
A laparoscopic suction instrument can extract debris from the intramedullary canal of long bones.
Dr. Jonathan H Quade, Department of Orthopaedic Surgery, University of Alabama at Birmingham, Birmingham, AL, USA. E-mail: jhquade@uabmc.edu
Abstract
Introduction: The reamer-irrigator-aspirator (RIA) is safe and effective for harvesting intramedullary autograft and tissue for culture. However, mechanical complications such as reamer head dissociation with retained intramedullary debris have been previously reported.
Case Report: Techniques to remove the metallic debris have been described, but are technically challenging and inefficient. The authors provide a novel technique to aid in the removal of loose debris using a laparoscopic suction device.
Conclusion: We have utilized this instrument on multiple occasions, and it has demonstrated itself to be safe, reliable, and effective at removing all debris.
Keywords: Reamer irrigator aspirator, intramedullary canal, complications, debris.
The reamer-irrigator-aspirator (RIA) system (DePuy Synthes®, West Chester, PA) (RIA-2) is a safe and effective device for harvesting bone autograft and culture tissue from the long bones of the lower extremity [1,2,3]. The autograft acquired using RIA has been shown to be superior to iliac crest bone grafting regarding pain and volume of graft harvested and equivalent with union rates, infection, and revision procedures [4]. However, like all surgical procedures, RIA has patient-related complications that surgeons should consider. These include iatrogenic femur fractures [5], post-operative pain at the entry site [6], increased blood loss [3], as well as mechanical complications such as breakage of the drive shaft tip [7] or reamer head dissociation [8,9].
These mechanical issues can be managed using the ball-tip guidewire to extract the reamer head [7,8,9]; however, retained metal debris poses an additional challenge. Chloros et al. recently reported using curettes, graspers, and a nail extraction hook under fluoroscopy to successfully remove retained debris [10]. The authors are reporting a novel technique that the treating orthopedic trauma surgeon can use to successfully remove intramedullary debris.
Illustrative case
A 40-year-old generally healthy Hispanic male with a history of a complex right femur fracture managed at an outside facility with intramedullary nailing, subsequent corrective osteotomy, and hardware removal presented to our academic institution for further evaluation after developing chronic osteomyelitis. A computed tomography scan of the right femur demonstrated stigmata of a chronic appearing fracture deformity of the right femur with intramuscular abscesses and adjacent osteomyelitis of the femoral diaphysis. At this time, the attending surgeon elected to proceed with incision and drainage, debridement, and culture obtainment using the RIA-2 and Hemovac placement.
The RIA-2 device was expertly used to obtain intramedullary tissue samples for culture through a retrograde approach due to the residual midshaft deformity and distally located infection. Briefly, a medially parapatellar stab incision was made 4 cm distal to the inferior pole of the patella, and an entry point to the femoral canal was made. Subsequently, an entry guidewire was advanced (Fig. 1a and b), and following measurement of the canal diameter, a 10 mm diameter RIA-2 reamer head was selected. The apparatus was correctly assembled, and the device was inserted into the canal (Fig. 1c). The reamer was advanced slowly, and care was taken to ensure frequent back-and-forth movements to avoid clogging. Fluoroscopy was used to ensure eccentric reaming was avoided. Continuous reaming was carried out, but the surgeon had trouble advancing the RIA, and therefore, reaming was stopped. This is the surgeon’s usual technique to prevent the current complication, which could have been caused by incorrect assembly, clogged flutes, eccentric reaming, and stopping the reamer. A fluoroscopy image was taken, revealing the head had fragmented and dissociated from the rest of the device (Fig. 1d).
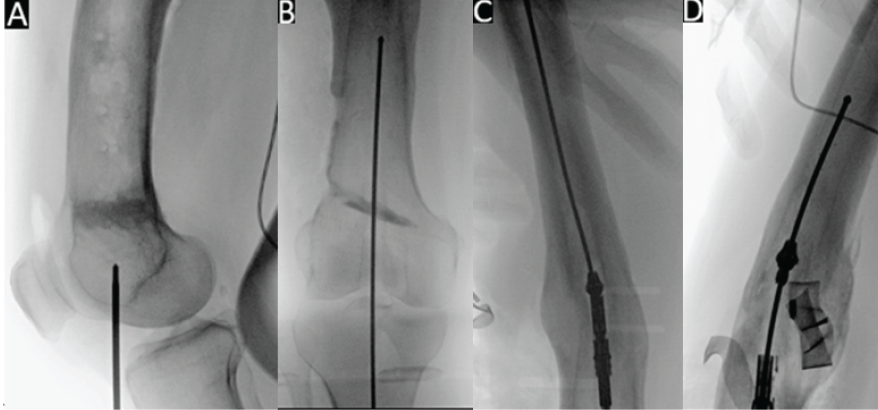
Figure 1: Fluoroscopic images of guidewire entry of femoral intramedullary canal (a), followed by advancement of the guidewire (b), then entry of the reamer-irrigator-aspirator (RIA-2) into the canal (c), and dissociation and fragmentation of the RIA-2 head (d).
