
Surgical management of snapping quadriceps caused by distal femur osteochondroma requires tailored intervention, guided by detailed imaging to ensure accurate diagnosis and effective treatment.
Dr. Madhan Jeyaraman, Department of Orthopaedics, ACS Medical College and Hospital, Dr. MGR Educational and Research Institute, Chennai, Tamil Nadu, India. E-mail: madhanjeyaraman@gmail.com
Abstract
Introduction: Osteochondromas, common benign bone tumors, can lead to complications such as snapping quadriceps when located near joints such as the knee. This case report discusses a rare instance of a distal femur osteochondroma causing a snapping sensation during knee movement. The pathogenesis involves the tumor altering the normal mechanics of the quadriceps tendon, necessitating a comprehensive diagnostic approach including magnetic resonance imaging and dynamic ultrasound.
Case Report: We report a 37-year-old male who presented with a 6-month history of progressive pain, swelling, and a snapping sensation in the right knee, which was confirmed as a pedunculated osteochondroma with a cartilage cap <2 cm in thickness with appropriate investigations. Due to failed conservative management, the surgical resection through the Swashbuckler approach was performed.
Conclusion: The case emphasizes the importance of precise diagnostic imaging and tailored surgical intervention in managing uncommon mechanical complications of osteochondromas.
Keywords: Osteochondroma, snapping quadriceps, distal femur, surgical resection, swashbuckler approach, knee biomechanics.
Osteochondromas are the most common benign bone tumors, often presenting as painless, palpable masses. While generally asymptomatic, these tumors can cause complications when located near joints, such as the knee. The proximity to the knee can lead to mechanical symptoms, including discomfort and limited mobility, particularly when involving the distal femur. A rare but significant complication in this context is snapping quadriceps, a condition marked by a palpable or audible snap during knee movements, caused by the quadriceps tendon or muscle sliding over a bony prominence such as an osteochondroma [1,2]. This report discusses a case of snapping quadriceps associated with a distal femur osteochondroma, emphasizing the rarity and mechanical implications of this condition. The pathogenesis of snapping quadriceps involves the abnormal protrusion of the osteochondroma, disrupting the normal gliding mechanism of the quadriceps tendon across the femur. This mechanical disruption results in a snapping sensation that is particularly noticeable during repetitive knee movements. Previous literature has highlighted various presentations of osteochondromas around the knee but has infrequently documented cases where these tumors lead to snapping quadriceps, underlining the unusual nature of this case. Diagnostic approaches typically include patient history, physical examination, and imaging studies such as magnetic resonance imaging (MRI) and dynamic ultrasound, which are crucial for confirming the mechanical interaction between the osteochondroma and the quadriceps tendon. Although osteochondromas are widely reported in orthopedic literature due to their commonality, the specific presentation involving snapping symptoms caused by these tumors remains scarcely discussed. The snapping phenomenon typically emerges from the mechanical interaction where the osteochondroma alters the local anatomy, imposing a physical barrier that affects the normal function of musculotendinous structures. In the case of the distal femur, the strategic position of the osteochondroma may directly engage with the quadriceps tendon, an interaction that is not typically observed in standard presentations of knee joint osteochondromas. The rarity of snapping quadriceps secondary to osteochondromas near the knee joint is notable [3,4], as most literature focuses on more common complications such as pain, fracture, and malignant transformation. The unusual mechanical relationship in our case adds a unique challenge for diagnosis and management, distinguishing it from typical presentations of osteochondromas, which are often addressed with observation or straightforward surgical excision when symptomatic. Given the scarcity of similar cases, this report contributes to the limited pool of documented instances where osteochondromas lead to dynamic mechanical symptoms such as snapping. This reinforces the necessity for a thorough diagnostic evaluation, combining both static and dynamic imaging techniques to accurately depict the interaction between the bony tumor and the moving tendinous structures. Understanding such rare presentations can aid clinicians in diagnosing similar cases more effectively, advocating for an individualized approach to treatment that may vary significantly from the typical management strategies employed for osteochondromas.
