
The SCIP flap allows preservation of forefoot length in complex soft-tissue defects, preventing unnecessary bone shortening and improving functional outcomes.
Dr. Steven D M Colpaert, Department of Plastic Surgery, AZ Monica General Hospitals, Antwerp, Belgium. E-mail: steven.colpaert@azmonica.be
Abstract
Introduction: Preservation of forefoot length is crucial for gait mechanics and long-term function. However, soft-tissue defects in this region often lead to bone shortening or amputation. The superficial circumflex iliac artery perforator (SCIP) flap offers a thin and reliable reconstructive option with minimal donor-site morbidity.
Case Report: We present three patients with complex forefoot soft tissue loss in whom SCIP flaps were used for reconstruction. In all cases, the flap provided stable coverage, preserved bone length, and allowed functional recovery.
Conclusion: The SCIP flap is a valuable option in forefoot reconstruction, enabling preservation of viable structures while maintaining good functional and esthetic outcomes.
Keywords: Superficial circumflex iliac artery perforator flap, forefoot reconstruction, soft-tissue defect, microsurgery, and foot trauma.
Complex forefoot trauma remains poorly documented in literature. We present 3 case reports of forefoot injuries with tissue loss, in which the superficial circumflex iliac artery perforator (SCIP) flap was used for reconstruction. Based on these case reports, we illustrate the value of this flap for this type of injury.
Case 1
A 27-year-old male patient was referred with infection and necrosis of the skin after a right hallux valgus correction. Osteosynthesis material was already removed, leaving the osteotomy site at the first proximal phalanx, the extensor tendons, and the first metatarsophalangeal joint exposed. As osteomyelitis of the osteotomy site could not be excluded, a filleted toe flap was considered initially. After clinical evaluation and discussion with the patient, debridement, K-pin fixation, and coverage with a SCIP flap were chosen. Healing of the flap and donor site was uneventful. Bone healing and joint function were completely restored. Despite some bulkiness of the flap, the patient could wear normal shoes and declined flap thinning (Fig. 1).

Figure 1: A 27-year-old male patient with skin necrosis after hallux valgus correction. Before, immediately after, and long-term results after K-pin fixation and superficial circumflex iliac artery perforator flap coverage.
Case 2
A 19-year-old male patient sustained a crush injury with partial degloving of his right toes and forefoot. At the time of the referral, there was dry necrosis extending from digit 1 through digit 4. There was insufficient skin available for primary closure. A SCIP flap provided coverage of the metatarsal heads, preventing further shortening and preserving full functionality (Fig. 2).

Figure 2: A 19-year-old male patient with a crush injury accompanied by a partial degloving of his right toes and forefoot. Before, immediately after, and long-term results after superficial circumflex iliac artery perforator flap coverage.
Case 3
A 16-year-old boy presented with multiple fractures and partial degloving after a truck drove over his foot. There was full-thickness necrosis of digit 3 through digit 5. As in case 2, a SCIP flap provided wound closure without additional bone shortening. The flap and underlying metatarsal fractures healed uneventfully. The patient regained full function and ambulates with normal footwear (Fig. 3).
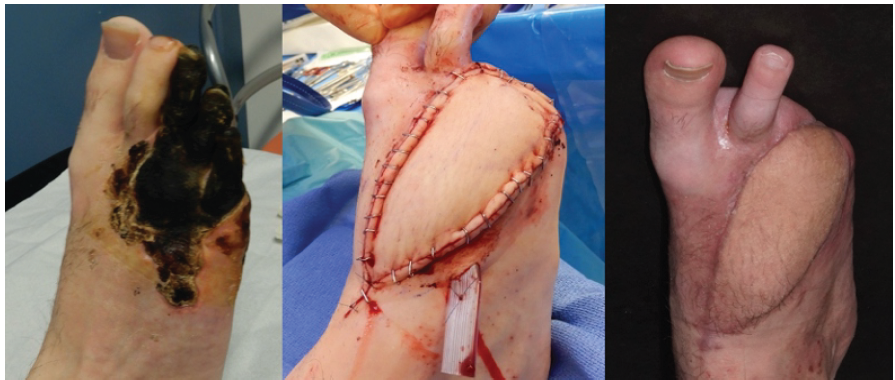
Figure 3: A 16-year-old boy with multiple fractures and partial deglovement after a truck drove over his foot. Before, immediately after, and long-term results after superficial circumflex iliac artery perforator flap coverage.
It is well documented that maintaining the length of the forefoot, including maximum preservation of the metatarsal bones, is crucial for maintaining optimal gait mechanics, load distribution, and shoe compatibility. Loss of length can lead to reduced propulsion, abnormal pressure points, and secondary deformities, which can ultimately affect long-term function and patient satisfaction. In patients with soft-tissue loss, the filleted toe flap and Lisfranc amputation are the prevalent treatment options for wound closure. These procedures often sacrifice viable bone through bone shortening. No other local flap options have proven reliable in the forefoot, making free flaps the method of choice if bone and tendon coverage is pursued. The decision whether to amputate or reconstruct is a collective decision between the surgeon and the patient. However, no data exist to guide this decision-making [1,2]. Partial foot amputation has many long-term complications and needs to be avoided whenever possible [3,4]. Traditional free skin flaps, such as the radial forearm flap, have a longer and larger vascular pedicle but are bulkier and have an unfavorable donor site. The free SCIP flap has evolved from the free groin flap, reducing its donor site morbidity and providing a thinner flap with a longer pedicle [5,6]. After its description in 2004 by Koshima, it has quickly gained popularity, with some authors advocating its use in lower extremity reconstruction [7,8,9,10]. Dissection of the flap is well described in the literature and is beyond the scope of this article. We have recently adopted the medial to lateral dissection approach as propagated by Hong [10]. Although counterintuitive, we have found this approach to improve the ease of dissection. The donor site of the SCIP flap could be closed primarily in all cases. The donor site scar is hidden in underwear and swimwear, which makes it exceptionally advantageous (Fig. 4). The diameter of the superficial circumflex iliac artery and veins provides a good match for the dorsalis pedis artery and the ample veins of the dorsal foot (Fig. 5).