Initially, the bulk of the reamer head was removed by retracting the ball-tip guide wire; however, four small metal pieces remained in the canal (Fig. 2a). Next, a removal attempt using a series of differently sized graspers was made; however, this was only partially successful and very time-consuming (Fig. 2b). Then, the idea of extracting the debris using a laparoscopic suction instrument (Stryker® Inc) (Fig. 3) under fluoroscopy was conceived and successfully put into practice (Fig. 2c). Finally, once the canal was clear (Fig. 2d), a new RIA-2 set was used, and the procedure was completed successfully. The patient was given broad-spectrum antibiotics until speciation of cultures and was allowed to weight bear as tolerated on the right lower extremity.
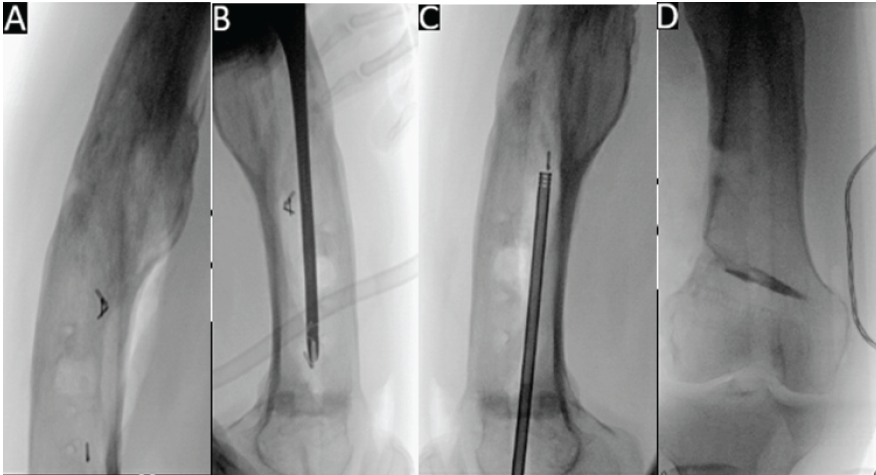
Figure 2: Fluoroscopic images of four pieces of debris remaining in the canal after extraction of the reamer-irrigator-aspirator – two head (a), followed by attempted removal of debris using pituitary grasper (b), then successful use of laparoscopic suction device to remove retained debris (c), and a clear intramedullary canal (d).
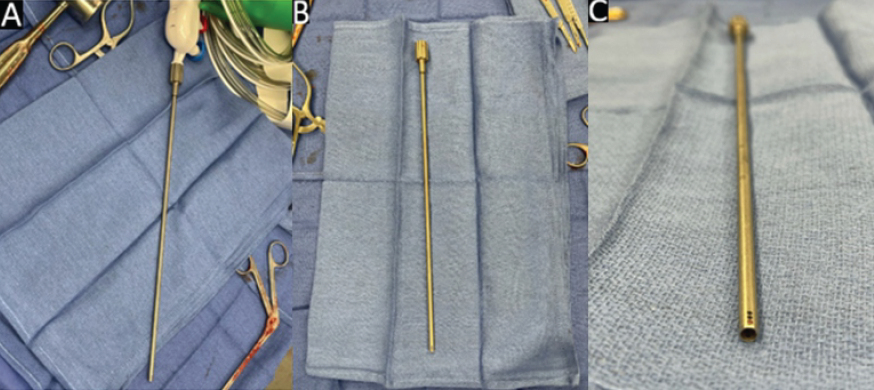
Figure 3: Stryker laparoscopic suction device attached to suction (a) and free-standing (b and c).
The RIA-2 consists of a disposable head that has been reported to dissociate or break within the intramedullary canal while reaming. While these complications are uncommon, the skilled orthopedic surgeon should be prepared to handle these situations when they do inevitably occur. In the literature reviewed, there is only one other report of metal debris persisting in the canal after extraction of the dissociated head [10]. The aim of the present surgical technique article was to describe a novel technique for the removal of intramedullary debris following RIA-2 head breakage.
All prior reports of these mechanical complications have been discussed successfully using the ball-tipped guidewire to remove the dissociated head with a single report of debris extraction using a series of curettes, graspers, and a nail extractor [7,8,9,10]. In the present case, the RIA-2 head was easily extracted using the ball-tipped guidewire as in all previous cases; however, removing the debris was more difficult. Our newly described technique using the laparoscopic suction (Stryker® Inc) device under fluoroscopy facilitated metallic debris removal, thus preventing prolonged operative time and potential complications from retained foreign bodies.