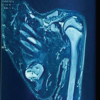
A 37-year-old male presented with a 6-month history of progressive pain and swelling in the right knee. The patient had no significant medical history and reported that the pain, initially mild and intermittent, had become more severe and constant, particularly with physical activity. In addition, he experienced a snapping sensation in the quadriceps region during knee movement. There was no history of trauma. On physical examination, a firm, non-tender mass was palpated on the distal aspect of the right femur, with no overlying skin changes or vascular compromise. The mild wasting of the quadriceps was also present. The range of motion in the knee was slightly reduced due to discomfort, and snapping of the quadriceps was noted during flexion and extension. However, there were no signs of neurovascular impairment or infection. Initial diagnostic imaging included plain radiographs of the distal femur, which revealed a pedunculated bony outgrowth emanating from the metaphyseal region, consistent with an osteochondroma (Fig. 1). To further evaluate the lesion, an MRI was performed. MRI confirmed the presence of an osteochondroma with no evidence of malignant transformation. The cartilage cap measured <2 cm, which is typically associated with a benign nature. The MRI also showed the lesion’s relationship to surrounding structures, ensuring there was no involvement of critical neurovascular bundles.

Given the progressive symptomatic nature of the tumor and potential complications such as a fracture or neurovascular compression, surgical resection was elected. The Modified swashbuckler approach used without arthrotomy of the knee was chosen for its excellent exposure of the distal femur. This approach involved an anterolateral incision, which allows for extensive visualization of the femur while preserving the integrity of the quadriceps muscle and minimizing disruption to surrounding tissues. Spinal anesthesia was administered to ensure patient comfort and optimal surgical conditions. The patient was positioned supine on the operating table with a tourniquet applied to the proximal thigh to control intraoperative bleeding. A longitudinal incision was made over the lateral aspect of the distal femur, providing direct access to the lesion. Superficial dissection was done, and the vastus lateralis muscle was identified and separated from the lateral intermuscular septum by blunt finger dissection, then the same muscle, along with the whole quadriceps, was elevated medially with the Homan retractor. Careful retraction was used to avoid damage to surrounding tissues. Distal femur exposed and bony outgrowth on the anterior aspect identified, corresponding quadriceps muscle impinged by this growth on the extension of the knee, but no tear or abnormal change present intra-operative on the contact part of the muscle. The osteochondroma was identified and meticulously excised using an extra periosteal technique to preserve the periosteum and underlying bone structure. After excision, bony margins were inspected and smoothened, and bone wax was applied to achieve hemostasis at the resection site. The resected specimen, measuring approximately 4 cm in diameter, was sent for histopathological examination. The surgical site was thoroughly irrigated to remove any debris, and the wound was closed in layers using appropriate sutures. A sterile dressing was applied to protect the incision site (Fig. 2 and 3).

Postoperatively, pain management included non-steroidal anti-inflammatory drugs (NSAIDs) and opioids as needed. Early mobilization was encouraged to prevent stiffness and promote healing, with physical therapy initiated on the first post-operative day to restore the range of motion and strength. The gross specimen consisted of a lobulated bony mass with a cartilaginous cap, typical of an osteochondroma. Histopathological examination confirmed the diagnosis, showing well-differentiated cartilaginous tissue capped with perichondrium and no evidence of malignant transformation. These findings corroborated the clinical and radiographic diagnosis, confirming the benign nature of the growth.
The patient was reviewed in the outpatient clinic at 2 weeks, 6 weeks, and 3 months postoperatively. At the 2-week follow-up, the surgical wound had healed well with no signs of infection or complications (Fig. 4). By the 6-week follow-up, the patient had regained a full range of motion in the knee and reported significant pain relief. At the 3-month follow-up, there was no recurrence of the lesion on imaging studies, and the patient had returned to normal activities without restrictions.
