley JT. Chondrosarcoma of small bones of the hand arising from enchondroma. J Hand Surg Am 1990;15:655-9. [Google Scholar | PubMed]
- 18.Kim CH. Enchondroma of the lunate. Arch Plast Surg 2012;39:678-80. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report
August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report
July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report
July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report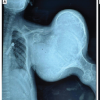 July 1, 2026 Severe Deforming Ollier Disease with a Giant Proximal Humeral Benign Chondroid Lesion in an Adolescent Male: Case Report
July 1, 2026 Severe Deforming Ollier Disease with a Giant Proximal Humeral Benign Chondroid Lesion in an Adolescent Male: Case Report