RIA-2 head dissociation and/or breakage is an uncommon complication that can occur as a result of user error or instrument malfunction. This problem can be augmented when metallic debris is left behind after head extraction. In addition to the previously reported technique using curettes, graspers, and a nail extraction hook, the present authors have demonstrated the success of laparoscopic suction for the removal of this debris. This technique has been successfully utilized at our institution on three separate occasions. Surgeons should consider using the laparoscopic suction device when presented with RIA-2 head breakage complications to aid in rapid debris clearance.
The reamer-irrigator-aspirator has been known to fracture on rare occasions, leaving behind metallic debris in the intramedullary canal of long bones. This debris is challenging to extract despite multiple prior techniques having been described. We have illustrated a novel technique that is faster and more effective than prior techniques using a laparoscopic suction device.
References
- 1.[references_numbered] 1. Madison RD, Nowotarski PJ. The reamer-irrigator-aspirator in nonunion surgery. Orthop Clin North Am 2019;50:297-304. 2. Yee MA, Hundal RS, Perdue AM, Hake ME. Autologous bone graft harvest using the reamer-irrigator-aspirator. J Orthop Trauma 2018;32 Suppl 1:S20-1. 3. Haubruck P, Ober J, Heller R, Miska M, Schmidmaier G, Tanner MC. Complications and risk management in the use of the Reaming-Irrigator-Aspirator (RIA) system: RIA is a safe and reliable method in harvesting autologous bone graft. PLoS One 2018;13:e0196051. 4. Dawson J, Kiner D, Gardner W 2nd, Swafford R, Nowotarski PJ. The reamer-irrigator-aspirator as a device for harvesting bone graft compared with iliac crest bone graft: Union rates and complications. J Orthop Trauma 2014;28:584-90. 5. Han F, Peter L, Lau ET, Thambiah J, Murphy D, Kagda FH. Reamer Irrigator Aspirator bone graft harvesting: Complications and outcomes in an Asian population. Injury 2015;46:2042-51. 6. Calori GM, Colombo M, Mazza EL, Mazzola S, Malagoli E, Mineo GV. Incidence of donor site morbidity following harvesting from the iliac crest or RIA graft. Injury 2014;45 Suppl 6:S116-20. 7. Eisenstein ED, Waterman BR, Kanlic EM, Abdelgawad AA. A new technique for obtaining bone graft in cases of distal femur nonunion: Passing a reamer/irrigator/aspirator retrograde through the nonunion site. Am J Orthop (Belle Mead NJ) 2016;45:E493-6. 8. Cipriano CA, Arvanitis LD, Virkus WW. Use of the reamer-irrigator-aspirator may reduce tumor dissemination during intramedullary fixation of malignancies. Orthopedics 2012;35:e48-52. 9. Kanakaris NK, Morell D, Gudipati S, Britten S, Giannoudis PV. Reaming Irrigator Aspirator system: Early experience of its multipurpose use. Injury 2011;42 Suppl 4:S28-34. 10. Chloros GD, Giannoudis VP, Kanakaris NK, Giannoudis PV. A technical note: How to extract broken Reamer-Irrigator-Aspirator (RIA) metal intramedullary debris. Injury 2022;53:1568-71. [/references_numbered] [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Bone Graft Harvesting Site Morbidity in Donor Area (Anterior Iliac Crest): A Retrospective Study
June 1, 2026 Bone Graft Harvesting Site Morbidity in Donor Area (Anterior Iliac Crest): A Retrospective Study December 1, 2025 Revision of Cemented Reverse Total Shoulder Arthroplasty with Bone Graft in Osteogenesis Imperfecta: A Case Report
December 1, 2025 Revision of Cemented Reverse Total Shoulder Arthroplasty with Bone Graft in Osteogenesis Imperfecta: A Case Report October 1, 2025 How Old is Too Old? Outcomes of Primary Total Knee Arthroplasty in Patients 70 Years or Older
October 1, 2025 How Old is Too Old? Outcomes of Primary Total Knee Arthroplasty in Patients 70 Years or Older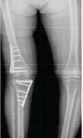 September 1, 2025 Long-term Comparison of Opening Wedge High Tibial Osteotomy and Double Level Osteotomy for Large Varus Knee Deformities: A Retrospective Cohort Study of Functional Outcomes, Complications, and Survival Rates
September 1, 2025 Long-term Comparison of Opening Wedge High Tibial Osteotomy and Double Level Osteotomy for Large Varus Knee Deformities: A Retrospective Cohort Study of Functional Outcomes, Complications, and Survival Rates