Snapping phenomena, whether involving the hip or quadriceps, typically present with audible or palpable snaps during limb movement. It can be classified into three primary categories: External, internal, and intra-articular. External snapping hip typically involves the iliotibial band or the gluteus maximus tendon snapping over the greater trochanter [5,6]. Internal snapping hip is most frequently associated with the iliopsoas tendon snapping over the iliopectineal eminence or the anterior aspect of the hip joint capsule [7,8]. Intra-articular causes include labral tears, loose bodies, and other internal joint abnormalities [1,9]. Osteochondromas, the most common benign bone tumors, protrude from the bone surface and are capped with cartilage. They generally originate from displaced cartilaginous cells near the growth plate and are often regarded as developmental lesions. In the knee, particularly the distal femur, osteochondromas can disrupt joint biomechanics by altering the trajectory or tension of tendons and muscles. This disruption can cause a snapping sensation, such as when the quadriceps muscle moves over the osteochondroma, as observed in our case report. Recent case reports have identified less common causes, such as calcific tendinitis of the rectus femoris and bifid iliopsoas tendon. Calcific tendinitis can lead to painful snapping due to impingement between the calcified tendon and the iliacus muscle [10]. Similarly, the bifid iliopsoas tendon, where the tendon splits into two parts, can result in persistent snapping even after surgical intervention if not all tendinous parts are released [8,11]. Snapping quadriceps is the term used to describe a distinct palpable or audible event generated by the abrupt movement of the quadriceps muscle or its tendon during knee joint motion. Osteochondromas, the most common benign bone tumors, have been consistently implicated in these cases when they form in anatomically relevant areas. Although they typically arise as asymptomatic bony outgrowths near the metaphyses of long bones, such as the distal femur, mechanical interaction with the quadriceps mechanism can lead to various clinical manifestations, including snapping, entrapment, or even a locked knee. One illustrative case is that of a 45-year-old female reported by Sadiq et al. (2007), who arrived at the emergency department with a locked right knee fixed at 30° of flexion, absent any history of trauma. Radiographs exposed a lesion on her distal femur, whereas MRI clarified a well-defined osteochondroma that displaced the vastus medialis and effectively “hooked” the quadriceps muscle around the bony outgrowth. Open surgical removal of the lesion fully restored her range of motion, underscoring the importance of direct tumor-muscle impingement in causing snapping and locking [12]. Meanwhile, Jung et al. (2015) described a 16-year-old with internal snapping of the hip linked to an osteochondroma on the posteromedial femoral neck. Despite the primary complaint centering around inguinal pain and a pincer-type femoroacetabular impingement, the lesion’s location led to repetitive friction with the iliopsoas tendon. Arthroscopic resection resolved symptoms completely, demonstrating that osteochondromas can cause extra-articular snapping at anatomically remote sites and potentially alter gait or stress patterns affecting the quadriceps mechanism [13]. A related but distinct phenomenon emerged in Song et al. (2019), who documented a 56-year-old patient with a snapping sensation localized to the medial femoral condyle 10 years after a total knee arthroplasty (TKA). Notably, no tumor was seen until 5 years post-TKA, and then progressively enlarged, ultimately impinging on the sartorius tendon from 40° to 20° of passive knee extension. Surgical excision of the now 3 × 3 × 2.5 cm osteochondroma effectively abolished snapping and improved motion, raising the important consideration that altered biomechanics or stress distribution after joint arthroplasty may predispose to new or progressive osteochondroma formation [14]. Chen et al. (2022) provided a broader perspective, analyzing 74 patients undergoing arthroscopic resection of extra-articular knee osteochondromas – 26 at the distal femur and 48 at the proximal tibia. This minimally invasive technique yielded significant improvement in pain (as measured by the Visual Analog Scale), knee function (Lysholm and International Knee Documentation Committee scores), and motor function (Tegner scores), with no recurrences or complications. Their