Figure 4: The donor site of the superficial circumflex iliac artery perforator flap could be closed primarily in all cases.
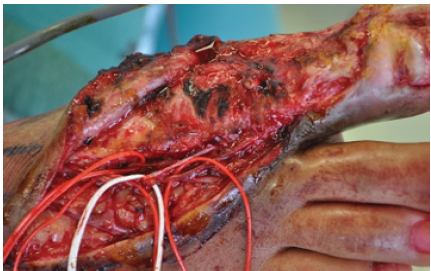
Figure 5: The diameter of the superficial circumflex iliac artery and veins provides a good match for the dorsalis pedis artery and the ample veins of the dorsal foot.
Owing to its minimal donor site morbidity and thinness, the SCIP flap is a valuable reconstructive option in forefoot trauma, enabling maximal preservation of forefoot length.
In complex forefoot soft-tissue defects, preservation of metatarsal length is essential for maintaining normal gait and foot biomechanics. The SCIP flap offers thin, reliable coverage with minimal donor-site morbidity and should be considered before resorting to bone shortening or amputation.
References
- 1. Working ZM, Elliott I, Marchand LS, Jacobson LG, Presson AP, Stuart A, et al. Predictors of amputation in high-energy forefoot and midfoot injuries. Injury 2017;48:536-41. [Google Scholar] [PubMed]
- 2. MacKenzie EJ, Bosse MJ, Kellam JF, Burgess AR, Webb LX, Swiontkowski MF, et al. Characterization of patients with high-energy lower extremity trauma. J Orthop Trauma 2000;14:455-66. [Google Scholar] [PubMed]
- 3. Dillon MP, Fatone S. Deliberations about the functional benefits and complications of partial foot amputation: Do we pay heed to the purported benefits at the expense of minimizing complications? Arch Phys Med Rehabil 2013;94:1429-35. [Google Scholar] [PubMed]
- 4. Bryant RC. Forefoot amputation. Arch Surg 1980;115:889. [Google Scholar] [PubMed]
- 5. McGregor IA, Jackson IT. The groin flap. Br J Plast Surg 1972;25:3-16. [Google Scholar] [PubMed]
- 6. Myung Y, Yim S, Kim BK. A comparison of axial circumference between superficial circumflex iliac artery perforator flap and other workhorse flaps in dorsal foot reconstruction. J Plast Surg Hand Surg 2017;51:381-6. [Google Scholar] [PubMed]
- 7. Koshima I, Nanba Y, Tsutsui T, Takahashi Y, Urushibara K, Inagawa K, et al. Superficial circumflex iliac artery perforator flap for reconstruction of limb defects. Plast Reconstr Surg 2004;113:233-40. [Google Scholar] [PubMed]
- 8. Kueckelhaus M, Gebur N, Kampshoff D, Hiort M, Varnava C, Harati K, et al. Initial experience with the superficial circumflex iliac artery perforator (SCIP) flap for extremity reconstruction in Caucasians. J Plast Reconstr Aesthet Surg 2022;75:118-24. [Google Scholar] [PubMed]
- 9. Barnhill CW, Greyson MA, Iorio ML. Superficial circumflex iliac artery perforator flap reconstruction of the upper extremity. Hand Clin 2024;40:179-87. [Google Scholar] [PubMed]
- 10. Hong JP. The superficial circumflex iliac artery perforator flap in lower extremity reconstruction. Clin Plast Surg 2021;48:225-33. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Successful Thumb Replantation Following Dog Bite Avulsion Amputation in a 2-Year-Old Child: A Case Report and Literature Review
January 1, 2026 Successful Thumb Replantation Following Dog Bite Avulsion Amputation in a 2-Year-Old Child: A Case Report and Literature Review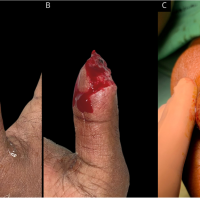 December 10, 2022 Minimally Invasive Reconstruction of an Allen Three Traumatic Thumb Injury with Platelet-rich Fibrin and Stacked Dermal Regeneration Template
December 10, 2022 Minimally Invasive Reconstruction of an Allen Three Traumatic Thumb Injury with Platelet-rich Fibrin and Stacked Dermal Regeneration Template November 1, 2024 Technical Note in Case Series a Novel Recent Technique for the Removal of Broken PFNA-II Blade in Intertrochanteric Fractures is a Technical Challenge
November 1, 2024 Technical Note in Case Series a Novel Recent Technique for the Removal of Broken PFNA-II Blade in Intertrochanteric Fractures is a Technical Challenge October 1, 2024 The effectiveness of negative pressure wound therapy in enhancing skin graft uptake on a burned lower leg stump: A case report
October 1, 2024 The effectiveness of negative pressure wound therapy in enhancing skin graft uptake on a burned lower leg stump: A case report