results highlight arthroscopy’s precision and reduced morbidity, particularly for extra-articular lesions near the knee [15]. Beyond natural etiologies, iatrogenic causes can also provoke quadriceps snapping, as shown by Ashy et al. (2024). Two patients developed painful lateral snapping in the quadriceps tendon after a partial-thickness harvest for anterior cruciate ligament reconstruction. Correcting the previous harvest defect through imbrication successfully resolved snapping in both cases. Taken together, these experiences underscore that meticulous imaging, careful surgical planning, and complete lesion removal or tendon repair are paramount. When appropriately addressed – be it through open or arthroscopic resection – most patients achieve full recovery and minimal recurrence risk, reinforcing the importance of early recognition and precisely tailored treatment for snapping quadriceps [16]. Patients with snapping hip syndrome often present with a characteristic snapping or clicking sensation during hip movements. This sensation can be painless or associated with discomfort and pain, particularly when it becomes chronic [17]. The snapping is typically most noticeable during activities that involve flexion and extension of the hip, such as running, climbing stairs, or rising from a seated position [17]. Physical examination usually reveals reproducible snapping with certain movements. Internal snapping of the hip might involve the patient actively moving from a position of hip flexion, abduction, and external rotation to extension and internal rotation [7,11]. The snapping can often be palpated and sometimes heard. Imaging plays a crucial role in diagnosing snapping hip syndrome and identifying its underlying cause. Standard radiographs are typically unremarkable in cases of internal snapping hip but can help rule out bony abnormalities or other intra-articular pathology. Ultrasound and MRI are more sensitive in detecting soft-tissue abnormalities such as tendinopathy or calcific deposits. Dynamic ultrasonography, in particular, allows for real-time observation of the snapping phenomenon and is useful in assessing tendon movement relative to bony structures [7]. In cases of calcific tendinitis, computed tomography (CT) scans can precisely localize calcific deposits and guide therapeutic injections. MRI may show thickening and edema of tendons, but can sometimes miss calcific deposits unless they are significant. For diagnosing a bifid iliopsoas tendon, both MRI and intraoperative findings are critical, as the anomaly may not be evident on pre-operative imaging [11]. The management of snapping hip syndrome varies depending on the underlying cause and severity of symptoms. Conservative treatment is the first line, including activity modification, physical therapy focusing on stretching and strengthening exercises, and NSAIDs [8]. For cases resistant to conservative measures, corticosteroid injections can provide relief, particularly in cases involving inflammation such as calcific tendinitis [8]. Surgical intervention is considered for patients who do not respond to conservative treatment. Arthroscopic iliopsoas tendon release is a common procedure for internal snapping of the hip, with a generally high success rate. However, recognizing anatomical variations such as a bifid tendon is crucial to avoid persistent symptoms postoperatively [18-20]. In cases of calcific tendinitis, CT-guided aspiration or debridement of the calcific deposit can be effective. The summary of literature evidence on the management of snapping quadriceps secondary to distal demur osteochondroma is tabulated in Table 1 and 2.


This case report illustrates a rare presentation of snapping quadriceps associated with a distal femur osteochondroma, treated successfully through surgical resection. The case emphasizes the importance of precise diagnostic imaging and tailored surgical intervention in managing uncommon mechanical complications of osteochondromas, understanding these rare presentations aids in the development of individualized treatment strategies, thereby improving patient outcomes. Our findings contribute to the limited but growing body of literature on dynamic mechanical symptoms induced by benign skeletal tumors.
Snapping quadriceps due to osteochondroma at the distal femur is a rare condition that can be effectively managed with precise surgical excision. Accurate imaging and individualized surgical approaches are critical for optimal outcomes in such uncommon presentations.
References
- 1.Musick SR, Varacallo M. Snapping hip syndrome. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar | PubMed]
- 2.Nolton EC, Ambegaonkar JP. Recognizing and managing snapping hip syndrome in dancers. Med Probl Perform Art 2018;33:286-91. [Google Scholar | PubMed]
- 3.Singh R, Jain M, Siwach R, Rohilla S, Sen R, Kaur K. Large para-articular osteochondroma of the knee joint: A case report. Acta Orthop Traumatol Turc 2012;46:139-43. [Google Scholar | PubMed]
- 4.Yoong-Leong Oh J, Tan KK, Wong YS. Snapping knee secondary to a tibial osteochondroma. Knee 2008;15:58-60. [Google Scholar | PubMed]
- 5.Andronic O, Rahm S, Fritz B, Singh S, Sutter R, Zingg PO. External snapping hip syndrome is associated with an increased femoral offset. Eur J Orthop Surg Traumatol 2022;32:1481-9. [Google Scholar | PubMed]
- 6.Randelli F, Mazzoleni MG, Fioruzzi A, Giai Via A, Calvisi V, Ayeni OR. Surgical interventions for external snapping hip syndrome. Knee Surg Sports Traumatol Arthrosc 2021;29:2386-93. [Google Scholar | PubMed]
- 7.Piechota M, Maczuch J, Skupiński J, Kukawska-Sysio K, Wawrzynek W. Internal snapping hip syndrome in dynamic ultrasonography. J Ultrason 2016;16:296-303. [Google Scholar | PubMed]
- 8.Yen YM, Lewis CL, Kim YJ. Understanding and treating the snapping hip. Sports Med Arthrosc Rev 2015;23:194-9. [Google Scholar | PubMed]
- 9.Yamamoto Y, Hamada Y, Ide T, Usui I. Arthroscopic surgery to treat intra-articular type snapping hip. Arthroscopy 2005;21:1120-5. [Google Scholar | PubMed]
- 10.Pierannunzii L, Tramontana F, Gallazzi M. Case report: Calcific tendinitis of the rectus femoris: A rare cause of snapping hip. Clin Orthop Relat Res 2010;468:2814-8. [Google Scholar | PubMed]
- 11.Shu B, Safran MR. Case report: Bifid iliopsoas tendon causing refractory internal snapping hip. Clin Orthop Relat Res 2011;469:289-93. [Google Scholar | PubMed]
- 12.Sadiq MZ, Syed T, Shah YR. Osteochondroma of distal femur as an unusual cause of locked knee. Eur J Orthop Surg Traumatol 2007;17:495-7. [Google Scholar | PubMed]
- 13.Jung HT, Hwang DS, Jeon YS, Kim PS. Arthroscopic resection of osteochondroma of hip joint associated with internal snapping: A case report. Hip Pelvis 2015;27:43-8. [Google Scholar | PubMed]
- 14.Song SJ, Bae DK, Park CH. Snapping knee due to a femoral osteochondroma after total knee arthroplasty. Knee Surg Relat Res 2019;31:147-50. [Google Scholar | PubMed]
- 15.Chen P, Shen L, Long Q, Dai W, Jiang X, Li C, et al. Clinical effect of arthroscopic resection of extra-articular knee osteochondroma. J Clin Med 2022;12:52. [Google Scholar | PubMed]
- 16.Ashy CC, Baird HB, Slone HS, Pullen WM. Snapping complication after partial-thickness quadriceps tendon autograft anterior cruciate ligament reconstruction: A report of 2 cases. JBJS Case Connect 2024;14:e24.00101. [Google Scholar | PubMed]
- 17.Walker P, Ellis E, Scofield J, Kongchum T, Sherman WF, Kaye AD. Snapping hip syndrome: A comprehensive update. Orthop Rev (Pavia) 2021;13:25088. [Google Scholar | PubMed]
- 18.Via AG, Basile A, Wainer M, Musa C, Padulo J, Mardones R. Endoscopic release of internal snapping hip: A review of literature. Muscles Ligaments Tendons J 2016;6:372-7. [Google Scholar | PubMed]
- 19.Ilizaliturri VM Jr., Villalobos FE Jr., Chaidez PA, Valero FS, Aguilera JM. Internal snapping hip syndrome: Treatment by endoscopic release of the iliopsoas tendon. Arthroscopy 2005;21:1375-80. [Google Scholar | PubMed]
- 20.Contreras ME, Dani WS, Endges WK, De Araujo LC, Berral FJ. Arthroscopic treatment of the snapping iliopsoas tendon through the central compartment of the hip: A pilot study. J Bone Joint Surg Br 2010;92:777-80. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report
August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor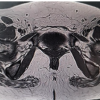 July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report